Juvenile nasal angiofibroma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"juvenile nasopharyngeal angiofibroma"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive material. Here is a detailed, well-organized summary of Juvenile Nasopharyngeal Angiofibroma (JNA).
Juvenile Nasopharyngeal Angiofibroma (JNA)
Overview
Juvenile angiofibroma (JA) is a benign but locally aggressive fibrovascular tumor that occurs almost exclusively in adolescent males, typically between ages 8 and 20. Despite being histologically benign, it can erode bone, invade adjacent spaces, and even extend intracranially. It is rare overall but notably more common in northern India (reasons unclear).
Pathology and Histology
Histologically, JA consists of:
- Numerous thin-walled vascular spaces lined by a single layer of endothelial cells, with no smooth muscle in the vessel walls (making them unable to constrict and explaining the severe, uncontrolled hemorrhage)
- These vascular channels are embedded in a dense collagenous fibrous stroma containing bland fibroblasts
- A mixed arterio-capillary component with muscularized channels also exists
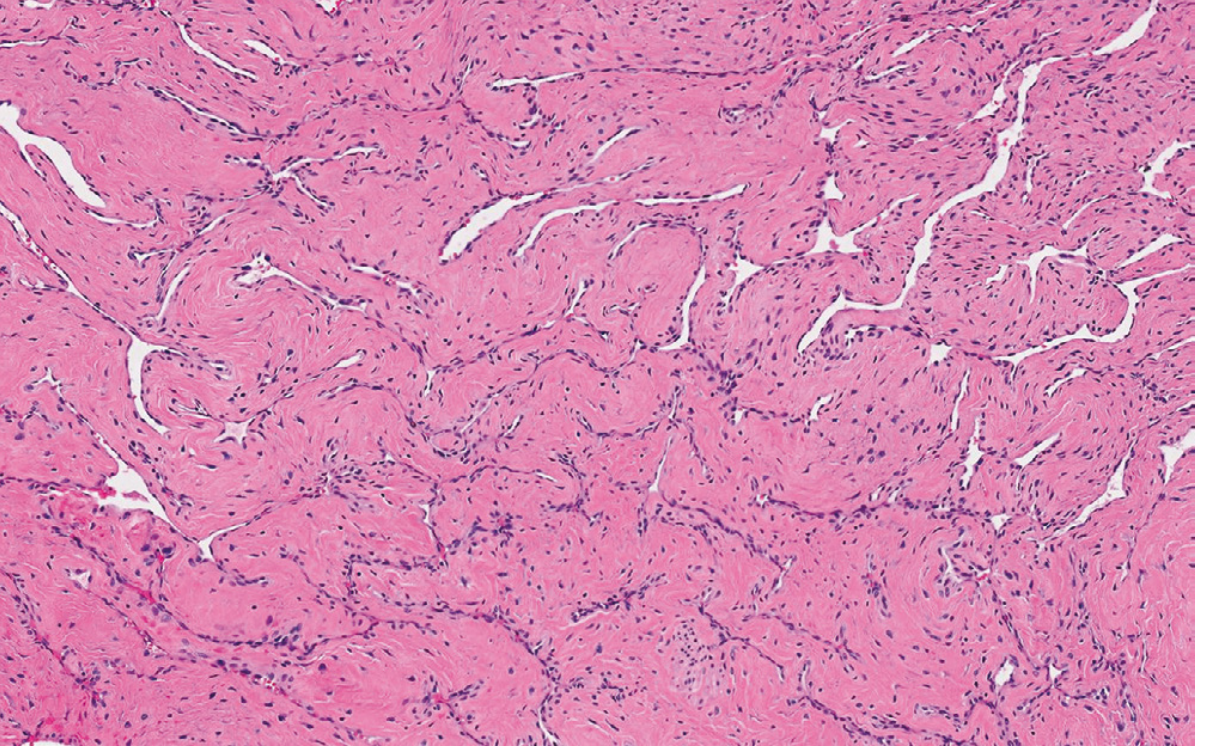
Histopathology: thin-walled vessels lined by a single endothelial layer set in dense collagenous stroma - Robbins, Cotran & Kumar Pathologic Basis of Disease
Some authorities classify JA as a vascular malformation (hamartoma) rather than a true neoplasm, based on immunohistochemical and electron microscopy findings.
Molecular Pathology
- CTNNB1 mutations (encoding β-catenin) are present in the majority of sporadic cases - activating the Wnt/β-catenin pathway
- JA can also arise syndromically in familial adenomatous polyposis (FAP), driven by germline APC mutations (also leading to β-catenin activation)
- Other molecular markers implicated: androgen receptor, bFGF, H-Ras, IL-6, c-Kit, c-Myc, PDGFa, TP53, VEGFA, and β-catenin show variable expression
- VEGF signaling and FGFR pathway are upregulated, suggesting angiogenic drive
Origin and Pathogenesis
Site of origin: The pathognomonic epicenter is the pterygopalatine fossa (PPF), specifically at or near the sphenopalatine foramen. Recent imaging evidence points to the base of the pterygoid process or superior choana as the exact origin point.
