
asnwer as per muhs exam systematically 2mbbs micro refer apurba shastri answer in detail and add colour diagrams easy to draw in exams as required as well cover details of answers
MUHS 2nd MBBS - MICROBIOLOGY - PAPER 1
LAQ SECTION
Q1. 5-year-old female: abdominal pain, weight loss, perianal itching
i) Likely Parasite (2 marks)
- Age: 5 years (children most affected)
- Perianal itching (pathognomonic) - especially at night
- Abdominal pain + weight loss
- Phylum: Nemathelmintha
- Class: Nematoda
- Habitat: Caecum, appendix, large intestine
ii) Life Cycle (3 marks)
┌──────────────────────────────────────────────────────────┐
│ LIFE CYCLE OF E. VERMICULARIS │
│ │
│ INFECTIVE EGGS (ingested) │
│ ↓ (Mouth → stomach → small intestine) │
│ LARVAE HATCH in duodenum │
│ ↓ migrate to large intestine │
│ ADULT WORMS develop in caecum/colon │
│ (Male + Female mate in large intestine) │
│ ↓ │
│ Gravid FEMALE migrates to perianal region at night │
│ ↓ lays 10,000-15,000 eggs │
│ EGGS deposited on perianal skin │
│ → become infective within 6 hours │
│ ↓ (Scratching → hand → mouth) │
│ RE-INGESTION / AUTO-INFECTION │
│ ↓ │
│ Retrograde infection also possible (rare) │
└──────────────────────────────────────────────────────────┘
- No intermediate host
- Infective form: embryonated egg (with larvae inside)
- Mode of infection: Feco-oral, hand-to-mouth (auto-infection)
- Time from egg ingestion to adult maturity: 2-4 weeks
- Retroinfection: eggs hatch on perianal skin, larvae re-enter via anus
- Ectopic sites: vagina, uterus, fallopian tubes, peritoneum (in girls)
iii) Labelled Diagram of Parasite and Egg (3 marks)
╔══════════════════════════════════════════════════════╗
║ ENTEROBIUS VERMICULARIS - ADULT WORMS ║
║ ║
║ FEMALE (10 mm): MALE (3-5 mm): ║
║ ┌──────────────┐ ┌──────────┐ ║
║ │ Cervical │ │ │ ║
║ │ alae (wing- │◄HEAD │ HEAD │ ║
║ │ like) │ │ ↓ │ ║
║ │ Esophagus │ │ CURVED │ ║
║ │ with bulb►───┤ │POSTERIOR │ ║
║ │ │ │ end │ ║
║ │ Long pointed │ │(single │ ║
║ │ POSTERIOR ──►│ │spicule) │ ║
║ │ end │ └──────────┘ ║
║ └──────────────┘ ║
║ ║
║ KEY: Cervical alae = cephalic alae (both sexes) ║
║ Female has POINTED TAIL (pin-shaped) ║
║ Male has CURVED TAIL ║
╚══════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════════════╗
║ ENTEROBIUS EGG - EASY TO DRAW ║
║ ║
║ ╔══════════════════╗ ← Thick shell ║
║ ║ ___________ ║ ║
║ ║ / EMBRYO \ ║ ← Larva visible inside ║
║ ║| (coiled | ║ ║
║ ║ \ larva) / ║ ║
║ ║ ----------- ║ ║
║ ╚══════════════════╝ ║
║ ║
║ Shape: PLANO-CONVEX (asymmetrical) ║
║ = D-shaped / football-shaped ║
║ Size: 50-60 x 20-30 μm ║
║ ONE side FLAT, OTHER side CONVEX ║
║ DOUBLE-WALLED shell ║
║ Contains coiled larva (infective stage) ║
╚══════════════════════════════════════════════════════╝
Exam tip: The FLAT-CONVEX shape of the egg is PATHOGNOMONIC - no other helminth has this egg shape.
