
IMG-20260529-WA0024.jpg
Find its clinical findings and treatment required in this case
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here is a full clinical analysis of this MRI report:
MRI Right Knee - Clinical Analysis
Patient: Sunil Prajapat, 19-year-old male | Date: 26/05/2026
Scan: 1.5 Tesla MRI, no gadolinium, sequences T1W, T2W, PDW/FS PDW, STIR, GRE
MRI Findings Summary
| Structure | Finding |
|---|---|
| Posterior horn medial meniscus | Contusional (intrasubstance) signal - Grade 1-2 signal change |
| ACL | Moderate sprain (Grade 2 - partial tear) |
| Bones | Normal cortical outline, normal marrow; no osteophytes |
| Tibiofemoral joint space | Preserved |
| Lateral meniscus | Normal morphology and signal |
| PCL | Normal morphology, signal, alignment, fibre continuity |
| MCL | Normal |
| LCL | Normal |
| Patellar retinaculum | Intact, normal signal |
| Popliteus/posterolateral corner | Within normal limits |
| Patella (Wiberg Type 2) | Articular cartilage normal |
| Joint effusion | Mild/no significant effusion |
Clinical Findings to Expect
1. Medial Meniscus Posterior Horn Contusion (Grade 1-2 Intrasubstance Signal)
A "contusional signal" in the meniscus represents an intrasubstance injury - the signal change (increased on MRI) does not extend to the articular surface, meaning this is not a full tear. The meniscal architecture is preserved.
Expected clinical signs and symptoms:
- Medial joint line tenderness (posteromedial aspect)
- Pain worsened by full flexion or rotation
- McMurray's test may be mildly positive (pain without a definite click/clunk)
- Thessaly test may provoke pain at the medial joint line
- No locking (no displaced fragment)
- Possible mild swelling from synovial irritation
2. Moderate ACL Sprain (Grade 2 - Second-Degree Sprain)
A "moderate sprain" corresponds to a Grade 2 / second-degree sprain - partial disruption of ACL fibres with intact gross continuity. The ACL is not completely torn.
As per the sprain classification from Campbell's Operative Orthopaedics:
- Disruption of ligamentous fibres (partial, not complete)
- Joint reaction (pain, tenderness, swelling)
- Some loss of function / mild-to-moderate instability
Expected clinical signs and symptoms:
- Anterior knee pain and swelling
- Lachman test: Positive but with a firm endpoint (ligament partially intact)
- Anterior drawer test: Mildly positive
- Pivot shift test: May be mildly positive
- Difficulty with cutting, pivoting, or sudden deceleration
- Joint line tenderness anteriorly
- Mild haemarthrosis may be present
Treatment Plan
Immediate / Acute Phase (Week 1-2): PRICE Protocol
| Component | Detail |
|---|---|
| Protection | Functional knee brace (hinged) to protect the partially injured ACL; activity restriction |
| Rest | Avoid pivoting, running, jumping, contact sport |
| Ice | 15-20 min application, 3-4x daily to reduce swelling |
| Compression | Compression bandage or sleeve |
