Ankylosing spondylitis
Reading File
Finding Sources
Searching PubMed
"ankylosing spondylitis"[MeSH Terms] AND treatment
Searching the Web
ankylosing spondylitis 2025 2026 guidelines treatment update
Reading File
Reading File
Searching PubMed
"ankylosing spondylitis"[MeSH Terms] AND "biologics"[tiab]
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have rich content from multiple authoritative textbooks. Let me compile the comprehensive answer.
Ankylosing Spondylitis (AS)
Overview
Ankylosing spondylitis is a chronic, progressive inflammatory spondyloarthropathy that primarily targets the axial skeleton - the sacroiliac joints, spine, and large peripheral joints. It is the prototypic form of axial spondyloarthritis (AxSpA). The term itself derives from Greek: ankylos (bent/fused) and spondylos (vertebra).
Epidemiology
-
Prevalence: ~0.1-0.5% of the general population; varies by ethnic group and HLA-B27 frequency
-
Age of onset: Most commonly 15-25 years; rarely begins after age 40
-
Sex: Affects men 2-3x more than women, though women are increasingly recognized (often milder or delayed diagnosis)
-
Genetics: Heritability exceeds 95%. Sibling recurrence risk is 9.2% vs. 0.1-0.4% in the general population
-
Firestein & Kelley's Textbook of Rheumatology, p. 3122
Pathogenesis
HLA-B27 and Genetics
- HLA-B27 is the strongest genetic susceptibility factor: >90% of White AS patients carry it (vs. ~8% of the general population), giving a relative risk of 50-100
- Only ~2% of HLA-B27-positive individuals develop AS, so additional genetic and environmental factors are required
- Over 80 risk loci outside the HLA region have been identified, including:
- ERAP1/ERAP2 (aminopeptidase genes) - involved in peptide trimming for HLA presentation; ERAP1 association is only found in HLA-B27-positive individuals (genetic epistasis)
- IL-23R, IL-12B, IL-27 - genes in the IL-23/IL-17 pathway (key therapeutic target)
Immune Mechanisms
-
The IL-23/IL-17 axis plays a central role: IL-23 drives Th17 differentiation, which produces IL-17A/F; this promotes entheseal inflammation
-
Notably, anti-IL-17 drugs are effective in AS but anti-IL-23 drugs are not - suggesting IL-23-independent sources of IL-17 at entheses (likely innate immune cells)
-
TNF-alpha also mediates spinal and sacroiliac inflammation
-
Pathological process: enthesitis (inflammation at ligament/tendon insertions into bone) → new bone formation → syndesmophytes → fusion
-
Firestein & Kelley's Textbook of Rheumatology, p. 3154-3166
Clinical Features
Axial (Spine and Sacroiliac)
- Inflammatory back pain is the hallmark - insidious onset, age <40, duration >3 months, worse with rest, improved with exercise, associated with morning stiffness >1 hour
- Sacroiliitis - bilateral and symmetrical; buttock pain may radiate down the thighs
- Reduced spinal mobility in all planes (Schober's test < 5 cm)
- Progressive thoracic kyphosis, loss of lumbar lordosis
- Chest wall restriction: fusion of costovertebral and sternoclavicular joints limits rib cage expansion to <2.5 cm (measured at 4th intercostal space)
Peripheral Joint Involvement
- Up to 30% of patients have peripheral arthritis (hips are the most important - the second most commonly affected joint after the SIJ)
- Hip involvement leads to diffuse joint space loss and characteristic entheseal new bone around the femoral head (can mimic femoroacetabular impingement)
Extra-articular Manifestations
| Feature | Frequency | Notes |
|---|---|---|
| Anterior uveitis | ~25-40% | Acute, unilateral, recurrent; HLA-B27-associated |
| Inflammatory bowel disease | ~5-10% | Crohn's > UC |
| Psoriasis | ~10% | |
| Pulmonary (fibrobullous upper lobe disease) | 1-4% | Bilateral upper lobe fibrosis and cyst formation; no effective therapy |
| Aortic regurgitation | rare | Ascending aortitis |
| Cardiac conduction defects | rare | |
| Cauda equina syndrome | rare | Late complication |
Late Complications
-
Osteoporosis - from chronic inflammation and abnormal biomechanical loading
-
Spinal fractures - the rigid, fused spine is paradoxically osteopenic and highly vulnerable; transverse fractures through fused segments are highly unstable and potentially catastrophic
-
Spondylodiscitis (Andersson lesion) - inflammatory destructive lesion at unfused disc levels in an otherwise fused spine; can mimic infection
-
Restrictive lung disease - from rib cage fixation; diaphragm compensates but eventually may cause respiratory failure
-
Goldman-Cecil Medicine, p. 3943-3945; Grainger & Allison's Diagnostic Radiology, p. 3659-3661
Diagnosis
Modified New York Criteria (for AS)
Clinical criteria:
- Low back pain and stiffness for >3 months, improved with exercise and not relieved by rest
- Limited lumbar spine motion in sagittal and frontal planes
- Limited chest expansion (relative to normal values for age and sex; <2.5 cm at 4th ICS)
Radiological criterion:
- Bilateral sacroiliitis grade ≥2, OR unilateral sacroiliitis grade 3-4
Definite AS = radiological criterion + ≥1 clinical criterion
ASAS Classification Criteria (axial SpA, broader)
Allows diagnosis before radiographic sacroiliitis (non-radiographic axial SpA) using MRI evidence of active inflammation or HLA-B27 + ≥2 other SpA features.
