Explain in detailed about anticoagulant
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from multiple major pharmacology textbooks. Let me compile the full, detailed answer.
Anticoagulants - A Detailed Overview
Anticoagulants are drugs that prevent blood clot formation (thrombosis) by interfering with one or more steps of the coagulation cascade. They are distinct from thrombolytics (which dissolve existing clots) and antiplatelets (which prevent platelet aggregation).
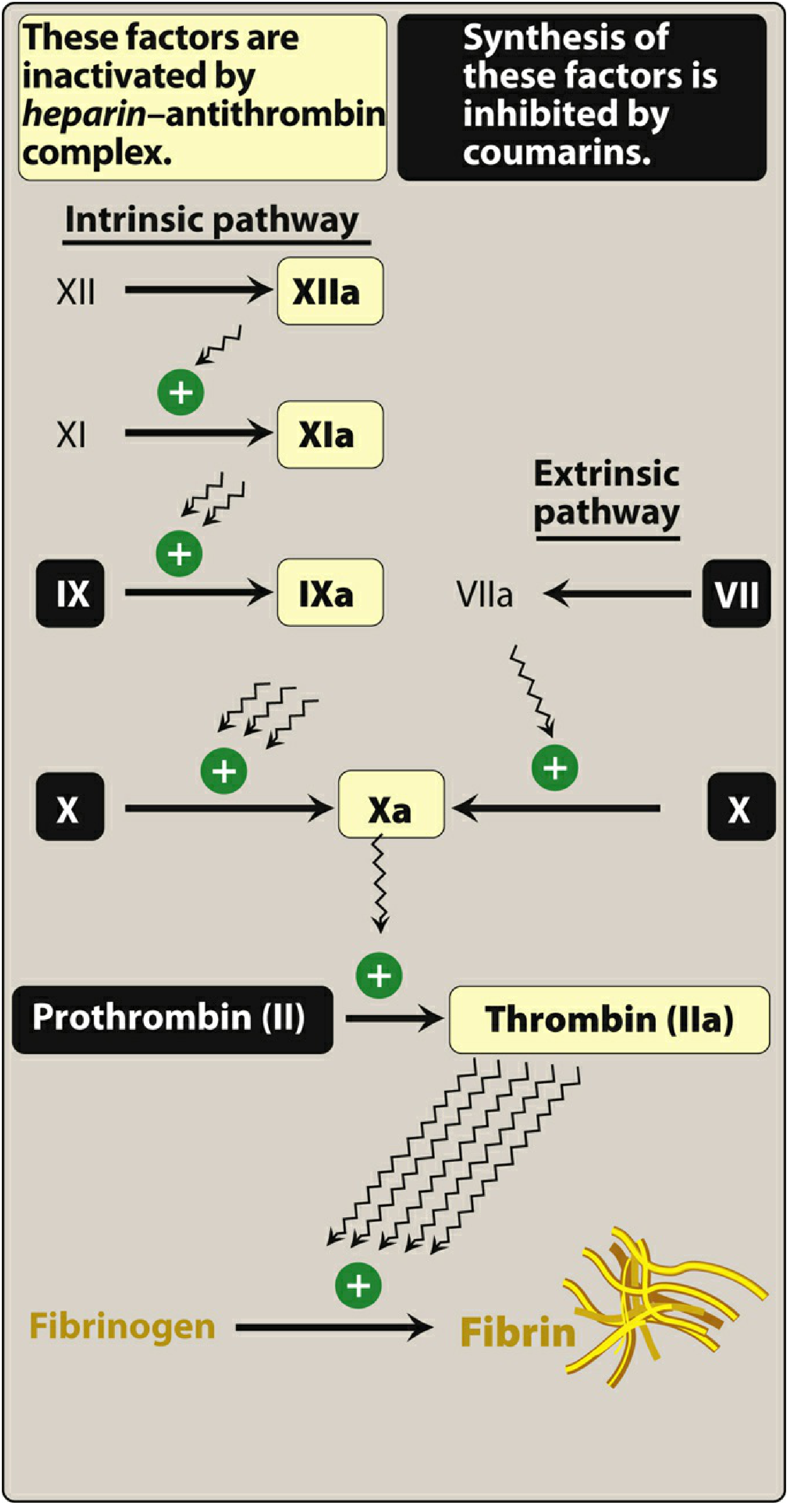
1. The Coagulation Cascade - Background
Understanding anticoagulants requires knowing what they target. Coagulation occurs via two converging pathways:
- Extrinsic pathway: Tissue factor (TF) + Factor VII → TF-VIIa complex → activates Factor X
- Intrinsic pathway: Contact activation (XII → XI → IX → X)
- Common pathway: Factor Xa + Va → Prothrombin (II) → Thrombin (IIa) → Fibrinogen → Fibrin clot
Natural Anticoagulant Mechanisms
The body has its own brake system on coagulation:
| Natural Inhibitor | Mechanism |
|---|---|
| Antithrombin (AT) | Serine protease inhibitor; inactivates IIa, IXa, Xa, XIa, XIIa |
| Protein C + Protein S | Proteolytically degrade cofactors Va and VIIIa |
| TFPI | Binds/inhibits Factor Xa, then the Xa-TFPI complex inhibits TF-VIIa |
Defects in these systems (e.g., Factor V Leiden - resistance to Protein C cleavage) lead to thrombophilia. - Katzung's Basic & Clinical Pharmacology, 16e
2. Classification of Anticoagulants
ANTICOAGULANTS
├── PARENTERAL
│ ├── Indirect thrombin inhibitors (via Antithrombin)
│ │ ├── Unfractionated Heparin (UFH)
│ │ ├── Low Molecular Weight Heparins (LMWH)
│ │ │ - Enoxaparin, Dalteparin, Tinzaparin
│ │ └── Fondaparinux (synthetic pentasaccharide)
│ └── Direct Thrombin Inhibitors (DTIs)
│ ├── Hirudin / Lepirudin (withdrawn)
│ ├── Bivalirudin
│ └── Argatroban
├── ORAL
│ ├── Vitamin K Antagonists (VKAs)
│ │ └── Warfarin
│ └── Direct Oral Anticoagulants (DOACs)
│ ├── Direct thrombin inhibitor: Dabigatran
│ └── Factor Xa inhibitors: Rivaroxaban, Apixaban, Edoxaban