Embryological theory (Schick et al.): JA may arise from incomplete regression of the first branchial arch artery. During embryogenesis (days 22-24), branchial arch arteries connect the ventral and dorsal aortas; regression forms a vascular plexus that may leave remnants - explaining the characteristic blood supply from maxillary and sphenopalatine arteries, with persistent connections to the internal carotid pathway.
Hormonal influence: Target cells of nasal mucosa are thought to develop into muscularized vascular channels secondary to testosterone stimulation and estrogen hypersensitivity at puberty - explaining the exclusive occurrence in adolescent males.
Routes of Spread
JA characteristically spreads along foramina, fissures, and natural pathways of the skull base:
| Direction | Path | Result |
|---|---|---|
| Medial/anterior | Sphenopalatine foramen | Nasopharynx, nasal cavity |
| Superior | Along vidian nerve | Floor of sphenoid sinus |
| Lateral | Pterygomaxillary fissure | Infratemporal fossa |
| Anterior | Pushes posterior maxillary wall | Bulges forward |
| Superior-posterior | Via orbit or superior orbital fissure | Intracranial extension, middle cranial fossa |
| Direct bone | Cancellous invasion of pterygoid root | Erosion of greater wing, MCF floor |
Clinical Features
- Recurrent severe epistaxis - often massive and the presenting complaint; may cause anemia
- Nasal obstruction - progressive, usually unilateral at first
- Purulent rhinorrhea
- Facial swelling / "frog face" deformity (anterior bulging)
- Loss of vision - from compression of optic nerve by superior/orbital extension
- Conductive hearing loss (eustachian tube compression)
- Cheek anesthesia (V2 involvement in ITF extension)
- Intracranial extension: headache, cranial nerve palsies
Key clinical pearl: These symptoms in a young male should always raise suspicion. Biopsy should be avoided unless clinical and radiological examination is non-diagnostic - due to severe bleeding risk.
Imaging
CT (Computed Tomography)
- Defines bony erosion and extent
- Widening of the pterygopalatine fossa - pathognomonic finding
- Erosion of the medial pterygoid plate
- Erosion in the region of the vidian canal aperture
- Anterior bowing of the posterior maxillary sinus wall
MRI (Magnetic Resonance Imaging)
- Defines soft-tissue extent and intracranial/orbital involvement
- Contrast-enhanced T1 shows diffuse or patchy enhancement
- Identifies dural enhancement suggesting intracranial spread
- Flow voids within the tumor on T2 (highly vascular lesion)
Pathognomonic radiological sign:
A nasal mass + widened pterygopalatine fossa in an adolescent male = pathognomonic for JNA
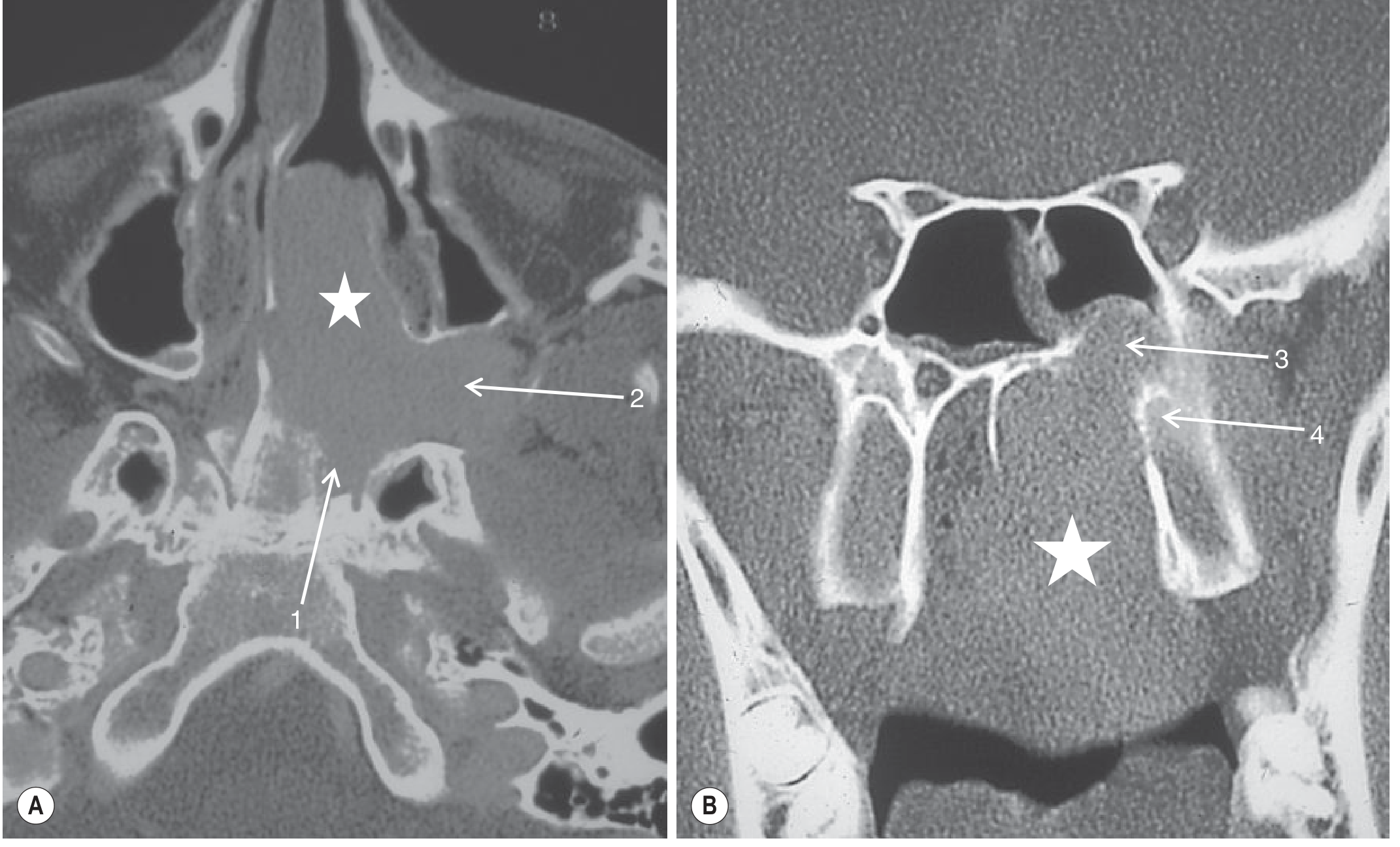
CT of JNA: (A) Axial - tumor (star) filling nasal cavity, eroding sphenoid at vidian canal aperture (1), widening the PPF (2). (B) Coronal - eroding vidian canal (3) and medial pterygoid plate (4) - Grainger & Allison's Diagnostic Radiology
DSA (Digital Subtraction Angiography)
- Shows enlarged intratumoral vessels with a mixed pattern of arterioles
- Intense inhomogenous tumor blush in the venous phase showing full extent
- Blood supply primarily from external carotid artery branches (maxillary artery, sphenopalatine artery)
- If there is intracranial extension: internal carotid artery branches may contribute
Staging Systems
Several staging systems exist; the Andrews-Fisch and Radkowski systems are commonly used. The general scheme based on Cummings:
| Stage | Description |
|---|---|
| I | Confined to nasal cavity and nasopharynx, no bony erosion |
| II | Extension into PPF, maxillary sinus, ethmoid, sphenoid (with or without limited bony erosion) |