iv) Lab Diagnosis
- Preferred method
- Transparent sticky tape applied to perianal skin early morning BEFORE bathing or defecation
- Tape placed on glass slide, examined under microscope
- Reveals characteristic plano-convex eggs
- Repeat on 3 consecutive mornings to improve sensitivity
- Wooden spatula with cellophane tape used to swab perianal area
- Examined microscopically
- Routine stool O&P: adult worms may be seen (less sensitive for eggs)
- Eggs rarely found in stool (laid outside in perianal region)
- Thread swallowed, retrived, examined for adherent eggs
Q2. 6 children, 9-10 years, rice-watery diarrhea, vomiting, no pus cells, darting motility
i) Probable Organism
| Feature | Significance |
|---|---|
| Rice-water stools | "Baryta water" appearance - characteristic |
| No pus cells | Non-inflammatory, toxin-mediated |
| Vomiting | Acute onset |
| Darting motility | "Shooting star" motility of Vibrio |
| Cluster (ashram) | Point source outbreak from contaminated water/food |
ii) Etiological Agent
| Property | Details |
|---|---|
| Morphology | Comma-shaped (curved) gram-negative rod |
| Motility | Single polar flagellum - darting/shooting star motility |
| Size | 1.5-3.0 x 0.2-0.4 μm |
| Arrangement | S-shape / school of fish in smear |
| Gram stain | Gram-negative bacilli |
| Capsule | Absent |
| Spores | Absent |
- Alkaliphilic - grows best at pH 8.5-9.5
- TCBS agar (Thiosulfate Citrate Bile Salts Sucrose) - yellow colonies (sucrose fermenter)
- Peptone water - forms surface pellicle
- Blood agar - beta-hemolysis (El Tor biotype)
- Non-halophilic (unlike other Vibrios)
- Classical biotype (original)
- El Tor biotype (currently predominant, 7th pandemic)
- Cholera toxin (CT) - A-B type exotoxin (most important)
- B subunit (5 subunits): binding to GM1 ganglioside on enterocytes
- A subunit: activates adenylyl cyclase → ↑↑ cAMP → massive Cl⁻ secretion + inhibits Na⁺ absorption → massive water loss
- Toxin co-regulated pilus (TCP) - colonization factor
- Neuraminidase - converts GM2 → GM1 (more receptor exposure)
iii) Lab Diagnosis
- Wet mount: Comma-shaped, highly motile organisms - darting motility
- "Hanging drop" preparation shows typical darting/shooting star motility
- Immobilization test: Motility inhibited by O1 antiserum (diagnostic)
- Alkaline peptone water (APW) pH 8.6 - enrichment broth (incubate 4-6 hrs)
- TCBS agar - yellow colonies of V. cholerae O1
- Gelatin stab: Infundibuliform (funnel-shaped) liquefaction
- Blood agar: Beta-hemolysis (El Tor), non-hemolysis (Classical)
- Oxidase positive (key feature - unlike Enterobacteriaceae)
- Indole positive
- String test positive (0.5% sodium deoxycholate → viscous string)
- Voges-Proskauer: El Tor +ve, Classical -ve
- Chicken cell agglutination: El Tor +ve
- Slide agglutination with O1 polyvalent antiserum
- Differentiate Ogawa (A+B) vs Inaba (A+C)
- Dipstick/lateral flow immunoassay (Crystal VC, SD Bioline) - for field use
- Multiplex PCR
- Identifies organism directly in stool
