Tell me everything about hypertension very easy word don't miss anything tell me everything
Reading File
Finding Sources
Searching PubMed
hypertension management guidelines
Searching the Web
hypertension overview causes symptoms treatment guidelines 2025
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed to write a complete, easy-to-understand guide on hypertension. Here it is:
Everything About Hypertension - In Simple Words
1. What Is Blood Pressure?
Before understanding hypertension, you need to know what blood pressure (BP) is.
Your heart pumps blood through tubes called arteries. As blood moves, it pushes against the walls of these arteries. This pushing force is called blood pressure.
BP is written as two numbers, for example 120/80 mm Hg:
- The top number (systolic) = pressure when your heart beats and pushes blood out
- The bottom number (diastolic) = pressure when your heart rests between beats
The unit "mm Hg" means millimeters of mercury - the way we measure pressure.
What controls blood pressure? Two main things:
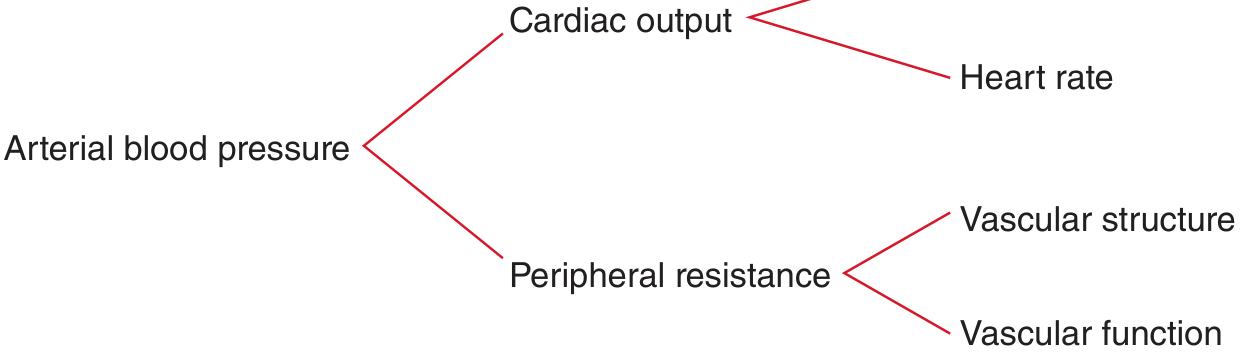
- Cardiac output - how much blood your heart pumps per minute (depends on heart rate and how forcefully it beats)
- Peripheral resistance - how narrow or stiff your blood vessels are (narrower = more resistance = higher pressure)
2. What Is Hypertension?
Hypertension = High Blood Pressure
Simply put, your heart is working too hard to push blood through your vessels, or your vessels are too stiff/narrow, or both.
Blood Pressure Categories (2025 AHA/ACC Guidelines)
| Category | Systolic (top) | Diastolic (bottom) |
|---|---|---|
| Normal | Less than 120 | Less than 80 |
| Elevated | 120-129 | Less than 80 |
| Hypertension Stage 1 | 130-139 | 80-89 |
| Hypertension Stage 2 | 140 or higher | 90 or higher |
| Hypertensive Crisis | Higher than 180 | Higher than 120 |
So hypertension is diagnosed when BP is consistently 130/80 mm Hg or higher according to current guidelines.
Note: In 2025, the AHA/ACC updated their guidelines using a new risk calculator (called PREVENT) that looks at 10-year AND 30-year cardiovascular risk to decide when to start treatment.
3. How Common Is Hypertension?
Hypertension is the most common reason people visit a doctor worldwide. It affects roughly 1 in 3 adults globally. It's often called an "iceberg disease" because:
- Only about half of people with high BP know they have it
- Of those who know, only half are treated
- Of those treated, only half are properly controlled
This means millions of people are walking around with dangerously high BP without knowing it. - Park's Textbook of Preventive and Social Medicine
4. Types of Hypertension
Type 1: Primary (Essential) Hypertension
- Most common - accounts for 90-95% of all cases
- No single clear cause found
- Caused by a combination of genetics, lifestyle, and environment
- "In 90% to 95% of adults with hypertension, the cause is unknown" - Comprehensive Clinical Nephrology
Type 2: Secondary Hypertension
- Caused by another specific disease (only about 5-10% of cases)
- Once you treat that disease, BP often improves
Common causes of secondary hypertension:
- Kidney diseases - chronic glomerulonephritis, renal artery stenosis (narrowing of the kidney artery)
- Hormonal problems:
- Primary aldosteronism (adrenal gland makes too much aldosterone hormone)
- Pheochromocytoma (a tumor in the adrenal gland)
- Cushing syndrome (too much cortisol)
- Thyroid disease
- Sleep apnea (breathing stops during sleep)
- Narrowing of the aorta (coarctation of the aorta) - more common in children
- Certain medications - birth control pills, NSAIDs (like ibuprofen), steroids, decongestants