| III | Extension into infratemporal fossa, orbit, parasellar region (lateral to cavernous sinus) |
| IV | Intracranial extension (cavernous sinus, optic chiasm, pituitary fossa) |
Management
Pre-operative Embolization
- Performed 24-48 hours before surgery (angiography + embolization in same session)
- Agents: PVA particles (transarterial) or NBCA/Onyx (transarterial or direct tumor puncture)
- Direct puncture with Onyx has improved the degree of devascularization
- Reduces intraoperative blood loss and tumor size
- Intracranial supply from ICA increases embolization risk (neurological deficit)
- For smaller, localized lesions - some centers now consider embolization unnecessary before endoscopic resection
Surgical Approaches
- Endoscopic resection - now preferred for Stages I-II and selected Stage III lesions (smaller tumors without significant spread)
- Midfacial degloving - allows ligation of the feeding maxillary artery; good exposure without facial scar
- Lateral rhinotomy - older open approach, still used for larger lesions
- Both open approaches allow ligation of the maxillary artery
Radiation Therapy
- Reserved for unresectable or recurrent disease, especially with intracranial extension
- Risk of radiation-induced malignancy in young patients limits its use
Hormonal Therapy
- Estrogen therapy has been used historically to reduce vascularity pre-operatively, but is largely abandoned due to side effects
Medical / Targeted Therapy
- Flutamide (anti-androgen) has been explored given androgen receptor expression
- Anti-VEGF agents (given VEGFA upregulation) are under investigation
Prognosis and Outcomes
- Recurrence rate: up to 20% after surgical resection
- Mortality: approximately 9% of cases can be fatal (from massive hemorrhage or intracranial spread)
- Spontaneous regression has been reported, particularly in older adolescents - consistent with the hormonal dependence theory
- Residual disease after surgery can be observed with imaging if it remains stable (no further growth mandate) - serial contrast-enhanced MRI is the standard follow-up modality
Key Points Summary
| Feature | Detail |
|---|---|
| Epidemiology | Adolescent males, 8-20 years, higher incidence in North India |
| Histology | Thin-walled vessels + fibrous stroma; no smooth muscle in vessel walls |
| Origin | Pterygopalatine fossa / sphenopalatine foramen |
| Key genetics | CTNNB1 / APC mutations (β-catenin pathway) |
| Symptoms | Epistaxis, nasal obstruction, facial swelling |
| Pathognomonic sign | Widened PPF on CT in adolescent male |
| Blood supply | ECA (maxillary/sphenopalatine arteries) ± ICA if intracranial |
| Biopsy | AVOID - severe bleeding risk |
| Treatment | Pre-op embolization + surgical excision (endoscopic preferred) |
| Recurrence | ~20% |
Sources:
- Cummings Otolaryngology Head and Neck Surgery - JUVENILE ANGIOFIBROMA section (pp. 988-991)
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Sinonasal Angiofibroma, p. 690
- Grainger & Allison's Diagnostic Radiology - Juvenile Angiofibroma (p. 1605)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 - Juvenile Nasopharyngeal Angiofibroma
- Bailey and Love's Short Practice of Surgery, 28th Ed. - Angiofibroma, p. 9684
Jna
Asking for Preferences
Here is the complete, detailed summary of Juvenile Nasopharyngeal Angiofibroma (JNA):
Juvenile Nasopharyngeal Angiofibroma (JNA)
Overview
JNA is a benign but locally aggressive fibrovascular tumor occurring almost exclusively in adolescent males (ages 8-20). Despite being histologically benign, it erodes bone, invades adjacent spaces, and can extend intracranially. It is rare globally but notably more common in North India.
