Types of seizures
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative neurology textbooks. Let me compile the full answer.
Types of Seizures
Seizures represent abnormal, highly synchronous neuronal activity. The current standard framework is the ILAE 2017 Operational Classification, which organizes seizures by their onset into three categories: focal, generalized, and unknown.
ILAE 2017 Classification at a Glance
Source: Katzung's Basic and Clinical Pharmacology, 16th Ed.
| Category | Subtypes |
|---|---|
| Focal Onset | Focal aware; Focal impaired awareness; Focal-to-bilateral tonic-clonic |
| Generalized Onset | Tonic-clonic; Absence (typical/atypical); Myoclonic; Atonic; Tonic; Clonic; Epileptic spasms |
| Unknown Onset | Tonic-clonic; Epileptic spasms; Behavior arrest |
1. Focal Onset Seizures (formerly "Partial")
Originate in a localized group of neurons in one hemisphere. Commonly caused by head injury, stroke, tumor, or brain infection - though often the cause is unknown. Symptoms depend entirely on the region involved.
a) Focal Aware Seizure (formerly Simple Partial)
- Consciousness is fully preserved
- Symptoms reflect the focal cortical region: localized jerking (motor cortex), sensory disturbance, autonomic changes, or psychic phenomena
- An aura is itself a focal aware seizure and represents the initial phase of a larger seizure
- Example: rhythmic jerking of one hand progressing to the entire arm (Jacksonian march), lasting 60-90 seconds
b) Focal Impaired Awareness Seizure (formerly Complex Partial)
- Consciousness or awareness is impaired
- Often begins with a motionless stare, followed by automatisms (lip smacking, chewing, picking movements, fumbling)
- Most commonly arise from the temporal lobe
- Followed by a postictal period of confusion
c) Focal-to-Bilateral Tonic-Clonic (formerly Secondarily Generalized)
- Begins focally, then spreads to involve both hemispheres
- Implies an underlying focal brain lesion
- The initial focal phase may be brief and unwitnessed
Key point: Focal seizures can be convulsive or nonconvulsive, and can secondarily generalize into any generalized type. - Adams and Victor's Principles of Neurology, 12th Ed.
2. Generalized Onset Seizures
Involve both hemispheres simultaneously from the outset, with widespread electrical activity bilaterally.
a) Generalized Tonic-Clonic (GTC) - formerly Grand Mal
The most common convulsive type. Typically no warning (or brief prodrome):
- Tonic phase (10-20 s): Sudden loss of consciousness + fall, body rigidity, jaw clamping (tongue bite risk), apnea, cyanosis, dilated unreactive pupils, bladder emptying possible
- Clonic phase (1-2 min): Rhythmic jerking of limbs at ~4-8/second, prominent autonomic signs (tachycardia, hypertension, hypersalivation)
- Postictal phase: Deep coma transitioning to confusion, lethargy, headache; lasts minutes to hours
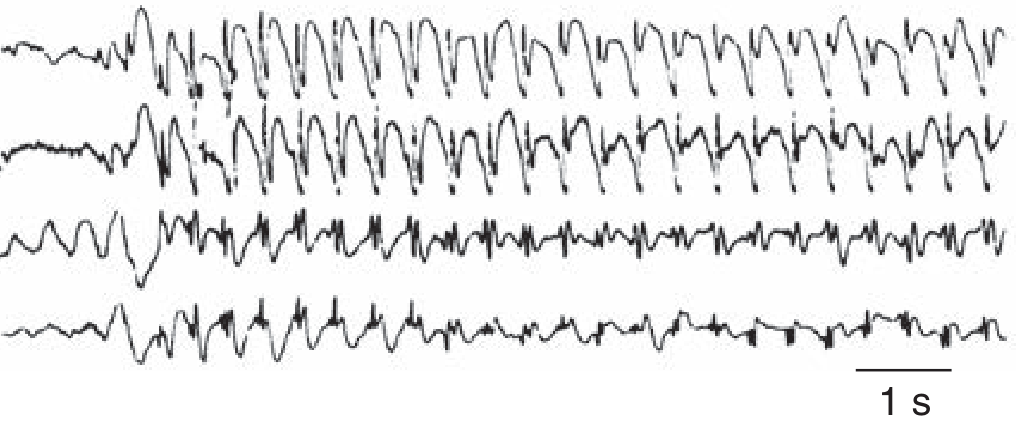
- EEG: fast activity during tonic phase; spike-slow wave complexes during clonic jerks
b) Absence Seizure - formerly Petit Mal
- Momentary (5-20 s) lapse of consciousness with sudden onset and offset
- Patient freezes mid-activity; eyelid flickering may occur; no falling
- No aura, no postictal period - distinguishes it from focal impaired awareness seizures
- EEG hallmark: 3 Hz spike-and-wave complexes (generated by T-type Ca²+ channels in thalamic neurons)
- Predominantly in children; multiple episodes per day possible
Atypical absence seizures have a slower onset/offset, more pronounced motor features, and irregular 1.5-2.5 Hz spike-waves; associated with Lennox-Gastaut syndrome.