Laboratory
- HLA-B27: positive in >90% of White patients (lower in other ethnic groups, e.g., ~70% in African Americans)
- Elevated CRP/ESR: in active disease (~50-60% of patients; normal does not exclude active disease)
- RF and ANA: negative (hence "seronegative" spondyloarthropathy)
- Henry's Clinical Diagnosis and Management by Laboratory Methods: HLA-B27 testing is confirmatory but not sufficient alone
Imaging
Plain Radiography
- Sacroiliac joints: erosion, subchondral sclerosis, eventually ankylosis (bilateral, symmetrical)
- Spine:
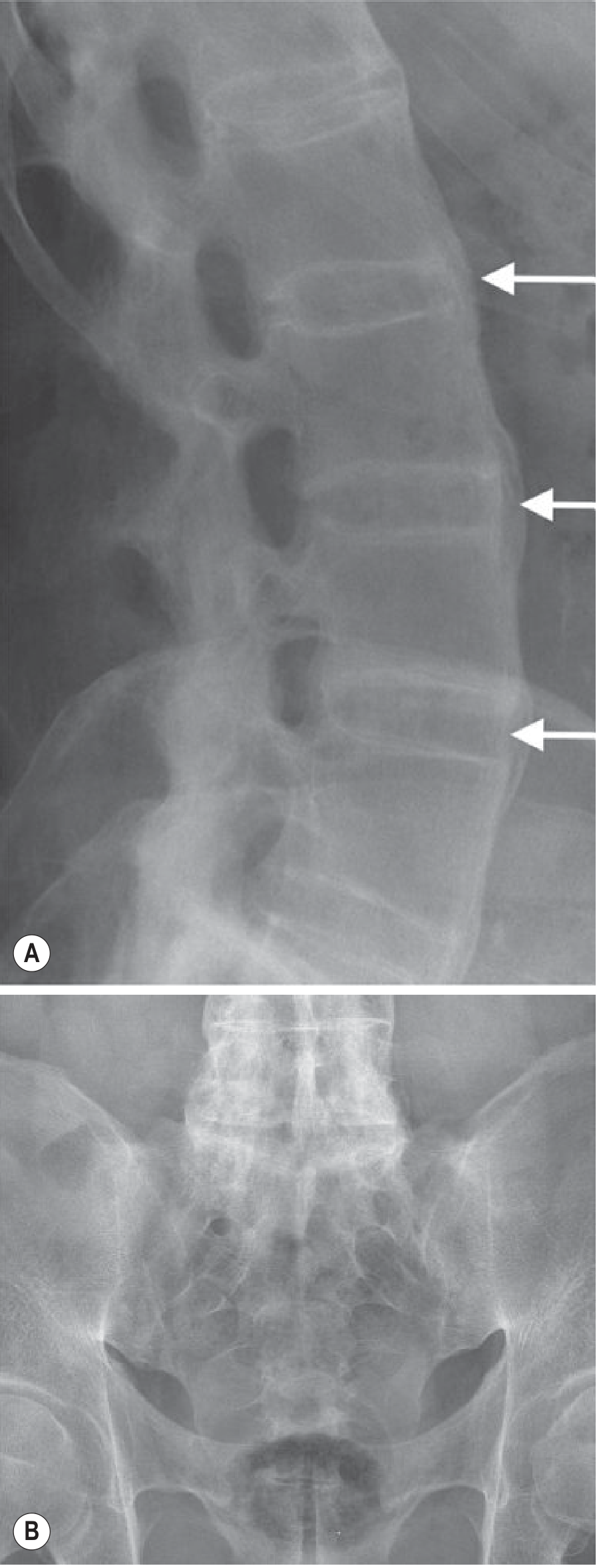
- Romanus lesions - sclerotic "shiny corners" at vertebral body corners (earliest X-ray finding; due to enthesitis at Sharpey fiber insertions)
- Squared vertebrae - due to erosion and anterior longitudinal ligament ossification
- Syndesmophytes - thin, vertical bone outgrowths (distinguishable from the coarser, horizontal osteophytes of OA or the "chunky" syndesmophytes of psoriatic/reactive arthritis)
- Bamboo spine - complete fusion of vertebral bodies and posterior elements (end-stage)
Fig. 44.17 - MRI of sacroiliac joints in AS: T1-weighted image shows erosion and joint space loss; T2 fat-suppressed shows extensive subchondral oedema (active disease):
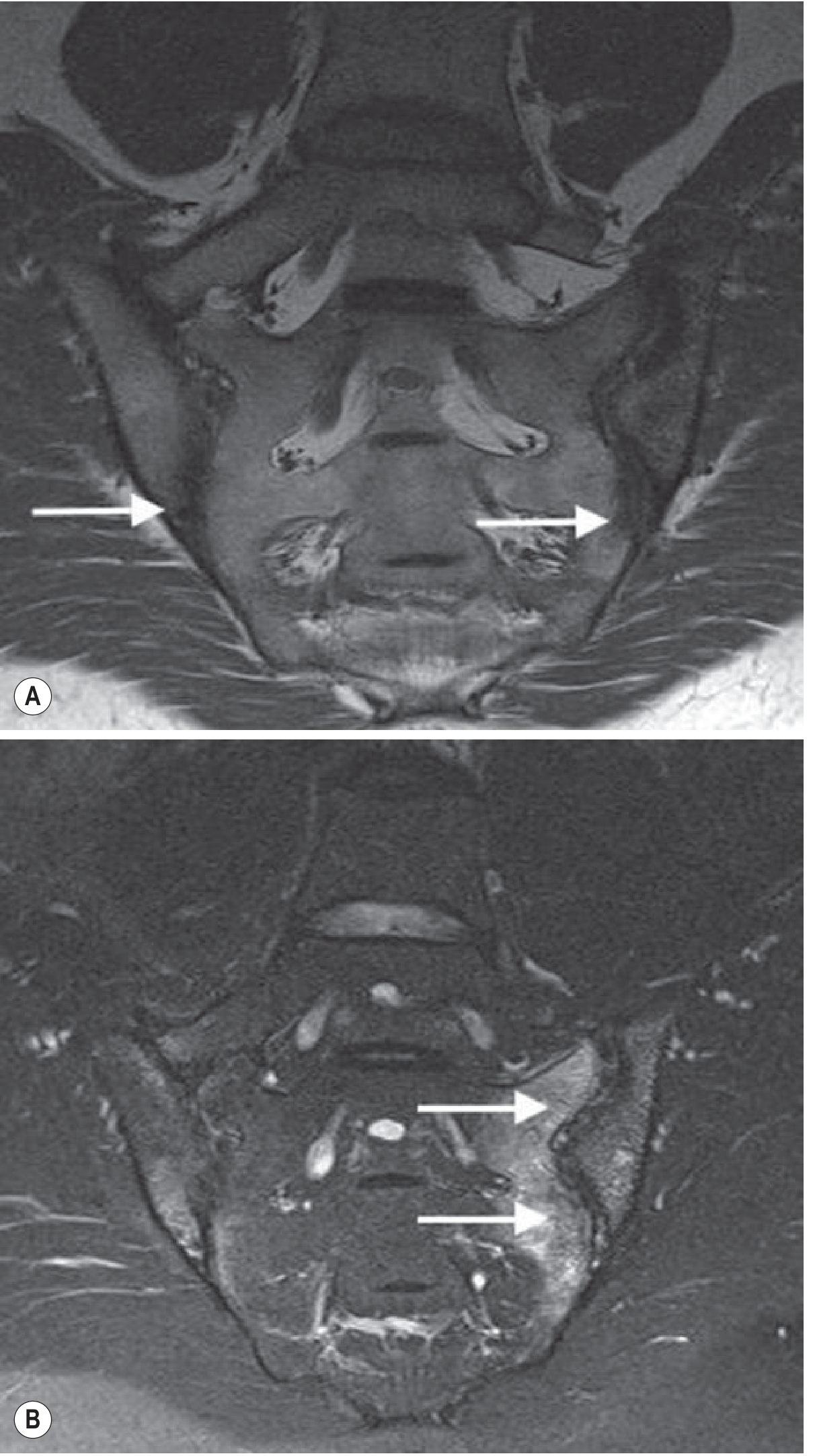
Fig. 44.18 - Plain radiograph showing Romanus lesions (sclerotic vertebral corners) and bridging syndesmophytes in the thoracic spine:

Fig. 44.20 - Advanced bamboo spine with vertical syndesmophytes (A) and complete bilateral sacroiliac joint fusion (B):
MRI (preferred for early disease)
- Most sensitive and specific for early sacroiliitis and spinal inflammation
- Detects subchondral bone marrow oedema before plain radiograph changes appear
- Key distinguishing feature: AS-related oedema is greater in craniocaudal dimension than transverse, and is not associated with disc dehydration or height loss (vs. degenerative disease)
- STIR sequences best for detecting active inflammation
CT
-
Best for detecting structural damage, erosions, and degree of ankylosis
