Skin changes in varicose veins
Reading File
Finding Sources
Finding Sources
Searching PubMed
"varicose veins" AND "skin changes" AND "chronic venous insufficiency"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive information and clinical images from multiple authoritative textbooks. Here is a thorough, well-organized answer:
Skin Changes in Varicose Veins
Varicose veins cause a progressive spectrum of cutaneous changes driven by chronic venous hypertension. These range from minor cosmetic abnormalities to severe tissue destruction. The underlying mechanism is sustained elevation of venular and capillary pressure, which damages endothelial cells, promotes fluid and protein extravasation, triggers leukocyte activation, and ultimately leads to tissue ischaemia and fibrosis.
Pathophysiological Basis
As venous pressure rises due to valvular incompetence, increased venular and capillary pressure damages cells and allows blood — including red cells and haemoglobin — to leak into the interstitium. The haemoglobin breaks down to haemosiderin, which deposits in the dermis. Inflammatory cell infiltration, smooth muscle cell proliferation, collagen deposition, and increased matrix metalloproteinases further alter the vessel wall and surrounding tissue. The extent and number of incompetent veins governs the severity of soft-tissue complications, though notably neither reflux burden nor the presence of skin changes (short of ulceration) reliably correlates with subjective symptom severity. — Bailey and Love's Short Practice of Surgery, 28th Ed.
Clinical Spectrum of Skin Changes
The changes follow a well-recognised progression (CEAP classes C0–C6):
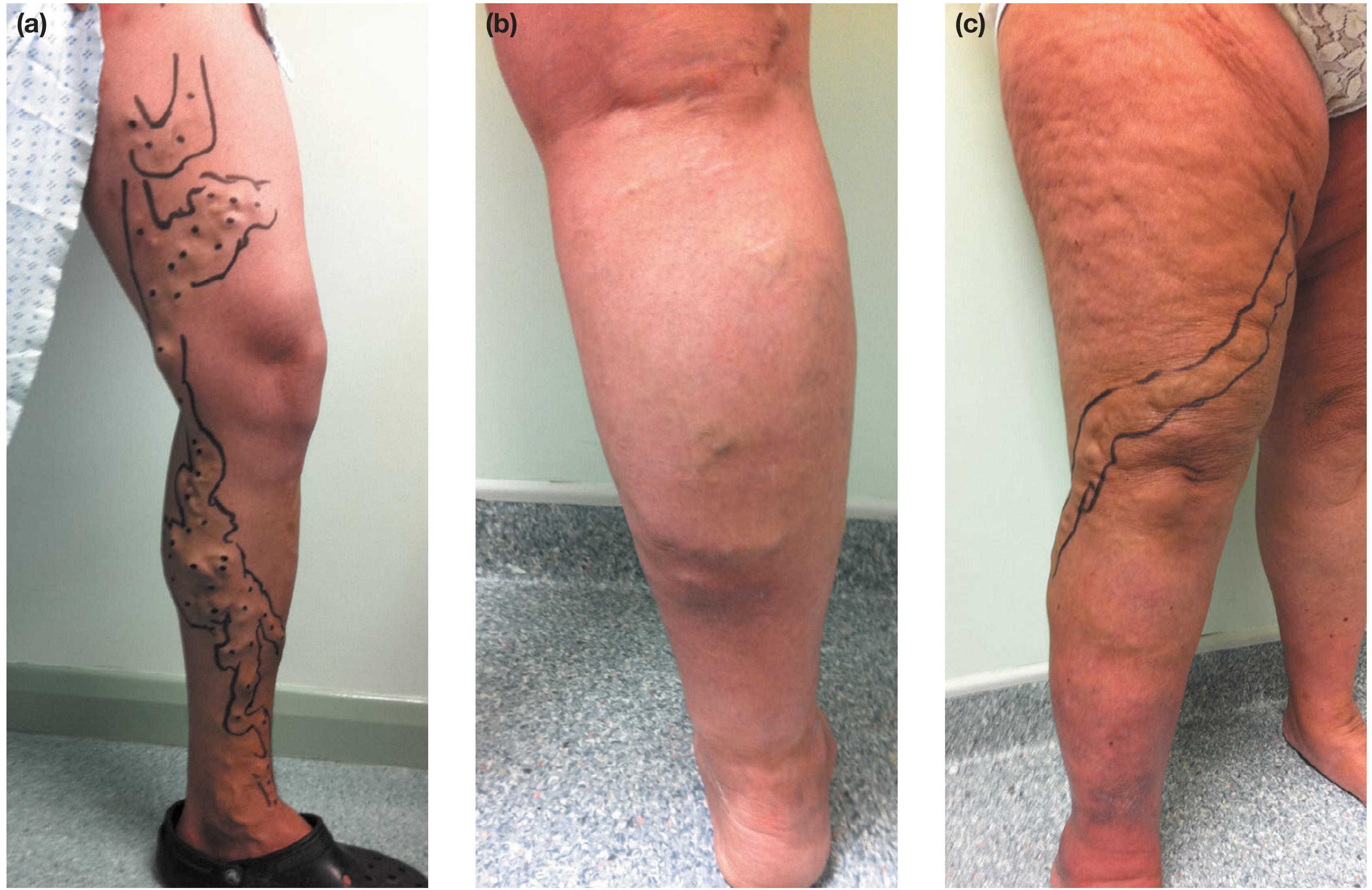
1. Telangiectasias and Reticular Veins (Early / C1–C2)
The earliest visible skin findings:
- Telangiectasias (thread veins, spider veins): tiny intradermal venules <1 mm diameter, appearing as blue, purple, or red linear/branching patterns near the skin surface
- Reticular veins: bluish subdermal dilated veins 1–2.9 mm diameter, often tortuous
- Corona phlebectatica (malleolar flare): a fan-shaped pattern of telangiectasia around the ankle/foot — an early marker of advanced venous disease