3. Parenteral Anticoagulants
A. Unfractionated Heparin (UFH)
Source & Structure: A heterogeneous mixture of sulfated glycosaminoglycans (mucopolysaccharides) extracted from porcine intestinal mucosa. Strongly acidic due to sulfate and carboxyl groups. Mean MW ~15,000 Da.
Mechanism of Action:
Heparin has no intrinsic anticoagulant activity. It binds to antithrombin (AT), inducing a conformational change that accelerates AT's inactivation of thrombin (IIa) and Factor Xa by ~1000-fold. Only ~1/3 of commercial heparin molecules contain the critical pentasaccharide sequence needed for high-affinity AT binding. UFH inhibits both Xa and IIa equally (anti-Xa:anti-IIa ratio = 1:1) because molecules must be ≥18 saccharide units to bridge AT and thrombin simultaneously. - Goodman & Gilman's Pharmacological Basis of Therapeutics
Pharmacokinetics:
- Route: IV bolus (immediate onset) or subcutaneous (effect in 1-2 hours)
- Half-life: 1-8 hours (dose-dependent, nonlinear kinetics)
- Cleared by saturable mechanism (binds plasma proteins, endothelium) + slower renal excretion
- Does NOT cross the placenta (large, negatively charged molecule)
Monitoring: Activated Partial Thromboplastin Time (aPTT) - therapeutic range is institution-specific due to reagent variability. Anti-Xa levels are an alternative.
Reversal: Protamine sulfate - 1 mg neutralizes 100 units of heparin. Protamine itself is a weak anticoagulant, so overdosing worsens bleeding.
Adverse Effects:
- Bleeding (major risk)
- Heparin-Induced Thrombocytopenia (HIT) - immune-mediated platelet activation via anti-PF4/heparin IgG antibodies; paradoxically causes thrombosis. Occurs in <5% of UFH patients.
- Osteoporosis with prolonged use
- Hypersensitivity (chills, fever, anaphylaxis - due to porcine source)
- Hypoaldosteronism
B. Low Molecular Weight Heparins (LMWHs)
Examples: Enoxaparin, Dalteparin, Tinzaparin (produced by depolymerization of UFH)
Structure: Mean MW ~5000 Da (~1/3 the size of UFH), heterogeneous compounds.
