osteotomy in torsional deformities
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
torsional deformity osteotomy femoral tibial
Loading Image
Loading Image
Finding Sources
I now have all the necessary material for a comprehensive answer. Let me compile it.
Osteotomy in Torsional Deformities
Overview of Torsional Deformities
Torsional deformities of the lower limb are rotational abnormalities of the femur, tibia, or foot that alter the foot progression angle during gait. The foot progression angle is measured as the angle the foot makes with the line of walking: a positive value = out-toeing; a negative value = in-toeing.
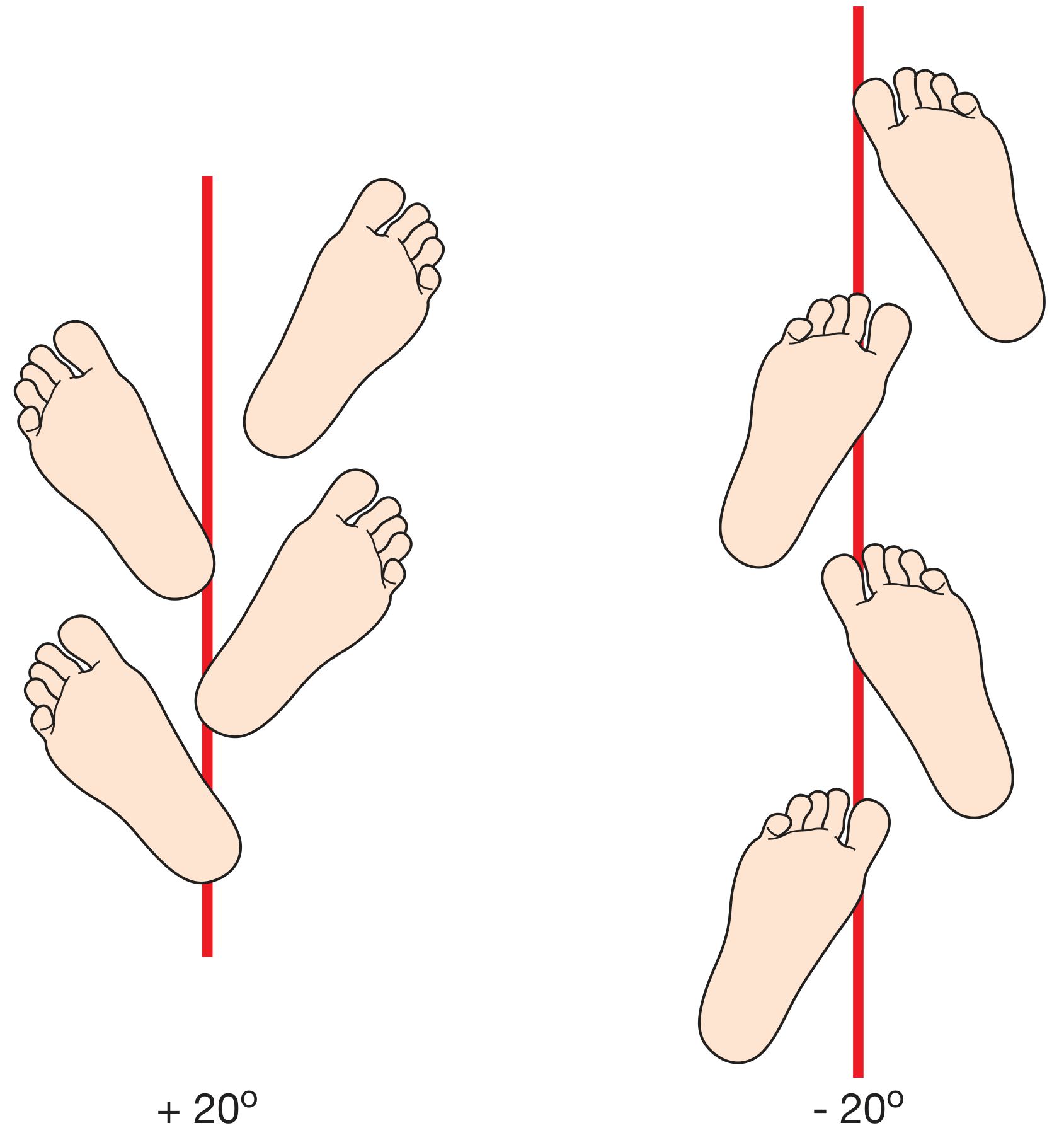
Foot progression angle - Bailey & Love's Short Practice of Surgery, 28th Ed.
Causes of Torsional Deformities
| Type | Cause | Gait |
|---|---|---|
| Femoral | Excessive anteversion | In-toeing |
| Tibial (internal) | Internal tibial torsion | In-toeing (toddlers) |
| Foot | Metatarsus adductus | In-toeing (infants) |
| Femoral | Retroversion | Out-toeing |
| Tibial (external) | External tibial torsion | Out-toeing |
Most torsional deformities in children are bilateral, arising from intrauterine positioning, and deformities are expected to be asymmetric findings that warrant closer evaluation. - Miller's Review of Orthopaedics, 9th Ed.