2. Oedema (C3)
- Increased volume of fluid in skin and soft tissues, beginning distally and progressing proximally
- Classic pitting oedema: firm digital pressure leaves an indentation
- The earliest finding is perimalleolar oedema ascending the leg; soft tissue tenderness is often elicited even over normal-appearing skin — Fitzpatrick's Dermatology
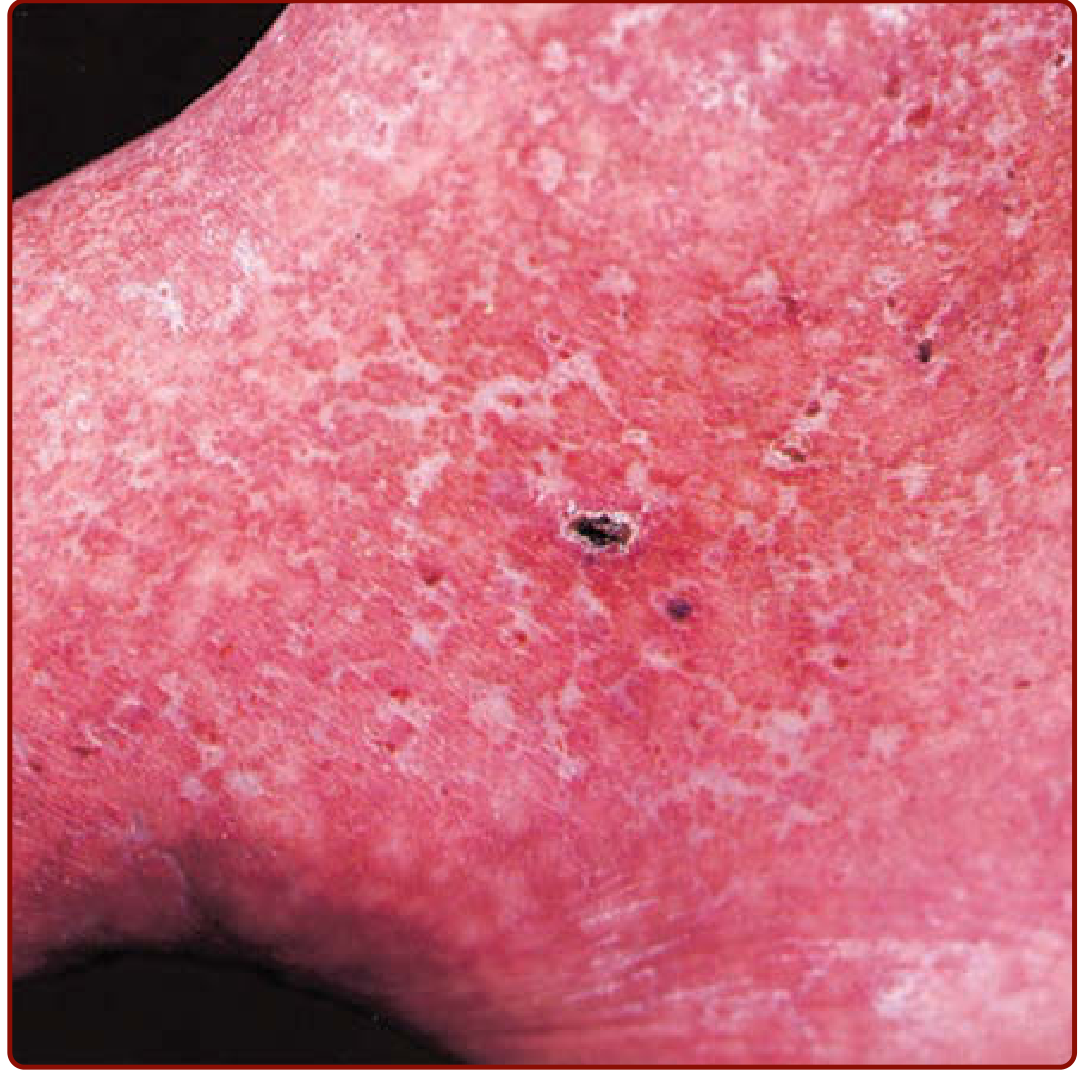
3. Stasis Dermatitis / Venous Eczema (C4a)

- An erythematous dermatitis with scaling, pruritus, erosions, crusting, occasional vesicles and serous drainage
- Typically arises in the medial supramalleolar region where microangiopathy is most intense
- Can occur at any stage of chronic venous insufficiency; over time, lesions may lichenify
- In extreme cases progresses to blistering and weeping
- Up to 80% of patients with venous leg ulcers develop allergic contact dermatitis from topical therapies — coexisting sensitisation must be considered — Fitzpatrick's Dermatology
4. Haemosiderosis / Pigmentation (C4a)

- A brownish discolouration of the skin, usually permanent
- Results from extravasation of red blood cells and subsequent haemoglobin breakdown to haemosiderin in the dermis
- Predominantly periankle but also seen adjacent to varicose veins and incompetent perforators — Bailey and Love's
5. Lipodermatosclerosis (C4b)
- Chronic inflammation and fibrosis of the skin and subcutaneous tissues, producing a tight, contracted, 'woody' leg
- The pliable subcutaneous fat is gradually replaced by fibrosis; the indurated plaque begins at the medial ankle and extends circumferentially around the distal lower leg
- As fibrosis tightens it may strangle the lower leg, causing the classical "inverted champagne bottle" appearance with brawny oedema above and below
- Occasionally presents acutely as bright red erythema and tenderness mimicking cellulitis — distinguished by the absence of systemic signs and failure to respond to antibiotics; septal panniculitis is seen histologically
- Can result in significant Achilles tendon contracture — a sign of severe disease — Fitzpatrick's Dermatology; Bailey and Love's
6. Atrophie Blanche (C4b)
- Localised areas of atrophic, porcelain-white skin, often stellate in shape, surrounded by hyperpigmentation and telangiectasias