Mechanism: Same pentasaccharide binding to AT, but because most LMWH molecules are too short (<18 saccharide units) to bridge AT and thrombin, they predominantly inhibit Factor Xa only. Anti-Xa:anti-IIa ratio = 2:1 to 3:1. - Goodman & Gilman's
Advantages over UFH:
- Predictable pharmacokinetics (90% bioavailability subcutaneously vs. 30% for UFH)
- Longer half-life (~4 hours)
- No need for routine aPTT monitoring
- Lower HIT risk (<1%)
- Suitable for outpatient use
Monitoring needed in: Renal impairment, obesity, pregnancy (anti-Xa levels at 4 hours post-dose).
Reversal: Protamine sulfate provides only partial neutralization of LMWH (no anti-Xa reversal).
Caution: Renally excreted; dose reduction required in renal insufficiency.
C. Fondaparinux
A synthetic pentasaccharide (MW ~1500 Da) - the minimal sequence of heparin responsible for AT binding.
Mechanism: Selectively inhibits Factor Xa only (anti-Xa:anti-IIa ratio = ∞). Too short to bridge AT and thrombin.
| Feature | UFH | LMWH | Fondaparinux |
|---|---|---|---|
| Mean MW (Da) | 15,000 | 5,000 | 1,500 |
| Target | Xa and IIa | Xa and IIa | Xa only |
| SC Bioavailability | 30% | 90% | 100% |
| Half-life | 1-8 h | 4 h | 17 h |
| Renal excretion | No | Yes | Yes |
| Antidote | Complete (protamine) | Partial | None |
| HIT risk | <5% | <1% | <0.1% |
Table from Goodman & Gilman's, Table 36-1
Uses: DVT/PE treatment, VTE prophylaxis in orthopedic and abdominal surgery.
Caution: Contraindicated in severe renal impairment. No reversal agent available.
D. Direct Thrombin Inhibitors (Parenteral)
These drugs directly bind thrombin's active site, independent of antithrombin. They can inhibit clot-bound thrombin (unlike heparin).
Bivalirudin
- Analog of hirudin (from leech saliva - Hirudo medicinalis)
- Bivalent: binds both the catalytic site and fibrin-recognition site of thrombin (reversibly)
- Half-life: 25 minutes; 80% metabolic, 20% renal clearance
- Used in PCI, and for HIT patients requiring coronary intervention
Argatroban
- Synthetic, derived from L-arginine; monovalent direct thrombin inhibitor
- Half-life: 39-51 minutes; hepatically metabolized
- Used in HIT (both prophylaxis and treatment)
- Monitoring: aPTT; dose reduction in hepatic impairment
- Lippincott Illustrated Reviews: Pharmacology
4. Oral Anticoagulants
A. Warfarin (Vitamin K Antagonist)
Mechanism: Warfarin blocks vitamin K epoxide reductase (VKORC1), preventing recycling of vitamin K epoxide back to its active hydroquinone form. Without active vitamin K, the liver cannot γ-carboxylate glutamate residues on clotting Factors II, VII, IX, X and Proteins C and S, rendering them biologically inactive. - Katzung's Basic & Clinical Pharmacology, 16e
Onset of Action: Delayed 8-12 hours; full effect depends on degradation of pre-formed clotting factors:
- Factor VII: half-life 6 hours (depleted first)
- Factor IX: 24 hours
- Factor X: 40 hours
- Factor II (prothrombin): 60 hours
Important: Warfarin initially depletes Protein C (a natural anticoagulant with a short half-life similar to Factor VII) before fully depleting procoagulant factors, creating a transient hypercoagulable state. This is why heparin bridging is always used for 5-7 days when starting warfarin in an acute thrombotic state.
Monitoring: INR (International Normalized Ratio) - target typically 2.0-3.0 for most indications (2.5-3.5 for mechanical heart valves).
Drug Interactions (extensive):
- Increased anticoagulation: NSAIDs, broad-spectrum antibiotics (reduce gut flora synthesizing vitamin K), amiodarone, metronidazole, fluconazole (CYP2C9 inhibition)
- Decreased anticoagulation: Rifampin, carbamazepine, St. John's Wort (CYP induction), high-dose vitamin K
Adverse Effects:
- Bleeding (principal risk)
- Skin/cutaneous necrosis - rare; occurs at warfarin initiation due to Protein C depletion in patients with underlying Protein C deficiency
- Purple toe syndrome - cholesterol microemboli
- Teratogenicity - crosses the placenta; causes fetal hemorrhage and bone malformations; contraindicated in pregnancy
Reversal:
- Minor bleeding: Hold drug ± oral Vitamin K1
- Major bleeding: IV Vitamin K + 4-factor prothrombin complex concentrate (PCC) or fresh frozen plasma (FFP)
B. Direct Oral Anticoagulants (DOACs)
DOACs offer predictable pharmacokinetics, fixed dosing, no routine monitoring, and fewer drug-food interactions compared to warfarin.