| Elevation | Limb elevation when resting |
Analgesics/Anti-inflammatories:
- NSAIDs (e.g., ibuprofen 400-600 mg TDS or diclofenac 50 mg BD) for 1-2 weeks
- Paracetamol for background pain relief
Conservative Rehabilitation Phase (Week 2-12)
This is the primary treatment for this patient, given:
- Grade 2 (moderate) ACL sprain (not a complete rupture)
- Meniscal contusion (intrasubstance, not a tear requiring surgery)
- 19-year-old - young patient who must be carefully monitored for instability
Phase 1 (Weeks 1-3) - Inflammation control:
- Crutches for offloading if pain is significant
- Isometric quadriceps and hamstring exercises
- Straight leg raises
- Range-of-motion exercises to regain full extension
Phase 2 (Weeks 3-8) - Strength recovery:
- Closed-chain exercises: mini squats, leg press, stationary cycling
- Proprioception and balance training (wobble board)
- Swimming and pool running
- Progressive weight-bearing
Phase 3 (Weeks 8-16) - Functional return:
- Jogging on flat surfaces
- Sport-specific agility drills
- Neuromuscular control training
- Plyometric exercises when quadriceps strength reaches 80% of contralateral limb
Surgical Considerations
Surgery is NOT indicated immediately for this presentation. However, surgical intervention should be reconsidered if:
- Persistent instability despite 3-6 months of rehabilitation
- Meniscal contusion progresses to a symptomatic tear (locking, catching, giving way)
- Return to high-demand sport fails due to recurrent giving way episodes
If surgery is needed in future:
- ACL reconstruction (autograft - patellar tendon or hamstring) - best performed when the knee has recovered full range of motion and muscle strength
- Arthroscopic meniscal debridement or repair if contusion evolves into a tear
Sprain Classification Reference
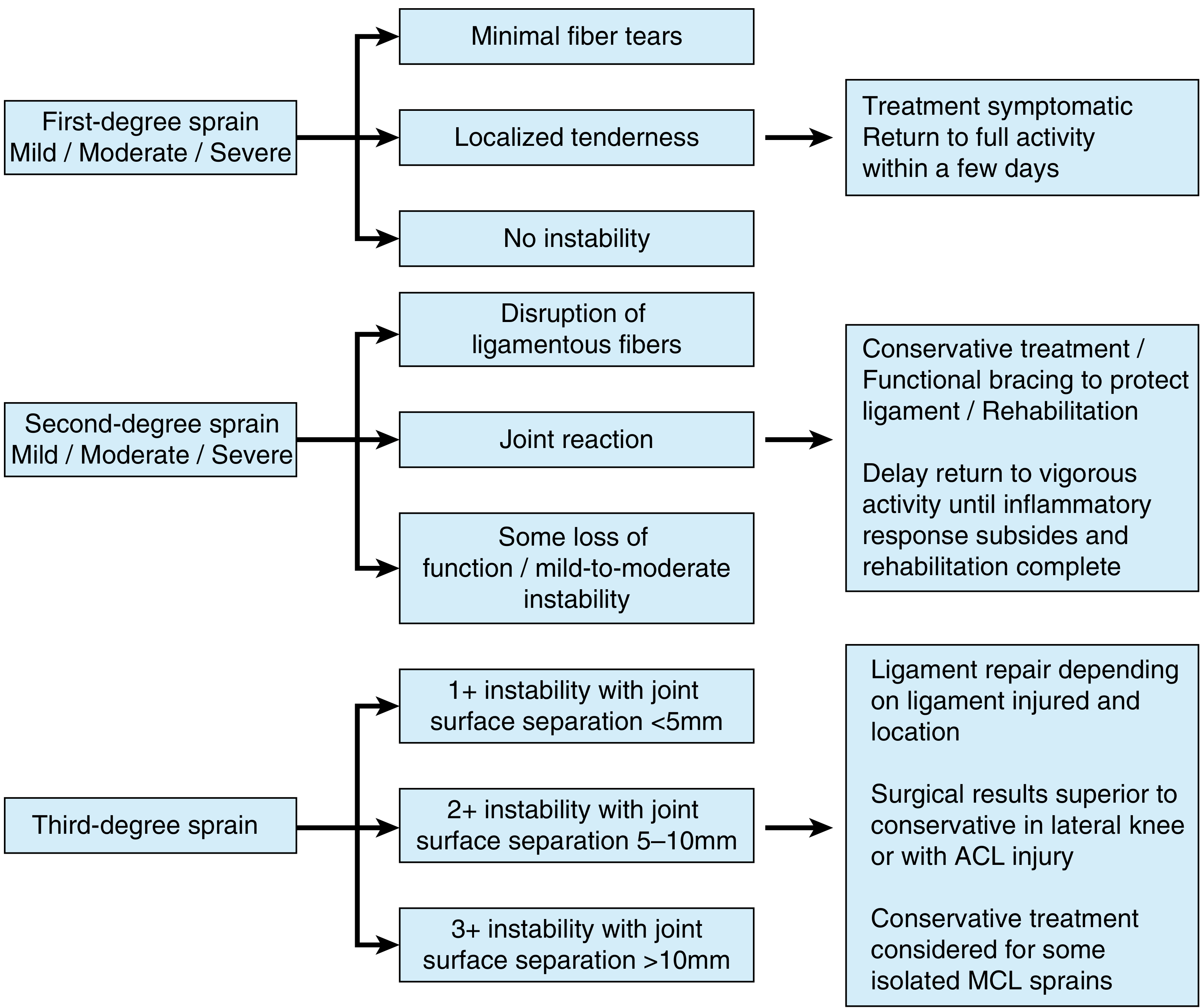
This patient falls into the second-degree (moderate) sprain category: conservative treatment with functional bracing, rehabilitation, and delayed return to vigorous activity until the inflammatory response has settled and rehabilitation is complete.
Follow-Up Recommendations
- Orthopaedic review in 2-4 weeks - assess Lachman/pivot shift clinically, monitor effusion
- Physiotherapy - structured programme as above
- Repeat MRI at 3 months if symptoms worsen or instability persists
- Return to sport only after full strength recovery and negative instability tests
- Avoid high-risk activities (pivoting sports, contact sports) until cleared
Note: This analysis is based on the radiological report. Clinical correlation with history, mechanism of injury, and physical examination findings is essential before finalizing the management plan, as stated in the report itself.
- Bailey and Love's Short Practice of Surgery 28th Edition, Meniscal tears section
- Campbell's Operative Orthopaedics 15th Ed 2026, Classification and Treatment of Sprains
This is a shared conversation. Sign in to Orris to start your own chat.