
ECG interpretation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer. Let me compile the full ECG interpretation and management plan.
ECG Interpretation — Ticket №9
Clinical Context (from the document)
- Patient: 28-year-old male
- Complaint: Episodes of sudden palpitations + dizziness
- Onset/offset: Abrupt start and abrupt stop
- During attack: HR ~170–190 bpm, regular rhythm, BP stable
ECG Analysis
Looking at the 12-lead tracing:
| Feature | Findings |
|---|---|
| Rate | ~170–190 bpm |
| Rhythm | Regular |
| QRS width | Narrow (<120 ms) |
| P waves | Not clearly visible before QRS; buried in or immediately after QRS (retrograde P) |
| Pseudo-r' in V1 | Present (retrograde P superimposed on terminal QRS) |
| Pseudo-S in II, III, aVF | Present (hallmark finding) |
| RP interval | Short (RP < PR) |
| No delta waves | No pre-excitation pattern |
Compare with the classic textbook AVNRT tracing:
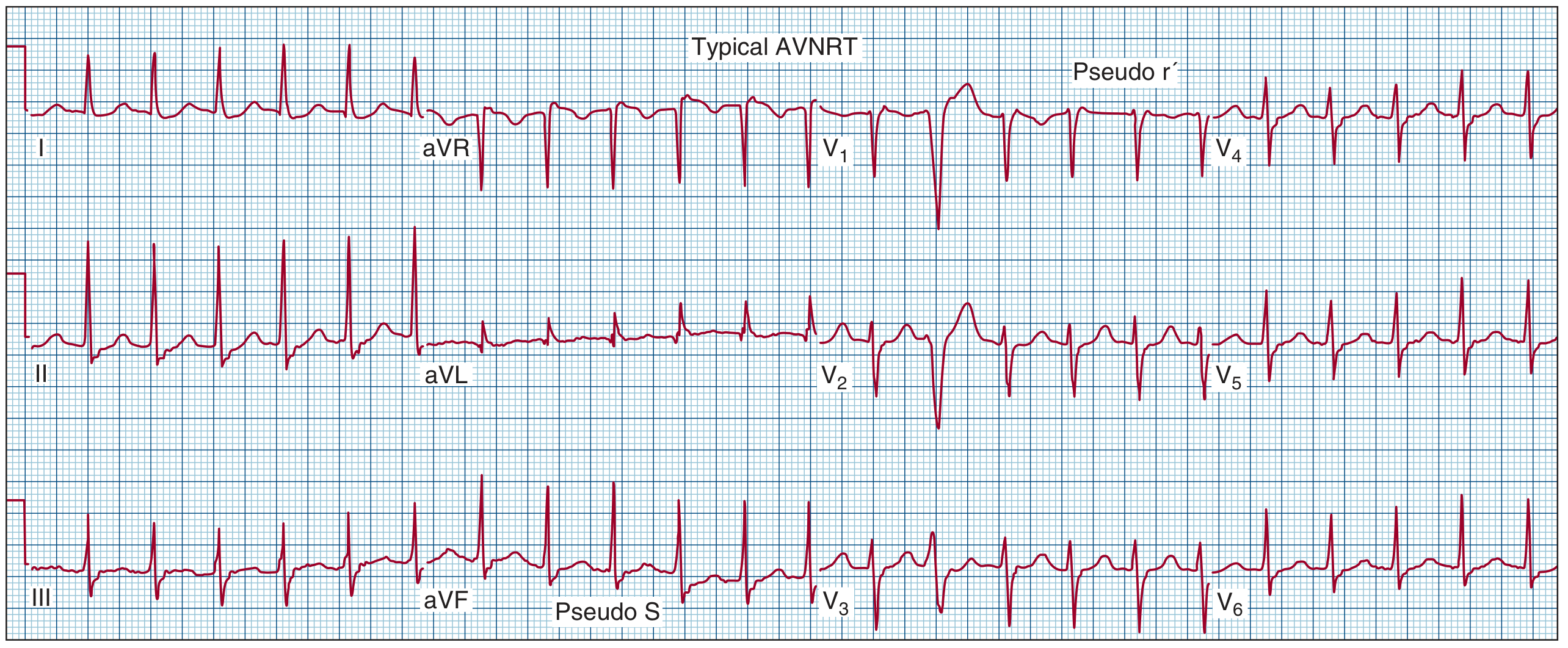
Note the pseudo-r' in V1 and pseudo-S waves in II/III/aVF — identical to the ECG in the exam ticket.