Clinical Assessment: The Torsional Profile
All assessments are performed with the child prone:
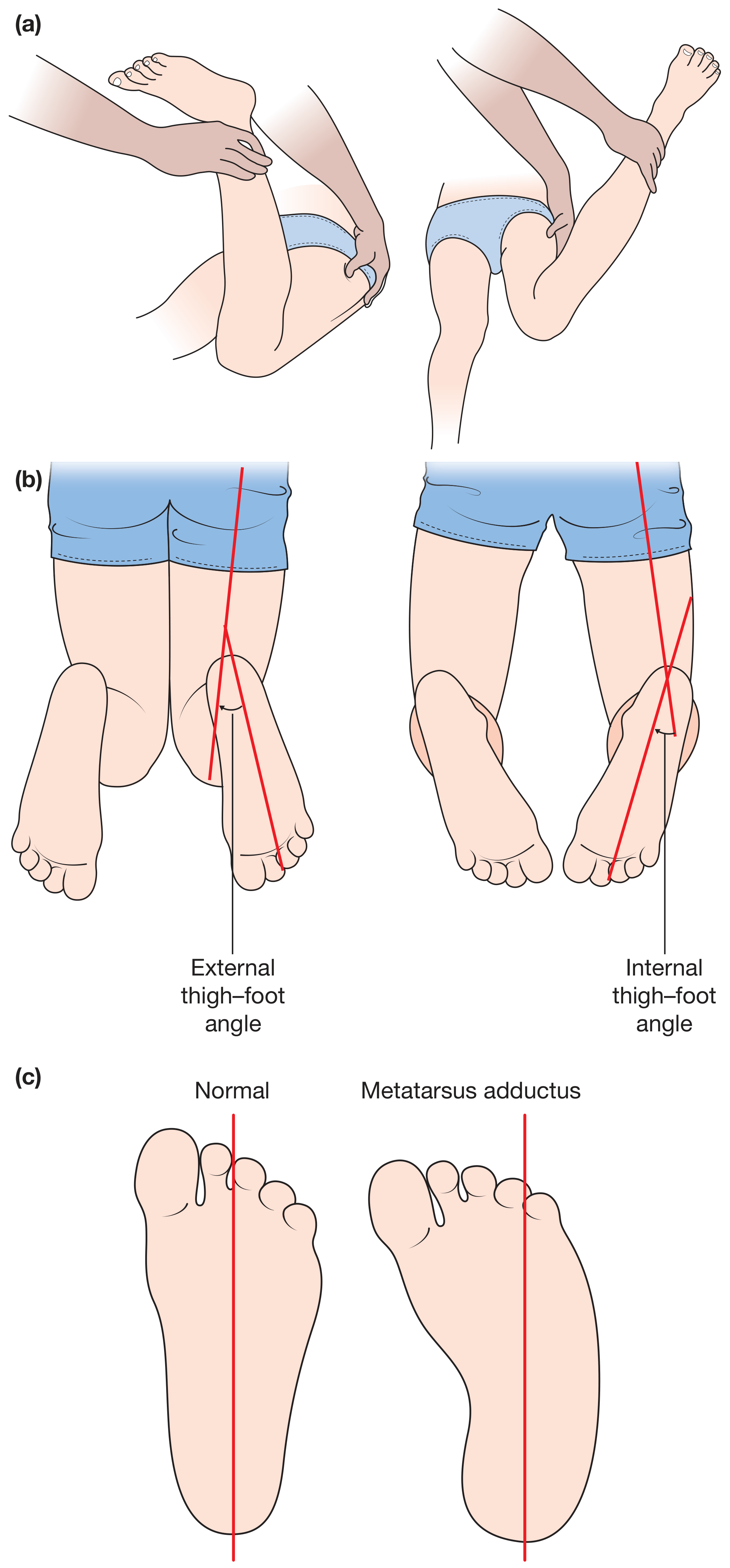
Assessment of the torsional profile - Bailey & Love's Short Practice of Surgery, 28th Ed.
| Measurement | Technique | Normal Values | Significance |
|---|---|---|---|
| Foot-progression angle | Foot vs. straight line | -5 to -20° | Nonspecific rotation |
| Medial hip rotation | Prone hip ROM | 20-60° | >70°: femoral anteversion |
| Lateral hip rotation | Prone hip ROM | 30-60° | <20°: femoral anteversion |
| Thigh-foot angle | Knee bent; foot up | 0 to +20° | < -10°: tibial torsion |
Miller's Review of Orthopaedics, 9th Ed.
Craig's test (trochanteric prominence test) measures the degree of internal rotation when the greater trochanter is at its most prominent position, giving an estimate of femoral anteversion. - Bailey & Love's, 28th Ed.
Natural History and Conservative Management
The vast majority of torsional deformities resolve spontaneously. Operative intervention is reserved for persistent, severe, or functionally disabling cases.
- Femoral anteversion: Corrects spontaneously by age 10. Special shoes, therapy, and derotational braces have never been shown to improve remodeling rates. - Miller's, 9th Ed.