iv) Management
SEVERITY ASSESSMENT:
↓
Mild/No dehydration → ORS (oral rehydration solution)
↓
Moderate dehydration → ORS aggressively
↓
Severe dehydration → IV Ringer's Lactate (100ml/kg)
WHO regimen: 30ml/kg in 30 min, then 70ml/kg in 2.5 hrs
- WHO ORS: NaCl 3.5g + KCl 1.5g + NaHCO3 2.5g + Glucose 20g in 1 liter water
- Rice-based ORS is superior
- Adults: Doxycycline 300mg single dose (drug of choice)
- Children: Azithromycin 20mg/kg single dose
- Alternatives: Cotrimoxazole, Ciprofloxacin
- 20mg/day for 10-14 days
- Identify source (water/food)
- Notify public health authorities
- Quarantine contacts
- Safe water supply, proper sanitation
- Boil water advisory
- Dukoral (oral killed whole cell + CTB) - 2 doses
- Shanchol (bivalent oral inactivated) - 2 doses
Q3. RT hypochondrial tenderness, fever, WBC 16,000, SGPT 247, SGOT 285, USG: single abscess postero-superior liver
i) Probable Pathogen
| Feature | Amoebic | Pyogenic |
|---|---|---|
| Age/sex | Young adult male | Any age |
| Abscesses | Usually SINGLE | Often multiple |
| Location | Right lobe, postero-superior | Anywhere |
| Pus | Anchovy sauce/chocolate | Yellow/green |
| Travel history | Tropical | Often biliary disease |
| Serology | Positive | Negative |
ii) Lab Diagnosis
- ELISA for anti-amoeba antibodies - sensitivity ~95%
- IHA (Indirect Hemagglutination Assay) - titre >1:256 significant
- Counter Immunoelectrophoresis (CIE)
- Latex agglutination test
- Wet preparation: look for motile trophozoites with ingested RBCs
- Stool microscopy positive in only 30-40% of ALA cases
- Cysts in formed stool
TROPHOZOITE features (diagnostic):
- Size: 12-60 μm
- Motility: Directional (unidirectional), progressive with finger-like pseudopodia
- INGESTED RBCs in cytoplasm (pathognomonic)
- Ectoplasm (clear) and endoplasm (granular) visible
- Pus: Anchovy sauce appearance (brownish, thick)
- Trophozoites found at PERIPHERY of abscess (not in pus)
- Gram stain: No organisms usually (sterile unless secondary bacterial infection)
- Send for: wet mount, ZN stain, C&S (to rule out pyogenic)
- Leukocytosis (WBC 16,000 as in this case) - polymorphonuclear predominance
- SGPT/SGOT elevated (hepatocellular damage)
- ALP markedly elevated
- Blood culture negative (unlike pyogenic)
- USG: single well-defined hypoechoic lesion, right lobe, postero-superior = classic ALA
- CT scan: low-density lesion with peripheral enhancement
- MRI: T2 hyperintense lesion
- Stool antigen ELISA (TechLab E. histolytica II test) - detects Gal/GalNAc lectin
iii) Life Cycle (3 marks)
╔═══════════════════════════════════════════════════════════════╗
║ LIFE CYCLE OF ENTAMOEBA HISTOLYTICA ║
║ ║
║ MATURE QUADRINUCLEATE CYST (infective form) ║
║ ↓ [Ingested via contaminated food/water] ║
║ STOMACH → resistant to gastric acid ║
║ ↓ ║
║ SMALL INTESTINE → EXCYSTATION ║
║ ↓ [metacystic trophozoite forms] ║
║ METACYSTIC TROPHOZOITE (8 nucleate → 8 trophozoites) ║
║ ↓ ║
║ LARGE INTESTINE (cecum, ascending colon) ║
║ ↓ ║