Pathology and Histology
Histologically, JNA consists of:
- Thin-walled vascular spaces lined by a single layer of endothelial cells with no smooth muscle in vessel walls - this is why bleeding is uncontrollable (vessels cannot vasoconstrict)
- Embedded in a dense collagenous fibrous stroma with bland fibroblasts
- Some authorities classify it as a vascular malformation / hamartoma rather than a true neoplasm
Sinonasal angiofibroma - thin-walled vessels lined by a single endothelial layer, separated by dense collagenous stroma (Robbins Pathology)
Molecular Pathology
| Marker | Significance |
|---|---|
| CTNNB1 mutation | β-catenin activation - majority of sporadic cases |
| APC gene mutation | Syndromic JNA in FAP (familial adenomatous polyposis) |
| Androgen receptor | Explains male-only occurrence, testosterone dependence |
| VEGFA upregulation | Drives angiogenesis; potential therapeutic target |
| FGFR pathway | Also implicated in angiogenesis |
| bFGF, H-Ras, IL-6, c-Kit, c-Myc, PDGFa, TP53 | Variable expression; molecular heterogeneity |
Pathogenesis and Origin
Site of origin: Pathognomonic epicenter at the pterygopalatine fossa (PPF), specifically the sphenopalatine foramen. Recent imaging data suggests the base of the pterygoid process or superior choana may be more precise.
Embryological theory (Schick et al.): Arises from incomplete regression of the first branchial arch artery (normally regresses by birth via a vascular plexus). Remnants explain the characteristic blood supply from the maxillary and sphenopalatine arteries, with persistent connections to the ICA pathway.
Hormonal theory: Target cells of nasal mucosa develop into muscularized vascular channels under testosterone stimulation and estrogen hypersensitivity at puberty - explaining the exclusive occurrence in adolescent males and the documented post-pubertal regression.
Routes of Spread
JNA travels along foramina, fissures, and natural pathways:
| Direction | Pathway | Space Entered |
|---|---|---|
| Medial / anterior | Sphenopalatine foramen | Nasopharynx, nasal cavity |
| Superior | Along vidian nerve | Floor of sphenoid sinus |
| Lateral | Pterygomaxillary fissure | Infratemporal fossa (ITF) |
| Anterior | Pushes posterior maxillary wall | Anterior bulge ("frog face") |
| Superior-lateral | Via orbit / superior orbital fissure | Intracranial middle cranial fossa |
| Direct bone | Cancellous invasion of pterygoid root | Erosion of greater wing / MCF floor |
Clinical Features
Cardinal symptoms:
- Recurrent severe epistaxis - uncontrolled, may cause anemia
- Progressive nasal obstruction - usually unilateral initially
- Purulent rhinorrhea
Advanced symptoms:
- Facial swelling / "frog face" deformity (anterior bulge of cheek)
- Visual loss - optic nerve compression from orbital/superior extension
- Conductive hearing loss (Eustachian tube obstruction)
- Cheek hypoesthesia (V2, from ITF involvement)
- Headache and cranial nerve palsies (intracranial extension)
Key pearl: These symptoms in a young male = always suspect JNA. Biopsy must be avoided unless imaging is non-diagnostic - risk of catastrophic hemorrhage.
Imaging
CT
- Defines bony erosion and tumor extent
- Widened pterygopalatine fossa - pathognomonic finding
- Erosion of the medial pterygoid plate
- Erosion at the vidian canal aperture
- Anterior bowing of the posterior maxillary sinus wall
MRI (with contrast)
- Best for soft-tissue extent, orbital, intracranial involvement
- Diffuse/patchy enhancement with contrast
- Flow voids on T2 (reflects high vascularity)
- Dural enhancement = intracranial spread
- Complements CT for preoperative planning
DSA (Digital Subtraction Angiography)
- Enlarged intratumoral vessels + intense inhomogenous tumor blush in venous phase
- Primary supply: ECA branches (maxillary artery, sphenopalatine artery)
- ICA contribution if intracranial spread present
- Used as part of pre-operative embolization
CT of JNA: (A) Axial - tumor (★) filling nasal cavity, widening PPF (2), eroding sphenoid at vidian canal (1). (B) Coronal - eroding vidian canal aperture (3) and medial pterygoid plate (4). - Grainger & Allison's Diagnostic Radiology
Pathognomonic radiological finding:
Nasal mass + widened pterygopalatine fossa in an adolescent male = JNA until proven otherwise
Staging Systems
Multiple systems exist; the Andrews-Fisch and Radkowski systems are most widely cited. General staging framework (Cummings):
| Stage | Extent |
|---|---|
| I | Limited to nasal cavity and nasopharynx; no or minimal bony erosion |
| II | Extension into PPF, maxillary sinus, ethmoid or sphenoid sinus; limited bone erosion |
| III | Extension into infratemporal fossa, orbit, parasellar region lateral to cavernous sinus |
| IV | Intracranial extension involving cavernous sinus, optic chiasm, or pituitary fossa |
Management
Step 1 - Pre-operative Embolization
- Performed 24-48 hours before surgery
- Transarterial: PVA particles or NBCA liquid embolic (for ECA-supplied tumors)
- Direct puncture: Onyx injection - improved devascularization, used when ICA involvement increases transarterial risk
- Goals: reduce intraoperative blood loss, induce tumor shrinkage, improve surgical access
- Smaller Stage I-II lesions: some centers now omit embolization before endoscopic resection
- ICA supply = higher risk of neurological deficit from embolization
Step 2 - Surgical Resection
| Approach | Indication | Notes |
|---|---|---|
| Endoscopic | Stage I-II, selected Stage III (no significant spread) | Now the preferred approach; reduced morbidity, no external scar |
| Midfacial degloving | Stage II-III, larger lesions | No external incision; allows maxillary artery ligation |
| Lateral rhinotomy | Larger/advanced lesions | Traditional open approach |
| Combined cranio-facial | Stage IV (intracranial extension) | Requires neurosurgical collaboration |
Both open approaches allow direct ligation of the feeding maxillary artery.