-
Not preferred for early disease (radiation, poor sensitivity for marrow oedema)
-
Grainger & Allison's Diagnostic Radiology, p. 3621-3662
Treatment
Non-Pharmacological
- Exercise and physiotherapy are strongly recommended and improve cardiorespiratory fitness, spinal mobility, and pain - must be started concurrently with drug therapy
- Posture training, hydrotherapy, supervised group exercise
- Smoking cessation (smokers have worse outcomes and more rapid radiographic progression)
NSAIDs (First-Line)
- NSAIDs at maximum tolerated doses are the cornerstone of treatment for active disease
- Continuous treatment is preferred over on-demand use for persistent symptoms
- No particular NSAID is superior to another; patient-specific factors (GI risk, cardiovascular risk) guide selection
- Treatment failure is defined as inadequate response to at least two different NSAIDs
- ACR guidelines: strong evidence for NSAIDs; strong caution against systemic glucocorticoids for active AS
Biologic DMARDs (Second-Line)
TNF Inhibitors (TNFi) - first biologic choice:
Five TNFi are approved and show remarkable efficacy similarity:
- Adalimumab, etanercept, infliximab, certolizumab pegol, golimumab
- Improve symptoms, quality of life, CRP, anemia, sleep, and MRI inflammation scores
- Early and continuous treatment inhibits radiographic progression (syndesmophyte formation)
- Special considerations: For patients with comorbid inflammatory bowel disease or recurrent uveitis, prefer infliximab or adalimumab over etanercept (TNFi monoclonal antibodies > etanercept for these conditions)
- TNFi are also effective in non-radiographic axial SpA
IL-17 Inhibitors - alternative biologic:
- Secukinumab, ixekizumab (IL-17A inhibitors) - effective in AS
- Bimekizumab (IL-17A and IL-17F dual inhibitor) - also effective
- Preferred in patients who fail or cannot tolerate TNFi, or with predominant skin involvement
- Note: anti-IL-23 agents (guselkumab, risankizumab) do NOT work in AS despite working in psoriatic arthritis