1. Dabigatran (Direct Thrombin Inhibitor)
- Prodrug (dabigatran etexilate) → converted by plasma esterases to active dabigatran
- Inhibits both free and clot-bound thrombin
- Substrate for P-glycoprotein (P-gp); eliminated renally
- Reversal agent: Idarucizumab (monoclonal antibody fragment; binds dabigatran with 350x higher affinity than thrombin)
- Adverse effects: Bleeding, GI upset (dyspepsia, GI bleeding)
- Contraindicated in mechanical prosthetic heart valves
- Avoid in severe renal impairment (CrCl <30 mL/min)
2. Factor Xa Inhibitors
| Drug | Route | Metabolism | Half-life | Renal Excretion |
|---|---|---|---|---|
| Rivaroxaban | Oral | CYP3A4/5, CYP2J2 | 9-13 h | 33% |
| Apixaban | Oral | CYP3A4 | 12 h | 27% |
| Edoxaban | Oral | Minimal hepatic | 10-14 h | 50% |
- Mechanism: Direct inhibition of Factor Xa, reducing thrombin generation
- Reversal agent: Andexanet alfa - a Factor Xa decoy molecule (no procoagulant activity) that competes for drug binding. FDA-approved (2018) for life-threatening bleeding with apixaban or rivaroxaban. Alternative: 4-factor PCC.
- Indications: Stroke prevention in nonvalvular AF, DVT/PE treatment and prevention
- Rivaroxaban also approved for reducing cardiovascular events in CAD/PAD
5. Indications Summary
| Indication | Preferred Agent(s) |
|---|---|
| Acute DVT/PE (initial) | UFH (IV) or LMWH (SC) |
| DVT/PE (long-term) | DOACs (rivaroxaban, apixaban, edoxaban), warfarin |
| Atrial fibrillation (stroke prevention) | DOACs preferred; warfarin if mechanical valve |
| Mechanical heart valves | Warfarin only |
| Pregnancy (VTE) | LMWH (warfarin and DOACs are contraindicated) |
| PCI / acute coronary syndromes | UFH, bivalirudin |
| HIT | Argatroban, bivalirudin (NOT heparin or LMWH) |
| VTE prophylaxis (orthopedic surgery) | LMWH, fondaparinux, or DOACs |
6. Monitoring Summary
| Drug | Test | Target |
|---|---|---|
| UFH | aPTT | 60-100 seconds (1.5-2.5x control) |
| UFH (high-dose) | Anti-Xa | 0.3-0.7 IU/mL |
| LMWH | Anti-Xa (if needed) | 0.5-1.0 IU/mL (peak, 4 hrs post-dose) |
| Warfarin | INR | 2.0-3.0 (most indications) |
| DOACs | None routinely | - |
7. Reversal Agents
| Anticoagulant | Reversal Agent |
|---|---|
| UFH | Protamine sulfate (1 mg per 100 units UFH) |
| LMWH | Protamine (partial; neutralizes anti-IIa, not anti-Xa) |
| Fondaparinux | No approved reversal agent; 4-factor PCC may help |
| Warfarin | Vitamin K + FFP or 4-factor PCC |
| Dabigatran | Idarucizumab |
| Rivaroxaban / Apixaban | Andexanet alfa or 4-factor PCC |
8. Key Contraindications and Cautions
- All anticoagulants: Active major bleeding, recent intracranial hemorrhage, severe uncontrolled hypertension
- Warfarin: Pregnancy (teratogen), unreliable/non-compliant patients
- DOACs: Mechanical heart valves (dabigatran proven harmful), severe renal impairment (varies by drug)
- LMWH/Fondaparinux: Severe renal impairment (CrCl <30 mL/min for LMWH, <20 for fondaparinux)
- Heparin: Prior HIT (absolute contraindication)
Sources:
- Lippincott Illustrated Reviews: Pharmacology, 7e, Chapters 13 (pp. 450-462)
- Katzung's Basic and Clinical Pharmacology, 16e, Chapter 34 (pp. 957-970)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 36 (pp. 731-750)
This is a shared conversation. Sign in to Orris to start your own chat.