Step 3 - Adjuvant Options
| Modality | Role |
|---|---|
| Radiotherapy | Unresectable or recurrent disease with intracranial extension; risk of secondary malignancy limits use in young patients |
| Flutamide (anti-androgen) | Investigated given androgen receptor expression; pre-operative volume reduction |
| Anti-VEGF agents | Under investigation given VEGFA upregulation |
| Estrogen therapy | Historical, now largely abandoned |
Prognosis
| Parameter | Value |
|---|---|
| Recurrence after surgery | Up to 20% |
| Potentially fatal cases | ~9% (from massive hemorrhage or intracranial invasion) |
| Spontaneous regression | Documented post-puberty (hormonal dependence) |
| Follow-up | Serial contrast-enhanced MRI; residual stable disease may be observed |
Quick-Reference Summary
| Feature | Key Point |
|---|---|
| Who gets it | Adolescent males, 8-20 yrs; commoner in North India |
| Histology | Thin-walled vessels (no smooth muscle) + fibrous stroma |
| Origin | Pterygopalatine fossa / sphenopalatine foramen |
| Genetics | CTNNB1 (sporadic); APC (FAP-associated) |
| Presenting symptoms | Epistaxis + nasal obstruction |
| Pathognomonic radiology | Widened PPF on CT in adolescent male |
| Blood supply | ECA (maxillary/sphenopalatine) ± ICA |
| Biopsy | Avoid - catastrophic bleeding risk |
| Treatment | Pre-op embolization + surgical resection (endoscopic preferred) |
| Recurrence rate | ~20% |
Sources: Cummings Otolaryngology (pp. 988-991), Robbins Pathology (p. 690), Grainger & Allison's Diagnostic Radiology (p. 1605), Scott-Brown's Otorhinolaryngology Vol. 1, Bailey & Love's Surgery 28th Ed.
Inverted papilloma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"inverted papilloma" AND sinonasal
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed. Here is the comprehensive review:
Sinonasal Inverted Papilloma
Definition and Overview
Inverted papilloma (IP) is a benign but locally aggressive epithelial tumor arising from the Schneiderian mucosa (respiratory epithelium) lining the nasal cavity and paranasal sinuses. It is the most common form of sinonasal papilloma and the second most frequent benign tumor of the sinonasal tract after osteoma.
- Incidence: 0.74 to 2.3 new cases per 100,000 per year; represents 0.4-4.7% of all surgically removed nasal tumors
- Sex: Male predominance - M:F ratio of 2-4:1
- Age: Most common in the 5th and 6th decades of life (middle-aged adults)
Types of Sinonasal Papilloma
| Type | Also Called | Key Features |
|---|---|---|
| Inverted (endophytic) | Inverted papilloma | Most common; grows inward into stroma; EGFR mutations |
| Oncocytic | Cylindrical cell papilloma | KRAS mutations (never found in IP); intermediate behavior |
| Exophytic | Fungiform papilloma | Grows outward; HPV 6/11; least aggressive |
These are distinct entities with different mutations: EGFR = inverted; KRAS = oncocytic. This distinction is preserved even in malignant transformation.