5. What Causes Primary (Essential) Hypertension?
Even though there's no single cause, many factors raise your risk:
Lifestyle Factors
- Eating too much salt - salt makes your body hold water, raising blood volume and pressure
- Being overweight/obese - obesity alone accounts for 65-75% of primary hypertension risk
- Not exercising enough (sedentary lifestyle)
- Drinking too much alcohol
- Not eating enough potassium (potassium helps relax blood vessels)
- Smoking
- Chronic stress
Medical Factors
- Insulin resistance and diabetes - high insulin damages blood vessel walls
- High sodium intake - kidneys hold onto more sodium and water
- The Renin-Angiotensin-Aldosterone System (RAAS) becoming overactive - this is a hormonal system that regulates how much water your kidneys keep. When overactive, it raises BP.
Genetic Factors
- Hypertension runs in families
- However, no single "hypertension gene" has been found - it's a complex mix of many gene variations plus environmental triggers
6. Symptoms - The "Silent Killer"
Hypertension is called the "silent killer" because it usually has NO symptoms.
Most people feel completely normal even with dangerously high blood pressure. This is why regular BP checks are so important.
When symptoms do appear, they often mean the BP is very high or has been high for a long time:
- Headaches (especially at the back of the head, in the morning)
- Dizziness
- Blurred vision
- Shortness of breath
- Chest pain
- Nosebleeds
- Fatigue
If you get a sudden, severe headache with BP above 180/120 - this is a hypertensive emergency and needs immediate medical attention.
7. How Is Blood Pressure Measured?
Using a blood pressure cuff (sphygmomanometer):
For accurate readings:
- Sit quietly for 5 minutes before measurement
- Sit with your back supported, feet flat on the floor
- The cuff should be on your bare upper arm, at heart level
- Do NOT smoke, exercise, or have caffeine 30 minutes before
- Measure at least 2-3 times and take the average
- Measure on the same arm each time
Types of BP monitoring:
- Office BP - measured by your doctor
- Home BP monitoring (HBPM) - you measure at home with your own device (the 2025 guidelines now emphasize this strongly)
- Ambulatory BP monitoring (ABPM) - a device you wear for 24 hours to get readings throughout the day and night - this is the most accurate method
The 2025 AHA/ACC guidelines now say that home and ambulatory BP monitoring should be central to diagnosis and management, not just supplements to office readings.
8. What Happens to Your Body With Hypertension?
High pressure in your arteries causes damage over time - like water pressure constantly beating against a pipe wall.
The main organs affected:
Heart
- The heart has to work harder to pump against high pressure
- The heart muscle gets thicker (left ventricular hypertrophy)
- This leads to heart failure (the heart gets too weak or too stiff to pump properly)
- Coronary artery disease and heart attack (myocardial infarction)
Brain
- Damaged arteries can burst: hemorrhagic stroke (bleeding in the brain)
- Blood clots form more easily in damaged arteries: ischemic stroke (blockage)
- Over time: dementia and cognitive decline
Kidneys
- High pressure damages the tiny filtering units in the kidney (glomeruli)
- Leads to chronic kidney disease (CKD)
- Eventually kidney failure requiring dialysis
Eyes
- Damaged blood vessels in the retina: hypertensive retinopathy
- Can cause blurred vision or even blindness
Blood Vessels
- Arteries throughout the body become stiff and narrow (atherosclerosis)
- Peripheral artery disease (poor circulation in legs)
- Aortic dissection (a life-threatening tear in the main artery) - Morgan & Mikhail's Clinical Anesthesiology
9. Hypertensive Emergencies
Hypertensive Crisis = BP above 180/120 mm Hg
There are two levels:
| BP | Organ Damage | Treatment | |
|---|---|---|---|
| Severe Hypertension (Urgency) | >180/120 | None | Oral drugs, lower BP over hours |
| Hypertensive Emergency | >180/120 | Yes (heart, brain, kidney affected) | IV drugs, lower BP within minutes to hours, hospitalize immediately |
Signs of organ damage in emergency:
- Chest pain (heart attack or aortic dissection)
- Shortness of breath (heart failure)
- Confusion or stroke symptoms
- Vision loss
- Kidney failure (less urine output)
10. Hypertension in Special Groups
In Pregnancy
- Gestational hypertension - high BP after 20 weeks, no protein in urine
- Preeclampsia - high BP after 20 weeks + protein in urine, or signs of organ damage
- Dangerous to both mother and baby
- Can cause seizures (eclampsia) - a life-threatening emergency
- Treatment with magnesium sulfate to prevent seizures; medications like labetalol or nifedipine to lower BP
- Delivery of the baby is the definitive cure
In Elderly
- "Isolated systolic hypertension" is common (top number is high, bottom number is normal)
- Goal BP is still <130/80 but must be careful not to lower BP too much (risk of falls and dizziness)
In Diabetes
- Hypertension + diabetes greatly multiplies the risk of kidney and heart disease
- ACE inhibitors or ARBs are preferred because they protect the kidneys
In Chronic Kidney Disease (CKD)
- Both hypertension causes CKD and CKD causes hypertension - a vicious cycle
- ACE inhibitors or ARBs are first-line to slow kidney damage
In Children
- Often secondary to kidney disease or coarctation of the aorta
- Lifestyle changes are the first step
11. Diagnosis - How Doctors Confirm Hypertension
- Measure BP on at least 2 separate visits
- Rule out secondary causes if:
- Young patient
- Resistant to multiple medications
- Sudden onset
- Low potassium (hypokalemia) - suggests aldosteronism
- Blood tests: kidney function, electrolytes, blood sugar, cholesterol, thyroid
- Urine test: for protein (sign of kidney damage)
- ECG: to check if heart is already enlarged
- Echocardiogram: to see heart size and function
- Eye exam (fundoscopy): to see if retinal vessels are damaged
White-coat hypertension - BP is only high in the doctor's office but normal at home. This is why home monitoring matters.
Masked hypertension - BP appears normal at the office but is actually high at home. This is dangerous because it goes untreated.
12. Treatment: Lifestyle Changes First
For most people with Stage 1 hypertension (130-139/80-89), lifestyle changes are tried first before medication:
The DASH Diet
DASH = Dietary Approaches to Stop Hypertension
- Eat more: fruits, vegetables, whole grains, low-fat dairy, nuts, seeds
- Eat less: salt (sodium), red meat, sugar, processed food, saturated fats
- Can lower BP by 8-14 mm Hg
Reduce Salt Intake
- Limit sodium to less than 2.3 grams per day (about 1 teaspoon of salt)
- The 2025 guidelines now also recommend salt substitutes (potassium chloride instead of sodium chloride) as an evidence-based strategy
Exercise
- At least 30 minutes of moderate-intensity aerobic exercise most days (walking, cycling, swimming)
- Can lower BP by 4-9 mm Hg
Weight Loss
- Losing even 5-10 kg (10-20 lbs) can significantly lower BP
- Every 1 kg of weight lost = approximately 1 mm Hg drop in systolic BP
Quit Smoking
- Smoking damages blood vessel walls and raises BP acutely
- Stopping protects the heart and vessels
Limit Alcohol
- Men: no more than 2 drinks per day
- Women: no more than 1 drink per day
Stress Reduction
- Relaxation techniques, adequate sleep, mindfulness
13. Treatment: Medications
When lifestyle changes are not enough, or BP is very high from the start, medications are needed.
The goal for most patients: BP < 130/80 mm Hg (2025 AHA/ACC guidelines)
The 4 Main First-Line Drug Classes
1. Thiazide Diuretics (Water Pills)
- Examples: Hydrochlorothiazide, Chlorthalidone
- How they work: Make your kidneys remove more salt and water, so blood volume decreases. After a few weeks, they also relax blood vessel walls.
- Good for: Most patients, especially elderly and African Americans
- Side effects: Low potassium (hypokalemia), high uric acid (can trigger gout), slightly raised blood sugar
2. ACE Inhibitors
- Examples: Lisinopril, Enalapril, Ramipril, Captopril
- How they work: Block a key enzyme (ACE) that converts angiotensin I to angiotensin II. Angiotensin II normally raises BP by narrowing blood vessels and increasing water retention. By blocking it, vessels relax and BP drops.