║ ├── COMMENSALISM: ║
║ │ lives on luminal surface → CYSTS formed ║
║ │ → passed in stool → continue cycle ║
║ │ ║
║ └── INVASION (pathogenic route): ║
║ ↓ [penetrate mucosa via cytotoxin + proteases] ║
║ FLASK-SHAPED ULCER in colon ║
║ ↓ ║
║ ├── AMOEBIC DYSENTERY (intestinal) ║
║ │ ║
║ └── BLOOD VESSEL INVASION ║
║ ↓ [portal vein] ║
║ LIVER → AMOEBIC LIVER ABSCESS ║
║ ↓ [transdiaphragmatic spread] ║
║ LUNG, BRAIN, SKIN (rare) ║
║ ║
║ CYST FORMS: 1-nucleate → 2-nucleate → 4-nucleate (mature) ║
╚═══════════════════════════════════════════════════════════════╝
- Size: 10-20 μm
- Shape: Spherical
- Nuclei: 1 to 4 (mature cyst = 4 nuclei)
- Chromatoidal bars: rounded/cigar-shaped ends (vs. E. coli: splinted ends)
- Glycogen mass: present in young cysts (stains brown with Lugol's iodine)
- Metronidazole 800mg TID x 10 days (drug of choice for invasive disease)
- Tinidazole 2g OD x 3 days
- Followed by luminal agent: Diloxanide furoate 500mg TID x 10 days (to eliminate intestinal cysts)
- Drain abscess if: >5cm, risk of rupture, failed medical therapy
SAQ SECTION
SAQ 1: Bacterial Growth Curve and Applications
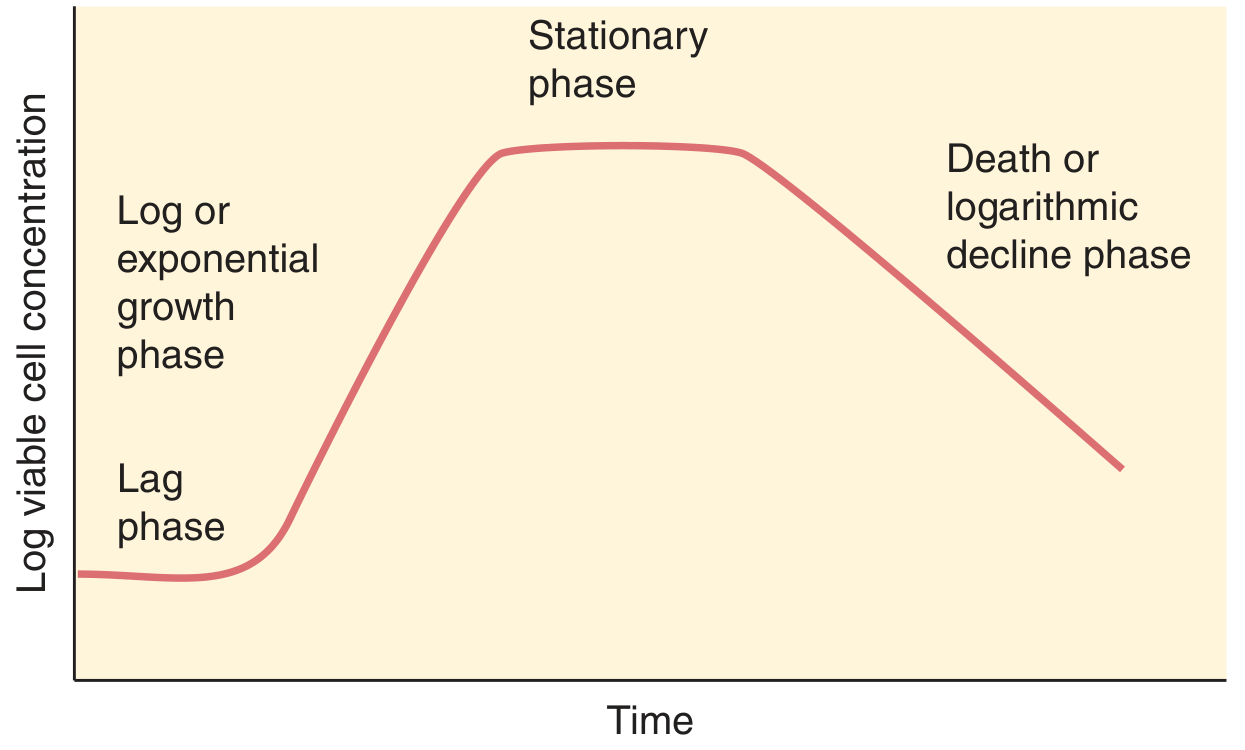
Four Phases:
╔══════════════════════════════════════════════════════════════════╗
║ BACTERIAL GROWTH CURVE ║
║ ║
║ Log │ ___________ ║
║ viable │ / \ STATIONARY ║
║ cell │ / \────────────────DEATH ║
║ count │ / (plateau) \ ║
║ │ ____/ EXPONENTIAL \ ║
║ │ LAG (log) ↘ ║
║ └────────────────────────────────────────── ║
║ TIME → ║
╚══════════════════════════════════════════════════════════════════╝
| Phase | Growth Rate | Events |
|---|---|---|
| 1. Lag phase | Zero (no division) | Adaptation: enzymes, co-factors being synthesized; metabolic activity high but no cell division |
| 2. Log/Exponential phase | Maximum (constant) | Rapid binary fission; doubling time constant; metabolically most active; most sensitive to antibiotics |
| 3. Stationary phase | Zero (birth = death) | Nutrient depletion; toxic metabolite accumulation; spore formation; some cell lysis balanced by new growth |
| 4. Death/Decline phase | Negative | Death exceeds growth; VBNC (viable but non-culturable) cells may persist |
Applications of Growth Curve:
- Antibiotic therapy: Log phase bacteria most susceptible to cell-wall synthesis inhibitors (penicillin, cephalosporins)
- Vaccine production: Organisms harvested at log phase (maximum viable count, maximum antigenicity)
- Industrial fermentation: Antibiotics, enzymes harvested in appropriate phases
- Sterilization protocols: Understanding death kinetics helps calculate D-value and sterilization time
- Epidemiology: Incubation period of diseases correlates with growth phase
- Culture media optimization: Determining generation time of organisms
- Antimicrobial susceptibility testing (MIC, MBC): Inoculum standardized to log phase
- E. coli: 20 min
- S. aureus: 30 min
- M. tuberculosis: 18-24 hours (explains slow disease progression)
SAQ 2: Methods of Horizontal Gene Transfer (HGT) - describe one in detail