Histopathology
The hallmark is epithelium inverting downward (endophytically) into the underlying stroma:
- Hyperplastic ribbons of multilayered epithelium grow inward in a bulbous, pushing pattern
- The epithelium is a mixture of squamous cells, ciliated columnar cells, and mucus-secreting (muco-cyte) cells, with transmigrating neutrophils
- A distinct, intact basement membrane is maintained throughout (distinguishes it from carcinoma)
- The surface is lined by thin respiratory epithelium while the underlying stroma contains multiple nodules of thick neoplastic epithelium growing inward
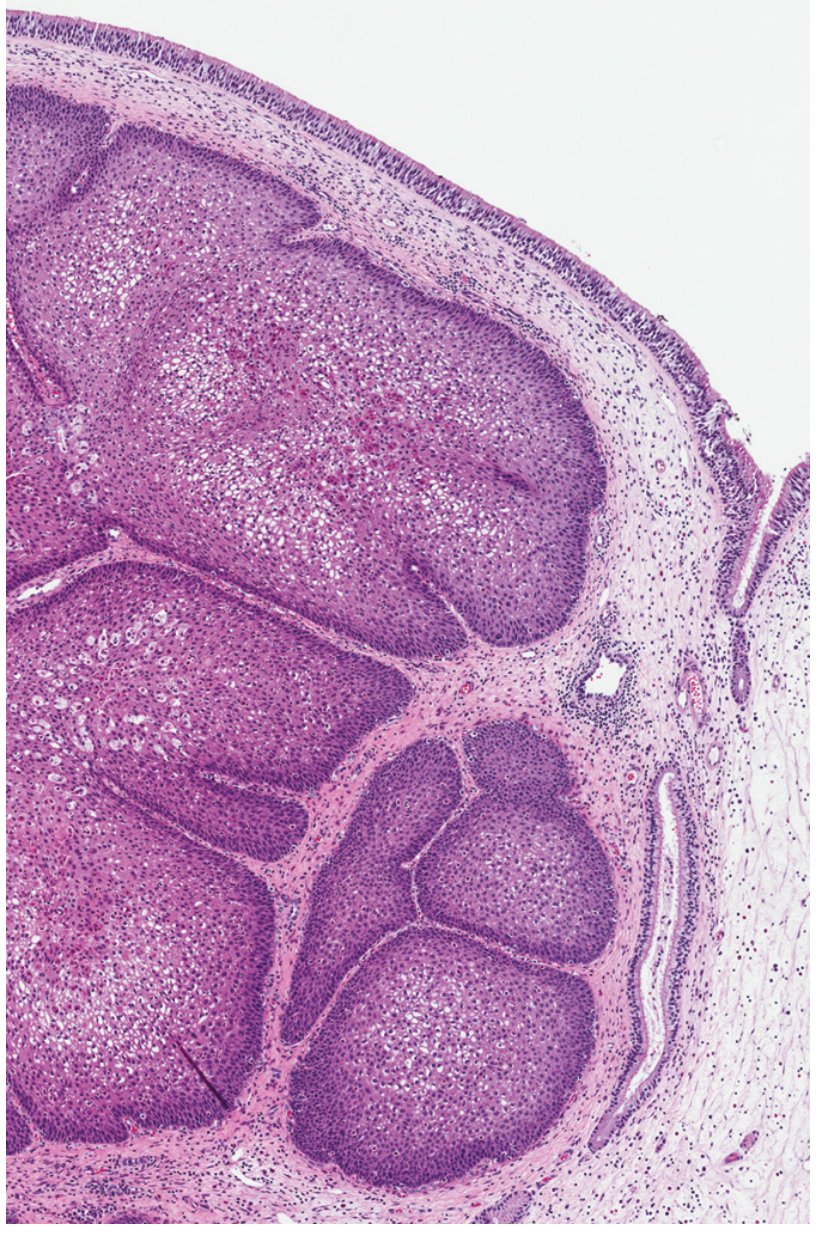
Inverted papilloma: thin surface respiratory epithelium overlying multiple nodules of thick neoplastic epithelium growing inward into the stroma - Robbins, Cotran & Kumar Pathologic Basis of Disease
Molecular Pathology and Etiology
Key Molecular Drivers
| Marker | Significance |
|---|---|
| EGFR mutations (activating) | Present in majority of IPs; also preserved in carcinoma ex-IP - the defining molecular alteration |
| KRAS mutations | Found in oncocytic papillomas ONLY - never in inverted papilloma |
| HPV (types 6, 11) | Low-risk HPV DNA found in ~13% of IPs; role remains controversial (colonizer vs. etiologic agent) |
| HPV high-risk (16, 18) | Found in dysplasia (56%) and carcinoma ex-IP (55%) in older studies; but transcriptionally active HPV not confirmed in recent studies |
HPV - The Controversy
The role of HPV in IP is debated. A large meta-analysis (Lawson et al.) found overall HPV incidence of 22-26%, higher in malignant transformation, suggesting an etiologic role. However, more recent studies using viral mRNA in situ hybridization to detect transcriptionally active HPV found it in none of 52 IPs - suggesting most carcinomatous transformation is driven by non-HPV mechanisms (Rooper et al.).
A 2025 meta-analysis (PMID 39739414) specifically examined HPV infection and IP recurrence.
Environmental Risk Factors
- Organic solvent exposure - significantly associated with IP (dose-response relationship)
- Smoking - not associated with development, but confers a 12-fold higher risk of malignant transformation (26.4% vs. 2.8% in smokers vs. non-smokers; p<0.001)
- Alcohol - no demonstrated association
Sites of Origin
| Site | Frequency |
|---|---|
| Ethmoid region | 48% |
| Lateral nasal wall + maxillary sinus (especially medial wall / fontanelles) | 28% |
| Maxillary sinus (medial wall, fontanelle region) | Most common single site |
| Frontal sinus | ~2.5% |
| Sphenoid sinus | Rare primary |
| Bilateral | Exceptional (rare) |
| Multi-site involvement (at presentation) | ~30% of cases |
Bilateral involvement of the frontal sinus is not uncommon (16%).
