
IMG_7529.jpeg
This patient had neck pain
Reading File
analyse_media
Finding Sources
Searching PubMed
"cervical lymphadenopathy" AND evaluation
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information to provide a thorough clinical interpretation. Here is the full analysis:
Neck Ultrasound Report - Clinical Interpretation
Patient: Mr. Bhuwan Goswami, 23-year-old male | Date: 03-Mar-2026
Facility: Fortis Hospital, Greater Noida | Reported by: Dr. Mayank Garg, MD (SR Radiology)
What the Report Shows
Impression: Cervical Lymphadenopathy - multiple enlarged lymph nodes in the neck.
Key findings:
- Thyroid gland: Normal in size, shape, and echotexture (this is reassuring - no thyroid pathology)
- Submandibular glands: Normal
- Jugular veins and carotid arteries: Normal
- Multiple lymph nodes detected at bilateral levels II, III, right levels IB, IVA & V, and left IA
- Largest node: ~7.2 mm short-axis diameter
How to Interpret the Nodes (7.2 mm Short Axis)
The 7.2 mm short-axis measurement is below the standard 10 mm cutoff used in most guidelines. Normal lymph nodes typically have a long-axis diameter roughly twice the short-axis diameter, preserving an oval/reniform shape. Nodes become suspicious when:
- Short-axis diameter exceeds 10 mm
- Shape becomes rounded (shape index >0.5)
- Loss of the echogenic fatty hilum
- Peripheral (rather than hilar) blood flow on Doppler
At 7.2 mm short axis, these nodes are borderline - not overtly pathological by size alone, but the bilateral, multilevel distribution across levels IA, IB, II, III, IVA, and V is clinically significant. - Sabiston Textbook of Surgery, 8th Ed.
Neck Level Map
The nodes span a wide distribution. Here is what those levels correspond to:
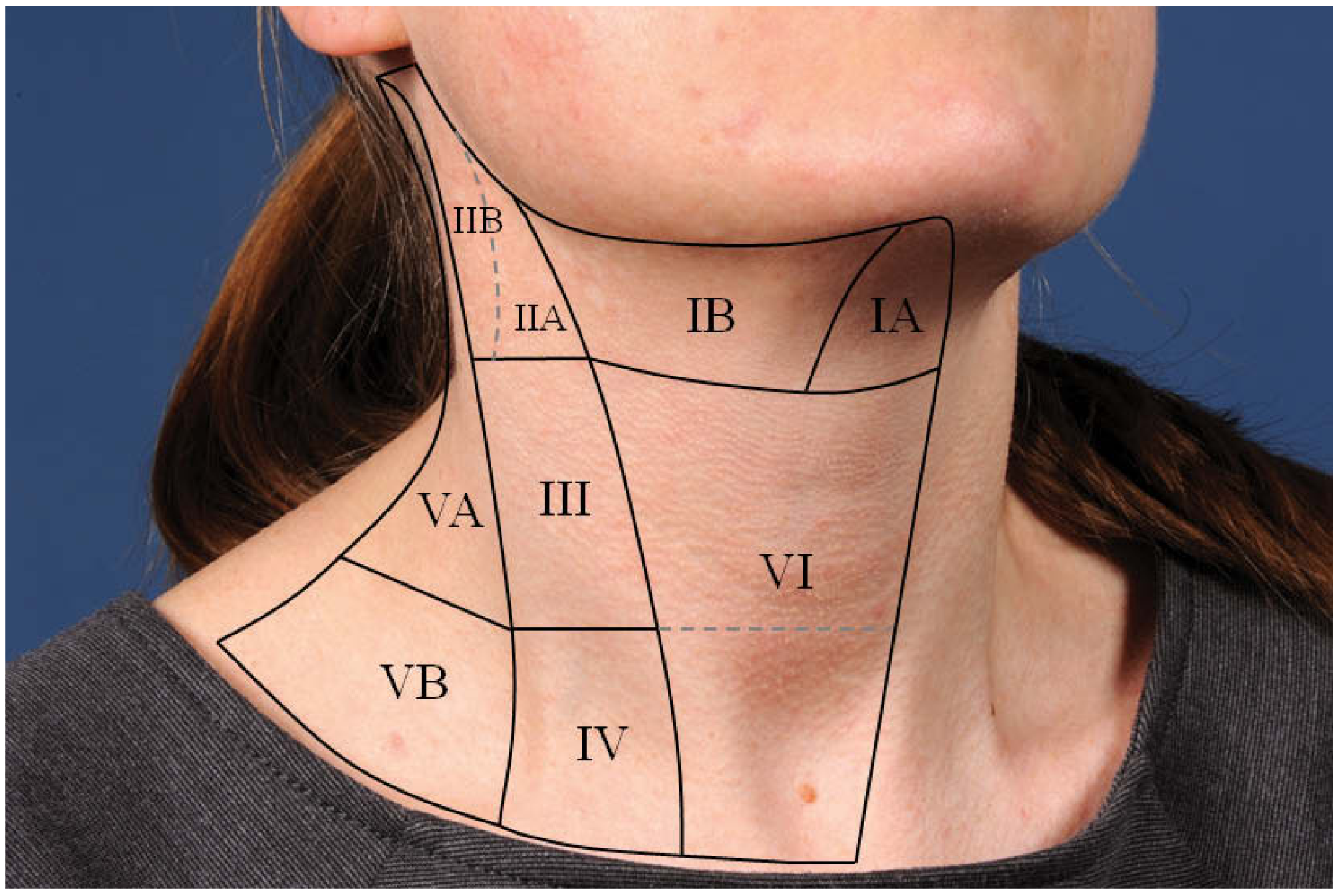
| Level | Region |
|---|---|
| IA | Submental (below chin, between digastric muscles) |
| IB | Submandibular (around submandibular gland) |
| II | Upper jugular chain (upper neck, along internal jugular vein) |
| III | Mid-jugular chain |
| IVA | Lower jugular chain |
| V | Posterior triangle (behind sternocleidomastoid) |
The bilateral distribution across multiple levels strongly suggests a reactive/systemic process rather than a focal infective or malignant process (which tends to be unilateral and localized). - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Differential Diagnosis for a 23-Year-Old Male with Neck Pain + Bilateral Cervical Lymphadenopathy
Most likely (reactive/infectious) - especially in a young adult:
- Infectious mononucleosis (EBV) - Classic cause of bilateral cervical lymphadenopathy in young adults; associated with pharyngitis, fever, fatigue. Should be at the top of the list.
- Viral upper respiratory infection - Rhinovirus, adenovirus, parainfluenza, CMV; very common and self-limiting.
- Bacterial pharyngitis/tonsillitis - Group A Streptococcus or Staphylococcus aureus (account for 40-80% of bacterial lymphadenitis). - Fischer's Mastery of Surgery
Less common but important to consider:
4. Tuberculosis (TB adenitis) - Especially relevant in India; commonly affects deep upper cervical nodes in young adults; neck pain can be a presenting feature. The bacilli typically enter via the tonsil. - Bailey & Love's Surgery, 28th Ed.
5. Toxoplasmosis - Most common parasitic cause; can present with painless or painful bilateral cervical lymphadenopathy.
6. HIV - Persistent generalized lymphadenopathy is an early feature; nodes are usually symmetrical and bilateral. Should be considered given the age group.
Less likely given young age and node size, but to rule out:
7. Lymphoma (Hodgkin/Non-Hodgkin) - Presents with B symptoms (night sweats, weight loss, fever); nodes >2 cm, firm, non-tender. These nodes at 7.2 mm are small, making lymphoma less likely - but it should not be dismissed without clinical correlation.
Recommended Next Steps (Clinical Correlation)
The radiologist appropriately recommends clinical correlation. Suggested workup:
| Investigation | Reason |
|---|---|
| CBC with differential | Reactive lymphocytosis in viral infections; atypical lymphocytes in EBV |
| Monospot test / EBV IgM | To rule out infectious mononucleosis |
| Throat swab / ASLO titre | If streptococcal pharyngitis is suspected |
| Mantoux test / IGRA | To rule out TB, especially in India |
| Chest X-ray | Screen for pulmonary TB or mediastinal lymphadenopathy |
| HIV serology | Important at this age group in the differential |
| ESR, CRP | Markers of inflammation |
| LDH, uric acid | If lymphoma is in the differential |
Reassuring signs in this report:
- Thyroid is normal (no thyroid malignancy)
- Nodes are small (<10 mm short axis) and bilateral (favors reactive)
- No report of necrosis, calcification, or loss of hilum (which would raise concern for TB or malignancy)
Red flags to watch for clinically:
- Nodes rapidly enlarging or >2 cm
- Firm, fixed, or rubbery consistency
- Constitutional B symptoms (night sweats, unexplained weight loss, fever >38°C)
- Asymmetric involvement developing over time
- Failure to regress after 4-6 weeks
Bottom line: For a 23-year-old with neck pain and bilateral multilevel cervical lymphadenopathy up to 7.2 mm, a reactive/infectious cause (most likely viral - consider EBV first) is by far the most probable explanation. Initiate the basic workup above, treat symptomatically if a benign viral cause is confirmed, and reassess in 4-6 weeks. If nodes persist, enlarge, or B symptoms appear, escalate to biopsy/further imaging. - Cummings Otolaryngology Head & Neck Surgery

IMG_7543.jpeg
Recent one
analyse_media
Finding Sources
Finding Sources
Searching PubMed
"cervical lymphadenopathy" AND "biopsy" AND young adult
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have enough to give a thorough comparative analysis. Here is the critical breakdown:
Follow-Up Neck Ultrasound - Comparison & Clinical Alert
Patient: Mr. Bhuwan Goswami, 23M | Date: 06-Jul-2026
Reported by: Dr. S Shubham, MD (Consultant Radiology)
⚠️ Critical Change: Significant Nodal Progression in 4 Months
| Parameter | March 2026 | July 2026 | Change |
|---|---|---|---|
| Largest node (short axis) | 7.2 mm | 8.8 mm | +1.6 mm |
| Largest node (long axis) | Not reported | 17.8 mm | New data |
| Level affected | Bilateral II, III, IB, IVA, V, IA | Level II (most prominent) | Persisting |
| Thyroid | Normal | Normal | Unchanged |
| Submandibular glands | Normal | Normal | Unchanged |
| Vessels | Normal | Normal | Unchanged |
Why This Matters
The 10 mm Short-Axis Rule
The standard threshold for pathologically enlarged cervical lymph nodes on ultrasound is 10 mm short-axis diameter. This patient's largest node is now at 8.8 mm short axis - still just under the traditional cutoff. However, there is a more alarming issue: the node is now 17.8 mm in long axis, which gives a shape index of 8.8/17.8 = 0.49 - borderline rounded, approaching the suspicious threshold of 0.5. - Sabiston Textbook of Surgery
Progressive Growth Over 4 Months = Red Flag
A lymph node that does not regress and continues to grow over 4 months in a young adult is a significant warning sign. In context:
- Reactive/viral nodes typically resolve within 4-6 weeks
- Persistence beyond 4-6 weeks, especially with growth, warrants aggressive workup
- Tuberculous lymphadenitis shows "rapid initial enlargement, followed by continued slow growth over time" - exactly this pattern. - Fischer's Mastery of Surgery
- Lymphoma can present with slowly but progressively enlarging bilateral cervical nodes in young adults
Revised Differential Diagnosis (Priority-Ordered for July 2026)
Given 4 months of persistence + nodal growth:
NOW HIGH PRIORITY:
- Tuberculosis (TB adenitis) - India-endemic, young adults most affected, deep upper cervical nodes (level II-III) commonly involved, slow progressive growth is characteristic. TB bacilli typically enter via the tonsil. The violet skin discoloration and collar-stud abscess may develop if untreated. - Bailey & Love's Surgery
- Lymphoma (Hodgkin's disease) - Young adults (bimodal peak at 15-35 years), level II neck is a classic site. Must be ruled out urgently. Associated B symptoms: fever >38°C, drenching night sweats, >10% weight loss.
- Infectious mononucleosis (EBV) - chronic/persistent - EBV can cause large nodes; however, persistent for 4 months would be unusual without diagnosis.
- Kikuchi-Fujimoto disease - Necrotizing lymphadenitis in young adults, self-limiting but can persist for months, associated with fever.
- Reactive lymphadenopathy - Now less likely given the 4-month persistence and growth.
LOWER PRIORITY NOW:
- Simple viral upper respiratory infection (would have resolved)
- Bacterial lymphadenitis (acute, would have responded to antibiotics)
Urgent Recommended Workup
This patient now requires an urgent, systematic investigation. Do not delay.
| Investigation | Priority | Rationale |
|---|---|---|
| CBC with differential + peripheral smear | Urgent | Atypical lymphocytes (EBV), lymphocytosis, blast cells (leukemia) |
| ESR, CRP, LDH, uric acid | Urgent | LDH elevated in lymphoma; ESR elevated in TB/lymphoma |
| Mantoux (tuberculin skin test) / IGRA (QuantiFERON) | Urgent | To rule out TB - especially in India |
| Chest X-ray (PA view) | Urgent | Mediastinal widening (lymphoma), pulmonary TB |
| EBV (Monospot/VCA IgM), CMV serology | Urgent | Rule out viral causes |
| HIV serology | Urgent | Risk factor for TB, lymphoma |
| FNAC (Fine Needle Aspiration Cytology) of the 17.8 mm node | Most important next step | Definitive tissue diagnosis; should be performed now given 4 months of persistence + growth |
Key point on FNAC vs excision biopsy: FNAC is the preferred first-line tissue sampling for cervical lymphadenopathy. If FNAC is non-diagnostic or inconclusive, excision biopsy should follow immediately. For suspected lymphoma, excision biopsy is often preferred over FNAC as it preserves nodal architecture needed for classification. - Fischer's Mastery of Surgery
Important: If TB is suspected clinically, avoid incision and drainage (I&D) - this causes chronic fistulous tract formation. Excisional biopsy is the safer surgical approach. - Fischer's Mastery of Surgery
Bottom Line
This patient's lymphadenopathy has not resolved in 4 months and the largest node has grown to 17.8 x 8.8 mm. This is beyond the window for watchful waiting. The two diagnoses that must be excluded urgently are tuberculosis and lymphoma. A FNAC of the largest node should be arranged immediately, alongside the blood workup listed above. The referring doctor (Dr. Anil Kumar Rai) should be clearly informed of this clinical urgency.
This is a shared conversation. Sign in to Orris to start your own chat.