c) Myoclonic Seizures
- Sudden, brief, bilateral muscle jerks without loss of consciousness (or very brief impairment)
- Typically occur on awakening; can be triggered by sleep deprivation or photic stimulation
- Seen in juvenile myoclonic epilepsy (JME) and Dravet syndrome
- EEG: polyspike-and-wave discharges
d) Atonic Seizures (Drop Attacks)
- Sudden loss of postural muscle tone causing the patient to fall
- Very brief (1-2 s); risk of injury from falls
- Also called drop seizures or akinetic seizures
- Associated with Lennox-Gastaut syndrome
- EEG: slow spike-wave or flattening
e) Tonic Seizures
- Sudden sustained muscle stiffening/rigidity without a clonic phase
- Often nocturnal; common in Lennox-Gastaut syndrome
- Brief (seconds); postictal confusion is minimal
f) Clonic Seizures
- Rhythmic jerking movements without a preceding tonic phase
- Rarer than tonic-clonic; more common in neonates and young children
g) Epileptic Spasms (Infantile Spasms)
- Brief flexion/extension of trunk and limbs in clusters, typically on waking
- Onset in infancy (3-12 months); signature of West syndrome
- EEG: hypsarrhythmia (chaotic, high-voltage, disorganized pattern)
3. Unknown Onset
Used when onset is unwitnessed or unclear. Includes tonic-clonic, epileptic spasms, and behavior arrest. Reclassified once more information becomes available.
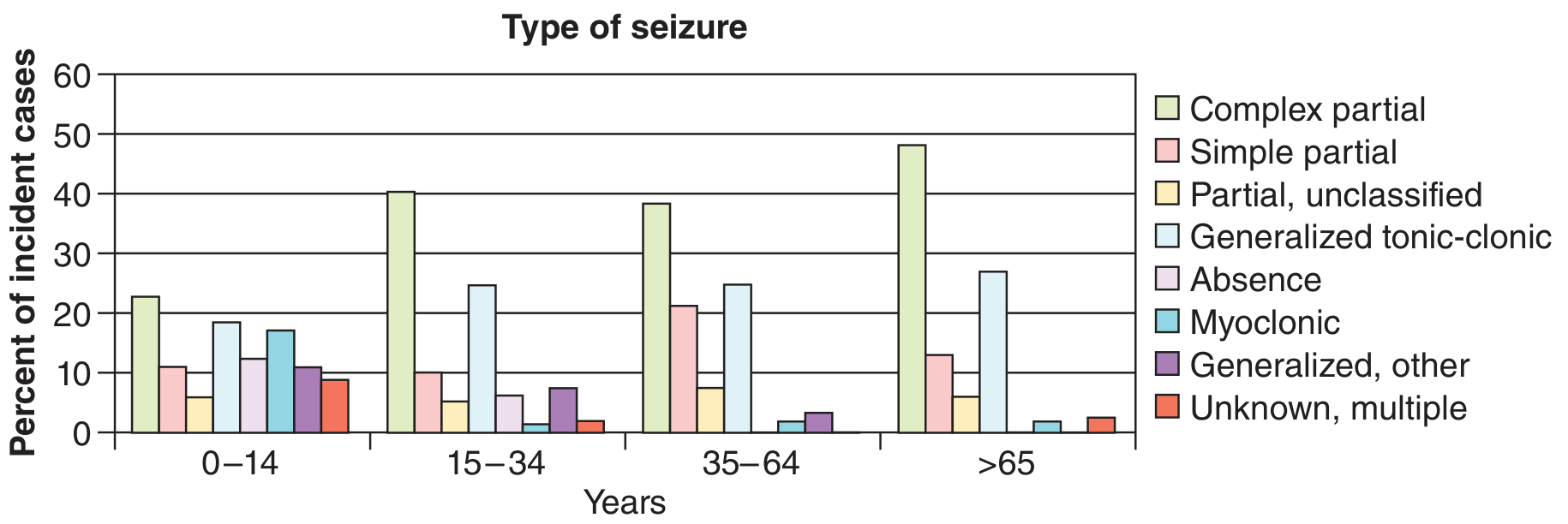
Age Distribution of Seizure Types
Quick Comparison: Key Differentiators
| Feature | Focal Aware | Focal Impaired Awareness | Absence | GTC |
|---|---|---|---|---|
| Consciousness | Intact | Impaired | Lost briefly | Lost |
| Aura | Often present | Often present | None | Rarely |
| Postictal | None/brief | Yes (confusion) | None | Yes (prolonged) |
| Duration | Seconds-minutes | 1-3 min | 5-20 s | 1-3 min |
| Automatisms | Possible | Common | Rare | No |
| EEG | Focal discharge | Focal discharge | 3 Hz spike-wave | Fast then spike-wave |
Terminology Update (Old vs. New)
| Old Term | New ILAE 2017 Term |
|---|---|
| Simple partial | Focal aware |
| Complex partial | Focal impaired awareness |
| Secondarily generalized | Focal-to-bilateral tonic-clonic |
| Grand mal | Generalized tonic-clonic |
| Petit mal | Generalized absence |
Sources: Adams and Victor's Principles of Neurology (12th Ed.), Katzung's Basic and Clinical Pharmacology (16th Ed.), Ganong's Review of Medical Physiology (26th Ed.), Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.