- Good for: People with diabetes, heart failure, chronic kidney disease
- Side effects: Dry persistent cough (in up to 10% of patients), high potassium, angioedema (rare but dangerous swelling of lips/throat), cannot be used in pregnancy
3. Angiotensin Receptor Blockers (ARBs)
- Examples: Losartan, Irbesartan, Valsartan, Olmesartan
- How they work: Similar to ACE inhibitors but block the receptor where angiotensin II acts (AT1 receptor). Lower BP by relaxing blood vessels and reducing water retention.
- Good for: Same as ACE inhibitors; preferred when ACE inhibitors cause a cough
- Side effects: Similar to ACE inhibitors but without the cough; still cannot be used in pregnancy
4. Calcium Channel Blockers (CCBs)
- Examples: Amlodipine, Nifedipine (dihydropyridines); Verapamil, Diltiazem (non-dihydropyridines)
- How they work: Calcium makes blood vessel muscle cells contract. By blocking calcium channels, the vessels relax and widen, lowering pressure.
- Good for: Elderly, African Americans, patients with angina (chest pain from heart)
- Side effects: Ankle swelling, flushing, headache; non-dihydropyridines (verapamil, diltiazem) can slow the heart
Other Drug Classes
| Drug Class | Examples | Used When |
|---|---|---|
| Beta-blockers | Metoprolol, Atenolol, Carvedilol | Heart failure, angina, after a heart attack, fast heart rate |
| Aldosterone antagonists | Spironolactone, Eplerenone | Resistant hypertension, heart failure |
| Alpha-blockers | Doxazosin | Enlarged prostate + hypertension |
| Central alpha-2 agonists | Clonidine, Methyldopa | Pregnancy (methyldopa), refractory cases |
| Vasodilators | Hydralazine, Minoxidil | Severe resistant hypertension |
| Renin inhibitor | Aliskiren | Alternative; NOT combined with ACE/ARB |
| Loop diuretics | Furosemide | Patients with kidney failure |
Drug Choice Based on Other Conditions
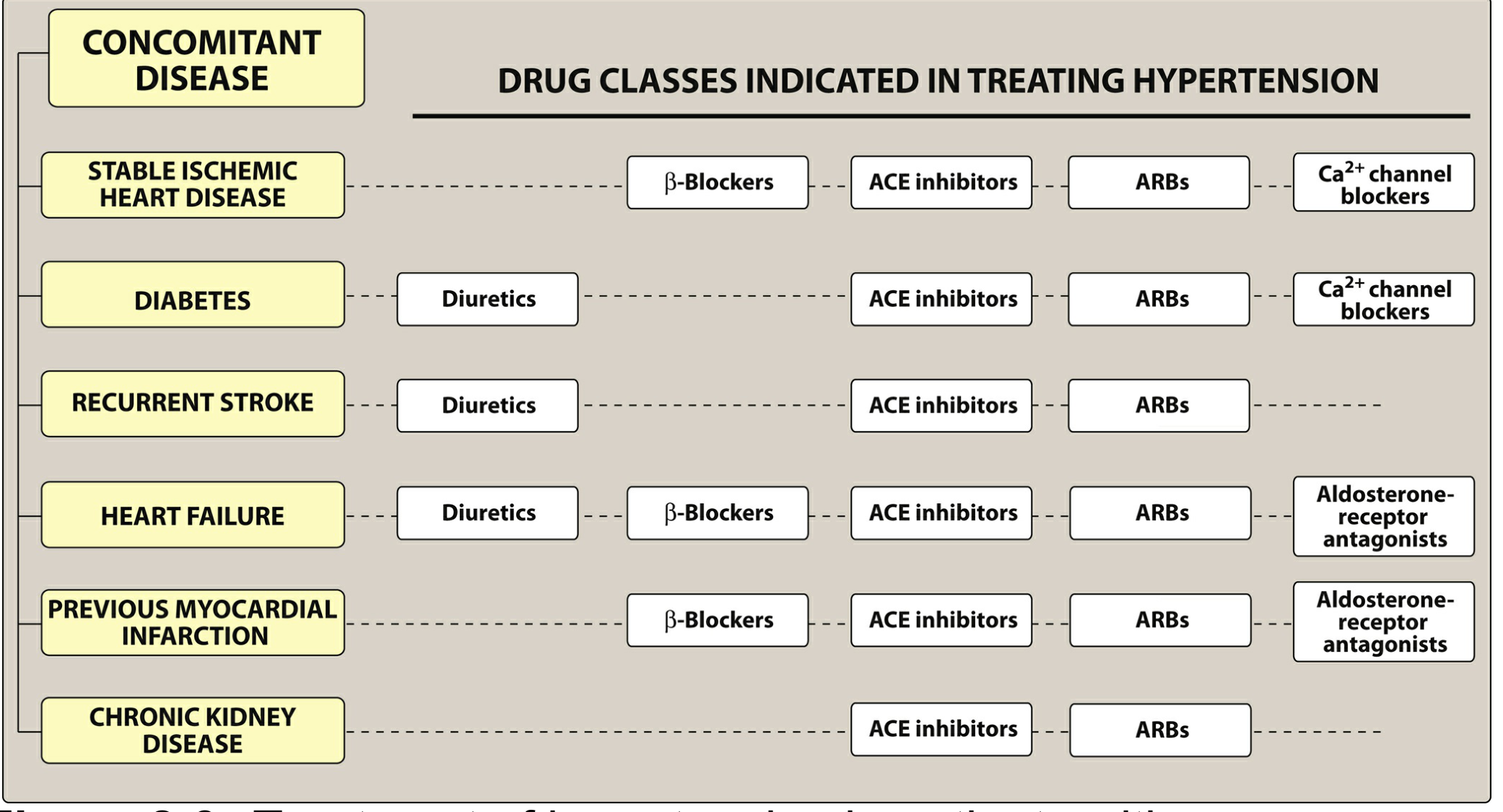
As shown in the chart above, the right drug depends on any other conditions the patient has. - Lippincott Illustrated Reviews: Pharmacology
When to Use More Than One Drug
- If BP is more than 20/10 mm Hg above target, start with TWO drugs at once
- Most people with hypertension need 2 or more drugs to reach their BP goal
- Fixed-dose combination pills (two drugs in one tablet) make this easier and improve compliance
14. Resistant Hypertension
Defined as: BP remaining above 130/80 mm Hg despite taking 3 or more antihypertensive medications (including a diuretic), or needing 4 or more medications to control it. - Goldman-Cecil Medicine