- Represents dermal fibrosis secondary to ischaemia; a marker of severe chronic venous disease
- May also occur in hypercoagulable states (antiphospholipid syndrome, inherited coagulopathies), livedoid vasculitis, or autoimmune diseases (scleroderma, SLE) — Fitzpatrick's
7. Venous Ulceration (C5–C6)

- Full-thickness skin loss, usually around the ankle ("gaiter area"), that fails to heal spontaneously
- Propagated by continuing venous hypertension, tissue ischaemia, and the cumulative changes of chronic venous disease
- Can become chronic varicose ulcers due to poor wound healing and superimposed infection
- ~20% of patients with chronic venous insufficiency eventually develop venous ulcers — Robbins; Harrison's
8. Acroangiodermatitis of Mali (Pseudo-Kaposi Sarcoma)
- Purple macules, nodules, or verrucous plaques on the dorsal feet and toes
- Seen in longstanding venous insufficiency; mimics Kaposi sarcoma both clinically and histologically
- Also described in AV malformations, dialysis shunts, paralysed limbs — Fitzpatrick's
CEAP Classification Summary
| Class | Skin Findings |
|---|---|
| C0 | No visible signs |
| C1 | Telangiectasias / reticular veins |
| C2 | Varicose veins |
| C3 | Oedema |
| C4a | Pigmentation, stasis dermatitis |
| C4b | Lipodermatosclerosis, atrophie blanche |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
Key Points
- The skin changes of varicose veins are collectively grouped under chronic venous insufficiency (CVI)
- The medial ankle/gaiter area is the most commonly and severely affected site due to the highest microangiopathic burden
- Stasis dermatitis, haemosiderosis, lipodermatosclerosis, atrophie blanche, and venous ulceration are the major dermatological sequelae
- Skin changes correlate with disease severity and reflux burden, but not necessarily with subjective symptoms
- Graduated compression (30–40 mmHg) is the foundation of management for C3–C6 disease
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed. | Fitzpatrick's Dermatology | Robbins & Kumar Basic Pathology | Harrison's Principles of Internal Medicine, 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.