Three Main Methods:
╔══════════════════════════════════════════════════════════════╗
║ HORIZONTAL GENE TRANSFER - OVERVIEW ║
║ ║
║ 1. TRANSFORMATION 2. TRANSDUCTION ║
║ ┌──────────────┐ ┌──────────────────────┐ ║
║ │ Donor cell │ │ Bacteriophage picks │ ║
║ │ lyses → │ │ up donor DNA → │ ║
║ │ naked DNA │ │ injects into │ ║
║ │ released → │ │ recipient cell │ ║
║ │ recipient │ └──────────────────────┘ ║
║ │ takes up DNA │ ║
║ └──────────────┘ ║
║ ║
║ 3. CONJUGATION (Cell-to-cell contact) ║
║ ┌──────────┐ ┌──────────┐ ║
║ │ DONOR │──sex pilus────►│ RECIPIENT│ ║
║ │ (F+/Hfr) │ ←conjugation │ (F-) │ ║
║ │ │ bridge │ │ ║
║ └──────────┘ └──────────┘ ║
╚══════════════════════════════════════════════════════════════╝
| Method | Mediator | Requires Cell Contact | DNA type transferred |
|---|---|---|---|
| Transformation | None (naked DNA) | No | Chromosomal/plasmid |
| Transduction | Bacteriophage | No | Any (phage-packaged) |
| Conjugation | Sex pilus | YES | Plasmid (F, R, Col plasmids) |
CONJUGATION - IN DETAIL (most important clinically):
- Donor cell: must carry F (fertility) plasmid (F+ cell) or Hfr (High frequency recombination)
- Recipient: F- cell
- Physical contact through sex pilus (conjugation tube/bridge)
Step 1: F+ donor cell extends sex pilus (F pilus) toward F- recipient
Step 2: Pilus contracts → cells drawn together → conjugation junction formed
Step 3: One strand of F plasmid DNA is nicked at oriT (origin of transfer)
Step 4: Single strand transferred 5'→3' through conjugation bridge
Step 5: Complementary strands synthesized in BOTH cells
Step 6: Recipient becomes F+ (now can transfer to others)
- R plasmids (Resistance plasmids): carry multiple antibiotic resistance genes
- Single conjugation event → multi-drug resistance spread to entire bacterial population
- Example: MRSA resistance, ESBL-producing E. coli
- Responsible for epidemic antibiotic resistance spread in hospital settings
SAQ 3: Blood Spill Management
Immediate Steps:
BLOOD SPILL ON SKIN:
1. Do NOT panic
2. Wash with soap and water for 10-15 minutes
3. Do NOT scrub/squeeze the wound
4. Do NOT use harsh antiseptics (bleach)
5. If mucous membrane (eye/mouth): flush with copious water/saline
6. Report to infection control officer IMMEDIATELY
Steps for Blood Spill on Environmental Surface:
STEP 1: PERSONAL PROTECTION
→ Wear gloves, mask, gown, eye protection
STEP 2: DECONTAMINATION
→ Cover spill with paper towels/cloth
→ Pour 1% Sodium Hypochlorite (bleach) solution over it
→ Leave for 30 minutes (contact time)
→ Clean up with fresh paper towels (outward-inward circular motion)
→ Discard in biohazard bag (yellow bag)
STEP 3: SECOND CLEAN
→ Mop area with detergent/water
STEP 4: WASTE DISPOSAL
→ All material in biohazard bag
→ Dispose as biomedical waste
STEP 5: HAND HYGIENE
→ Remove gloves carefully (glove-in-glove technique)
→ Wash hands with soap and water 6-step WHO method
- Routine decontamination: 0.5% (5000 ppm) hypochlorite