Why it happens:
- Not taking medications properly (poor adherence)
- Too much salt in diet
- Secondary cause not treated (e.g., undiagnosed sleep apnea or aldosteronism)
- Interactions with other medications (NSAIDs, birth control pills, steroids)
Treatment options for resistant hypertension:
- Add spironolactone (very effective)
- Renal denervation - a new procedure (catheter-based) that cuts the nerve supply to the kidneys. The 2025 AHA/ACC guidelines introduced this as a Class IIb option (can be used with shared decision-making).
15. Monitoring and Follow-Up
Once on treatment:
- Check BP regularly (home monitoring every day or at least weekly)
- Blood tests every 3-6 months to check kidneys, potassium, and blood sugar
- Annual eye exam
- ECG or echo if needed
- Keep taking your medications even when you feel well - hypertension has no symptoms but still causes damage silently
16. Can Hypertension Be Prevented?
Yes, to a large extent. The same lifestyle measures that treat it also prevent it:
- Healthy weight from childhood
- Low-salt, high-potassium diet
- Regular exercise
- No smoking
- Limited alcohol
- Stress management
- Regular BP checks from age 18 onward
17. Quick Summary Table
| Topic | Key Point |
|---|---|
| Definition | BP consistently ≥130/80 mm Hg |
| Types | Primary (90-95%) and Secondary (5-10%) |
| Symptoms | Usually NONE - "silent killer" |
| Main risk factors | Obesity, salt, alcohol, sedentary lifestyle, genetics |
| Complications | Stroke, heart attack, heart failure, kidney failure, blindness |
| Diagnosis | BP readings + blood/urine tests + ECG |
| Lifestyle treatment | DASH diet, exercise, weight loss, salt reduction |
| First-line drugs | Thiazide diuretics, ACE inhibitors, ARBs, CCBs |
| BP goal | <130/80 mm Hg for most adults (2025 guidelines) |
| Hypertensive emergency | BP >180/120 + organ damage = treat immediately with IV drugs |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 288 on Hypertension
- Lippincott Illustrated Reviews: Pharmacology - Antihypertensive Drugs Chapter
- Fuster and Hurst's The Heart, 15th Ed. - Pathophysiology of Primary Hypertension
- Goldman-Cecil Medicine - Drug-Resistant Hypertension
- Comprehensive Clinical Nephrology, 7th Ed. - Classification by Cause
- Park's Textbook of Preventive and Social Medicine - Hypertension Epidemiology
- 2025 AHA/ACC Hypertension Guideline - Updated BP classification and treatment thresholds
This is a shared conversation. Sign in to Orris to start your own chat.