1. Diagnosis
Paroxysmal Supraventricular Tachycardia — Typical (slow/fast) AVNRT
Rationale:
- Narrow QRS tachycardia at ~170–190 bpm with sudden onset and termination (re-entry mechanism)
- Retrograde P waves buried within or at the terminal portion of the QRS → very short VA interval (VA < 70 ms)
- Pseudo-r' in V1 and pseudo-S in inferior leads are the classic hallmarks of typical AVNRT
- No delta wave → excludes WPW/AVRT
- Young patient, structurally normal heart, BP stable
The mechanism is re-entry within the AV node using the slow pathway (anterograde) and fast pathway (retrograde), creating a rapid circus movement entirely within the AV nodal region.
"AVNRT is characterized by a tachycardia with a narrow QRS complex with sudden onset and termination generally at regular rates between 120 bpm and 200 bpm... The presence of a pseudo r' wave in lead V1 or pseudo S wave in leads II, III, and aVF suggests typical AVNRT." — Fuster and Hurst's The Heart, 15th Edition
2. Possible Complications
| Complication | Comment |
|---|---|
| Presyncope / syncope | Due to sudden drop in cardiac output at high rate (already showing dizziness) |
| AF development | Up to 12% of PSVT patients develop atrial fibrillation during follow-up |
| ST-segment depression | Seen in 25–50% during tachycardia — does not indicate ischemia, but requires differentiation |
| Post-tachycardia T-wave inversions | Seen in ~40% after termination; transient, not ischemic |
| Hemodynamic compromise | Rare at this age with normal heart, but possible if prolonged |
| Misdiagnosis as panic/anxiety | Clinically important — delays correct treatment |
3. Treatment Strategy
Acute Episode — Termination
Step 1: Vagal maneuvers (first line)
- Valsalva maneuver (modified: lying flat with legs elevated — most effective)
- Carotid sinus massage (right side first, rule out carotid bruits)
- Cold water immersion (especially in children)
- These increase vagal tone → slows/blocks AV node → breaks re-entry circuit
Step 2: Pharmacologic cardioversion (if vagal fails)
| Drug | Dose | Mechanism |
|---|---|---|
| Adenosine (1st choice) | 6 mg IV rapid bolus → 12 mg if no response | Transient AV block — interrupts re-entry; very short half-life (~10 sec) |
| Verapamil | 5–10 mg IV slowly | Calcium channel blocker — blocks AV node |
| Diltiazem | 0.25 mg/kg IV | Calcium channel blocker |
| Metoprolol | 5 mg IV slowly | Beta-blocker, slows AV node |
Step 3: Synchronized DC cardioversion
- Reserved for hemodynamic instability (rare in this patient given stable BP)
- Energy: 50–100 J biphasic
Long-term / Preventive Management
Option A — Pharmacological prophylaxis (for frequent symptomatic episodes)
- Beta-blockers (metoprolol, bisoprolol)
- Non-dihydropyridine CCBs (verapamil, diltiazem)
- Flecainide or propafenone (in patients without structural heart disease)
Option B — Catheter ablation (preferred definitive treatment)
- Radiofrequency ablation of the slow pathway — success rate >95%, recurrence <5%
- Indicated in: frequent episodes, drug-refractory AVNRT, patient preference
- Complication: AV block risk ~1% (requires permanent pacemaker in rare cases)
- For a 28-year-old with recurrent symptomatic episodes, ablation is the treatment of choice
Summary Answer for the Exam
- Diagnosis: Paroxysmal SVT — typical AVNRT (slow/fast), re-entry mechanism within the AV node
- Complications: Presyncope/syncope, AF development (12%), ST-depression during episode (not ischemic), hemodynamic deterioration if prolonged
- Treatment:
- Acute: Valsalva → IV Adenosine → IV Verapamil → synchronized cardioversion (if unstable)
- Long-term: Catheter radiofrequency ablation of slow AV nodal pathway (definitive, >95% cure rate) or beta-blocker/CCB prophylaxis
Sources: Fuster and Hurst's The Heart, 15th Ed.; Braunwald's Heart Disease, 12th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.