- Large spills: 1% (10,000 ppm) hypochlorite
- Contact time: Minimum 30 minutes
SAQ 4: Steps in NSI (Needle Stick Injury)
- HIV: 0.3% per exposure
- HBV: 6-30% per exposure (highest risk)
- HCV: 0.5-1.8% per exposure
IMMEDIATE STEPS (within seconds-minutes):
┌─────────────────────────────────────────────────┐
│ STEP 1: FIRST AID (IMMEDIATE) │
│ • Do NOT squeeze/suck the wound │
│ • Allow blood to flow freely (encourage) │
│ • Wash with soap and water for 10-15 min │
│ • Apply antiseptic (povidone-iodine/70% alcohol)│
│ • If eyes/mouth: flush with water/saline │
│ │
│ STEP 2: REPORT (within 1-2 hours) │
│ • Report to infection control officer │
│ • Fill NSI reporting form │
│ │
│ STEP 3: ASSESS SOURCE PATIENT │
│ • HIV status (with consent) │
│ • HBsAg, Anti-HCV │
│ • Note: Do NOT delay PEP waiting for results │
│ │
│ STEP 4: BASELINE TESTING OF INJURED HCW │
│ • HIV serology (at 0, 6 weeks, 12 weeks, │
│ 6 months) │
│ • Anti-HBs titre │
│ • Anti-HCV │
│ │
│ STEP 5: POST-EXPOSURE PROPHYLAXIS (PEP) │
│ HIV PEP (start within 2 hours, max 72 hrs): │
│ → TDF + FTC + LPV/r (or RAL) x 28 days │
│ │
│ HBV PEP: │
│ → If vaccinated + immune: No action │
│ → If not vaccinated: HBIG 0.06ml/kg IM + │
│ Hepatitis B vaccine series │
│ → If vaccinated, no response: HBIG x 2 doses │
│ │
│ HCV PEP: No effective PEP available │
│ → Monitor HCV RNA at 4-6 weeks │
│ │
│ STEP 6: FOLLOW UP │
│ • Counselling │
│ • Repeat serology as per schedule │
│ • Report final outcome │
└─────────────────────────────────────────────────┘
- Type of injury (deep vs. superficial)
- Type of device (hollow-bore needle = highest risk)
- Volume of blood inoculated
- Source patient viral load
- Immunization status of HCW
SAQ 5: Note on Autoimmunity
Normal Self-Tolerance Mechanisms:
- Central tolerance: Clonal deletion of self-reactive T cells in thymus (negative selection), B cells in bone marrow
- Peripheral tolerance: Clonal anergy (no co-stimulation), Regulatory T cells (Tregs), immune ignorance
Mechanisms of Autoimmunity (how tolerance breaks down):
╔══════════════════════════════════════════════════════════════╗
║ MECHANISMS OF AUTOIMMUNITY ║
║ ║
║ 1. MOLECULAR MIMICRY ║
║ Microbial antigen → similar to self-antigen ║
║ Ex: Streptococcal M protein → cardiac myosin ║
║ (Rheumatic fever) ║
║ ║
║ 2. POLYCLONAL ACTIVATION ║
║ EBV, superantigens → non-specific activation ║
║ of self-reactive B/T cells ║
║ ║
║ 3. BYSTANDER ACTIVATION ║
║ Inflammation → release of sequestered antigens ║
║ → activated APCs present self-antigens ║
║ ║
║ 4. EPITOPE SPREADING ║
║ Initial immune response → damage → ║
║ exposes new self-epitopes → expanded response ║
║ ║
║ 5. REGULATORY T CELL DEFICIENCY ║
║ Loss of Tregs → unchecked self-reactive clones ║
║ ║
║ 6. SEQUESTERED ANTIGEN RELEASE ║
║ Eye lens, sperm, brain antigens normally hidden ║
║ → trauma exposes them → immune attack ║
║ Ex: Sympathetic ophthalmia, orchitis ║
╚══════════════════════════════════════════════════════════════╝
Classification of Autoimmune Diseases:
| Type | Mechanism | Examples |
|---|---|---|
| Organ-specific | Ab or T cells against specific organ | Hashimoto's thyroiditis, T1DM, Myasthenia gravis, MS |
| Non-organ-specific (systemic) | Ab against ubiquitous antigens | SLE (anti-dsDNA), RA (anti-CCP/RF), Sjogren's (anti-Ro/La) |
Examples of Autoantibodies (High yield):
- SLE: Anti-dsDNA, Anti-Sm (specific), ANA
- RA: Rheumatoid Factor (IgM anti-IgG), Anti-CCP
- Myasthenia gravis: Anti-AChR antibodies
- Pemphigus vulgaris: Anti-desmoglein antibodies
- Graves' disease: TSI (thyroid stimulating immunoglobulin)
- Hashimoto's: Anti-TPO, Anti-thyroglobulin
Role of HLA in Autoimmunity:
- HLA-DR3/DR4 → Type 1 DM
- HLA-B27 → Ankylosing spondylitis
- HLA-DR4 → Rheumatoid arthritis
- HLA-DQ2/DQ8 → Celiac disease
Factors predisposing to Autoimmunity:
- Genetic: HLA haplotype, family history
- Gender: More common in females (sex hormones)
- Environmental: Infections (molecular mimicry), drugs (drug-induced lupus), UV radiation
- Age: Varies with disease
Source references: Jawetz, Melnick & Adelberg's Medical Microbiology 28th Edition; Murray's Medical Microbiology 9th Edition; Apurba Shastri's framework for MUHS examination pattern.
MUHS Exam tip: For LAQs, always begin with "Definition/Classification," then proceed to morphology/life cycle/lab diagnosis/treatment. For SAQs, use clear headings, tables, and diagrams. Time management: LAQ ~15 min each, SAQ ~7-8 min each.
answer
6define prescription Note on mention application with examples 7 Rickertrial infecrow 8]Immunopathogenesis lab d of RHD 9]Laboratory diagnosis of leptospirosis 10] NACO strategies for HIV 11]HIV lab diagnosis 12] hiv, watery diarrhea sporulated oocytes [ CRYPTOSPOridium ]watery RN stain: sporulared oocyst PARUL 13]Note on lymphatic filarisis 14]Basic Lab D of fungal inferion (Baile pinoples). 15]Note on Histoplasmosis 16]causative agent of scoub typhus & lab diagnosis 17) PUO )18Indications of blood cuiture ?blood samples → collection & processing of 19)Diff between 1° & 2° Immune response à examples 20)life cycle & labd of taento douum 21)15ylo male, yever rever to AMA, responding t I chill sinu 4 days not Ancimia & opleenomegaly [ crescents MALARIA ]lab D etological agent t/t asnwer as per muhs exam systematically 2mbbs micro refer apurba shastri answer in detail and add colour diagrams easy to draw in exams as required as well cover details of answers
MUHS 2nd MBBS - MICROBIOLOGY - PAPER (Qs 6-21)
Q6. PRESCRIPTION - NOTE WITH APPLICATIONS
Parts of a Prescription:
╔══════════════════════════════════════════════════════════════════╗
║ PARTS OF PRESCRIPTION ║
║ ║
║ 1. SUPERSCRIPTION → Date, Patient name, age, sex, address, ║
║ IP/OP number ║
║ ║
║ 2. INSCRIPTION → Name of drug (generic/brand) ║
║ Dose, strength, dosage form ║
║ ║
║ 3. SUBSCRIPTION → Directions to pharmacist ║
║ (dispense X tablets/ml) ║
║ ║
║ 4. SIGNA (Sig) → Directions to patient ║
║ (1 tab BD x 5 days after food) ║
║ ║