- Internal tibial torsion: Usually resolves with growth by age 4. No treatment needed in the majority. - Bailey & Love's, 28th Ed.
- Metatarsus adductus: ~85% resolve spontaneously. Stretching for flexible feet; serial casting for rigid feet (rare). - Miller's, 9th Ed.
- External tibial torsion: Can worsen with growth; associated with early DJD and patellofemoral malalignment. Rest and rehabilitation first.
Indications for Osteotomy
Surgery is indicated when:
- The deformity persists beyond the expected age of spontaneous resolution (typically age 10-12 for femoral, 7-10 for tibial)
- There is functional impairment (difficulty walking, pain, instability)
- The deformity exceeds threshold angles (see below)
- The child has no ability to externally rotate the extended hip (for femoral anteversion)
Types of Osteotomy by Location
1. Femoral Derotation Osteotomy
Indications:
- Femoral anteversion persisting beyond age 10-11 years with functional impairment - Schwartz's Principles of Surgery, 11th Ed.
- Less than 10 degrees of external hip rotation in older children
- Miserable malalignment syndrome (femoral anteversion + compensatory external tibial torsion causing patellofemoral pain)
Procedure:
- Rotational (derotational) femoral osteotomy - typically an intertrochanteric or subtrochanteric osteotomy
- The femur is externally rotated (derotated) to correct excessive anteversion
- In cerebral palsy with hip subluxation, a varus derotation osteotomy (VDRO) is performed, reducing the neck-shaft angle to 120 degrees in ambulatory patients - Campbell's Operative Orthopaedics, 15th Ed. 2026
VDRO in Cerebral Palsy - specific technique considerations:
- Used when migration percentage (MP) > 40-60%, combined with pelvic osteotomies and soft-tissue release
- A femoral varus and derotation (external rotation) osteotomy, often combined with femoral shortening, reduces the neck-shaft angle
- Acetabular procedures (Salter, Pemberton, Dega, Ganz, Steel) may be added to correct associated acetabular dysplasia
- Careful matching of acetabular procedure to the specific deformity is essential - Campbell's, 15th Ed.
Post-fracture torsional deformity:
- Torsional deformities occur in one-third to two-thirds of children with femoral shaft fractures; most are mild (<10 degrees) and asymptomatic, rarely requiring treatment
- Corrective osteotomy for significant angular or torsional malunion should be delayed at least 1 year unless function is impaired - Campbell's, 15th Ed.
2. Supramalleolar Osteotomy (for tibial torsion)
Indications:
- Internal tibial torsion: Operative correction rarely necessary except in severe cases, addressed with supramalleolar osteotomy when the child is 7-10 years of age - Miller's, 9th Ed.
- External tibial torsion: Supramalleolar osteotomy if child is older than 8-10 years and external tibial torsion >40 degrees - Miller's, 9th Ed.
Technique: The osteotomy is performed just above the ankle (distal tibia/fibula), and the distal segment is rotated to the desired alignment. This location allows rotational correction with minimal shortening and good healing potential.
3. Combined/Multi-level Osteotomy
For miserable malalignment syndrome or neuromuscular conditions (cerebral palsy, myelomeningocele):
- Both femoral and tibial osteotomies may be required simultaneously
- In cerebral palsy, malalignment from excessive femoral anteversion, external tibial torsion, and genu valgum may require osteotomy for skeletal realignment, in combination with lateral retinacular release for patellofemoral instability - Campbell's, 15th Ed.
4. Osteotomy in Osteogenesis Imperfecta
In OI with genu varum, the femur, tibia, and fibula are all commonly deformed with lateral bowing plus internal torsion. Osteotomy (often the Sofield-Millar multiple osteotomy with intramedullary rodding) corrects both angular and rotational deformity simultaneously.
Summary Table: Osteotomy Decision Guide
| Deformity | Osteotomy Type | Timing | Threshold |
|---|---|---|---|
| Femoral anteversion | Femoral derotation (intertrochanteric/subtrochanteric) | Age 10-11+ | Functional impairment, no ext. rotation |
| Internal tibial torsion | Supramalleolar | Age 7-10 | Severe, symptomatic |
| External tibial torsion | Supramalleolar | Age 8-10+ | >40 degrees |
| CP hip subluxation | VDRO ± acetabular osteotomy | Individualized | MP >40-60% |
| Post-fracture malunion | Corrective osteotomy | >1 year post-fracture | Functional impairment |
Key Principles
- Wait for spontaneous resolution - most torsional deformities correct with growth
- Age matters - osteotomy is not indicated in young children; near-skeletal maturity is preferred
- Bilateral deformities are expected; asymmetric findings should raise concern for pathology
- Functional impairment (not cosmesis alone) is the primary surgical indication
- Neuromuscular conditions (CP, myelomeningocele) lower the threshold for surgery due to loss of compensatory mechanisms
Sources: Campbell's Operative Orthopaedics 15th Ed. 2026; Miller's Review of Orthopaedics 9th Ed.; Bailey & Love's Short Practice of Surgery 28th Ed.; Schwartz's Principles of Surgery 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.