Clinical Features
Presenting symptoms:
- Unilateral nasal obstruction with watery rhinorrhea - most common symptom
- Unilateral chronic rhinosinusitis - headache, facial pressure/pain from sinus drainage obstruction
- Epistaxis (less common than in JNA)
Advanced disease:
- Epiphora (lacrimal obstruction)
- Proptosis and diplopia - orbital involvement; also raises suspicion for malignant transformation
- Invasion of orbit or cranial vault in locally aggressive cases
Endoscopic appearance:
- Pale, polypoid mass with a papillary or cerebriform (brain-like) surface protruding from the middle meatus
- Coexisting inflammatory polyps may make diagnosis trickier
- Biopsy is required for definitive histology (unlike JNA where biopsy is avoided)
Imaging
CT
- Primary modality; defines bony involvement and extent
- Unilateral middle meatal mass with ostiomeatal pattern opacification
- Focal hyperostosis at the site of tumor attachment - useful for identifying the origin
- Calcification in 10% of cases at the attachment site
- Characteristic lobulated outline
- Bony thickening of sinus roof at insertion
MRI (with gadolinium)
- Superior to CT for differentiating tumor from retained secretions/inflammatory mucosa
- Cerebriform/columnar pattern on T1 gadolinium-enhanced MRI - pathognomonic for IP
- Reflects alternating parallel folds of cellular metaplastic epithelium and less cellular stroma
- Best for assessing frontal sinus involvement (distinguishes tumor from obstructed mucus)
- Preferred for detecting recurrence (CT used for initial staging)
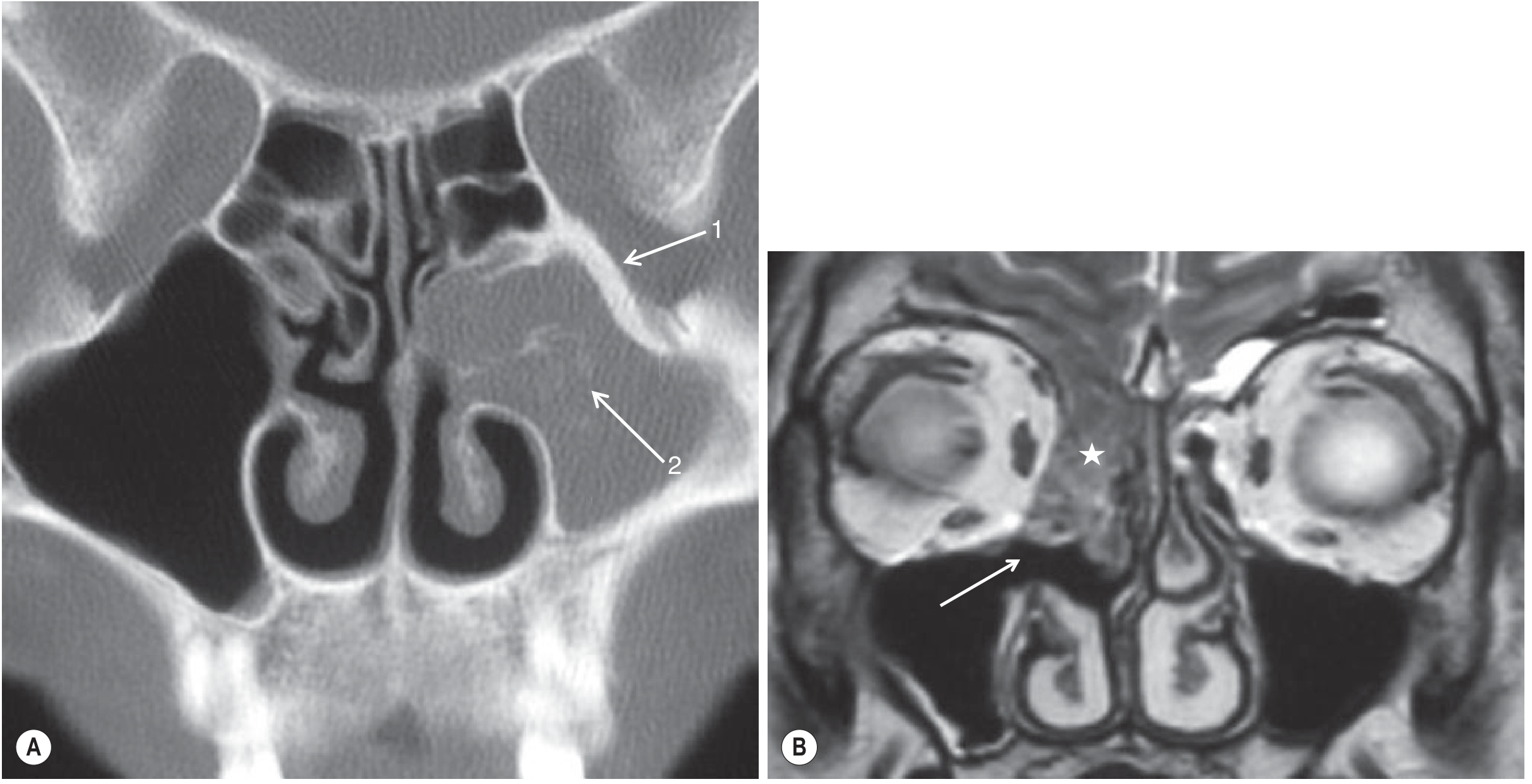
CT and MRI of inverted papilloma: (A) Coronal CT - unilateral antral mass, bony thickening of the roof (1) and calcification (2). (B) Coronal T2 MRI - prior middle meatal antrostomy (white arrow) and recurrent IP (white star) - Grainger & Allison's Diagnostic Radiology
Malignant Transformation
This is the most feared complication:
- Overall rate: 5-15% (Cummings); Robbins cites up to 5%
- Synchronous carcinoma (present at time of IP diagnosis) is more common than metachronous (arising after initial treatment)
- Vast majority are squamous cell carcinomas (SCC)
- Rare associated malignancies: sinonasal undifferentiated carcinoma (SNUC), mucoepidermoid carcinoma, verrucous carcinoma
- Risk factors for malignant transformation:
- Smoking (12x increased risk)
- High-risk HPV subtypes (controversial)
- Recurrent disease
Staging (Krouse Classification - most widely used)
| Stage | Description |
|---|---|
| T1 | Tumor confined to nasal cavity; no extension to sinuses; no malignancy |
| T2 | Tumor extends to ethmoid sinuses and/or medial maxillary sinus, superior or inferior walls; no malignancy |
| T3 | Tumor extends to lateral, inferior, superior, anterior, or posterior walls of maxillary sinus; sphenoid or frontal sinuses; no malignancy |
| T4 | Any tumor with malignancy, OR tumor extends outside the sinonasal tract (orbit, intracranial, pterygomaxillary space) |
Treatment
Principle
Complete surgical excision with subperiosteal dissection at the site of attachment + drilling of the underlying bone at the point of insertion. The margin of surgery is dictated by the site of origin.