JAK Inhibitors (Third-Line/Later):
- Tofacitinib (JAK inhibitor) - FDA-approved December 2021 for AS in patients with inadequate response to or intolerance of TNFi
- ASAS20 achieved in 56.4% vs. 12.5% placebo at 16 weeks; response seen by 2-4 weeks
- Safety: hepatic events (2.3%), herpes zoster (2.3%), serious infections (0.8%)
- Upadacitinib - also approved for AS
Certolizumab for Non-Radiographic AxSpA
- First anti-TNF agent FDA-approved for non-radiographic axial SpA specifically
Surgery
-
Total hip arthroplasty for severe hip involvement
-
Spinal osteotomy for severe fixed kyphotic deformity
-
Special anesthetic consideration: endotracheal intubation must be performed with great caution due to rigid cervical spine; hyperextension can cause fracture; cricoarytenoid joint involvement may limit mouth opening
-
Firestein & Kelley's Textbook of Rheumatology, p. 7809-7823; Goldman-Cecil Medicine, p. 3948
Disease Monitoring
- BASDAI (Bath Ankylosing Spondylitis Disease Activity Index) - validated patient-reported measure
- ASDAS (Ankylosing Spondylitis Disease Activity Score) - incorporates CRP; preferred by guidelines
- Serial MRI for assessing response to biologics
- Serial plain radiographs every 2 years to monitor structural progression
Prognosis
-
Clinical course is highly variable
-
Strongest predictor of new syndesmophyte formation is presence of syndesmophytes at baseline
-
Significant impact on work disability and quality of life
-
Osteoporosis occurs in proportion to disease duration and activity
-
With early biologic treatment, radiographic progression can be significantly retarded
-
Late complications (bamboo spine, fractures, cauda equina syndrome, upper lobe fibrosis) are largely preventable with effective therapy
-
Goldman-Cecil Medicine, p. 1004-1008
Sources: Firestein & Kelley's Textbook of Rheumatology (2-Volume Set); Goldman-Cecil Medicine International Edition; Grainger & Allison's Diagnostic Radiology; ACR/SAA/SPARTAN Guidelines (2019 update)
This is a shared conversation. Sign in to Orris to start your own chat.