Surgical Approaches
| Approach | Indication | Features |
|---|---|---|
| Endoscopic sinus surgery (ESS) | T1, T2, selected T3; mainstay of modern treatment | Low morbidity, no facial incision, excellent visualization |
| Endoscopic medial maxillectomy | Maxillary sinus origin | Ranges from simple antrostomy (Type A) to Sturmann-Canfield procedure (Type D) with removal of anterior maxillary wall |
| "TuNa-saving" technique | Inferior lateral/anterior maxillary wall origin | Preserves inferior turbinate head + nasolacrimal duct; reduces epiphora/dacryocystitis |
| Prelacrimal approach | Maxillary sinus; difficult access cases | Removes bone between lacrimal pathway and piriform aperture; full sinus access, mucosal preservation |
| Lateral rhinotomy / medial maxillectomy | Advanced T3, failed endoscopic approach | External incision; older standard |
| Midfacial degloving | Large or recurrent T3-T4 | No facial scar; wide exposure |
Modern Trend - Pedicle-Oriented Resection
A shift toward conservative pedicle-oriented resection (Landsberg 2008; Kamel, Pagella) focuses surgery only on the point of insertion of the lesion rather than the entire involved mucosa:
- Tumor debulked first to identify the stalk/origin
- Subperiosteal dissection + bone drilling limited to the attachment point only
- Equal recurrence rates to radical demucolization but shorter operative times and fewer complications
Recurrence and Follow-up
- Recurrence rate: 0-30% depending on approach; often due to residual disease rather than true recurrence
- HPV DNA in adjacent normal-appearing mucosa may contribute to recurrence (explains why complete field resection was historically advocated)
- Smoking is an independent risk factor for recurrence
- Follow-up: Regular nasal endoscopy + MRI (preferred over CT for detecting early recurrence)
- Endoscopic surveillance is the standard; CT used mainly for initial staging
Key Summary Table
| Feature | Detail |
|---|---|
| Type | Benign, locally aggressive; Schneiderian origin |
| Who gets it | Males, 5th-6th decade, M:F = 2-4:1 |
| Commonest site | Lateral nasal wall / maxillary sinus (medial wall) |
| Histology | Endophytic (inward-growing) epithelial ribbons, intact BM, mixed squamous/columnar/mucocytes |
| Pathognomonic finding | Cerebriform pattern on MRI |
| Imaging sign | Focal hyperostosis at attachment site on CT |
| Key mutation | EGFR (inverted); KRAS (oncocytic - NOT inverted) |
| HPV | Low-risk types 6/11; role controversial |
| Malignant transformation | 5-15%; mostly SCC; smoking = 12x risk |
| Treatment | Endoscopic subperiosteal resection + bone drilling at attachment |
| Recurrence | 0-30%; due to residual disease |
| Biopsy | Required for diagnosis (unlike JNA) |
Sources: Cummings Otolaryngology Head and Neck Surgery (pp. 985-991); Robbins, Cotran & Kumar Pathologic Basis of Disease (p. 690); Grainger & Allison's Diagnostic Radiology (p. 1604); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 (pp. 1146-1154)
This is a shared conversation. Sign in to Orris to start your own chat.