║ 5. DOCTOR'S SIG → Signature, Reg. no., stamp ║
╚══════════════════════════════════════════════════════════════════╝
Sample Prescription (Microbiology context):
┌──────────────────────────────────────────────────────┐
│ Dr. A. Kumar, MBBS, MD │
│ Reg. No. MH-12345 │
│ OPD Room 4, Civil Hospital │
│ Date: 15/07/2026 │
│ │
│ Patient: Ram, 30yr/M IP No: 1234 │
│ │
│ Rx │
│ │
│ Tab. Doxycycline 100mg #14 │
│ 1-0-1 x 7 days (after food) │
│ (For: Scrub Typhus) │
│ │
│ Cap. Azithromycin 500mg #3 │
│ 1-0-0 x 3 days (with food) │
│ │
│ Sig: Take with plenty of water │
│ Avoid sun exposure │
│ Review after 5 days │
│ │
│ [Signature + Stamp] │
└──────────────────────────────────────────────────────┘
Applications (Microbiology context):
| Application | Example |
|---|---|
| Antibiotics for infections | Tab. Amoxicillin 500mg TID x 7 days for UTI |
| Antifungals | Cap. Fluconazole 150mg stat for candidiasis |
| Antiparasitics | Tab. Metronidazole 400mg TID x 10 days for amoebiasis |
| Antivirals | Tab. Acyclovir 400mg TID x 5 days for Herpes simplex |
| Vaccines | Inj. Hepatitis B vaccine 0.5ml IM on 0, 1, 6 months |
| ORS | Packet ORS - dissolve in 1L water, give as per dehydration |
Legal aspects:
- Schedule H drugs: prescription mandatory
- Schedule X drugs: prescription in duplicate, records maintained 2 years
- Generic prescription mandated by MCI (write INN names)
Q7. RICKETTSIAL INFECTIONS
Classification of Rickettsiae:
╔══════════════════════════════════════════════════════════════════╗
║ CLASSIFICATION OF RICKETTSIAE ║
║ ║
║ GENUS RICKETTSIA: ║
║ ├── Typhus Group: ║
║ │ ├── R. prowazekii → Epidemic typhus (louse) ║
║ │ └── R. typhi → Endemic/murine typhus (flea) ║
║ │ ║
║ ├── Spotted Fever Group: ║
║ │ ├── R. rickettsii → RMSF (tick) ║
║ │ ├── R. conorii → Boutonneuse fever (India) ║
║ │ └── R. akari → Rickettsialpox (mite) ║
║ │ ║
║ GENUS ORIENTIA: ║
║ └── O. tsutsugamushi → SCRUB TYPHUS (mite/chigger) ║
║ ║
║ GENUS COXIELLA: ║
║ └── C. burnetii → Q fever (no arthropod transmission) ║
╚══════════════════════════════════════════════════════════════════╝
Morphology (General):
- Small, pleomorphic, gram-negative coccobacilli
- Obligate intracellular parasites (cannot grow on artificial media)
- Stain: Giemsa, Machiavello, Castaneda (NOT gram stain reliably)
- Found in cytoplasm (Typhus group) or nucleus (Spotted fever group)
Scrub Typhus (most common in India - MUHS favourite):
- Chigger bites → organism enters skin → local eschar forms
- Spreads via lymphatics → bacteremia → endothelial cell invasion
- Perivascular inflammatory infiltrate
- Eschar (pathognomonic) - painless black ulcer at bite site
- Fever (high grade, remittent)
- Maculopapular rash (trunk → extremities, spares palms/soles)
- Lymphadenopathy
- Myalgia, headache
WEIL-FELIX REACTION TABLE (classic serological test):
╔═════════════════╦═══════╦═══════╦════════╗
║ Disease ║ OX-19 ║ OX-2 ║ OX-K ║
╠═════════════════╬═══════╬═══════╬════════╣
║ Epidemic typhus ║ +++ ║ + ║ - ║
║ Murine typhus ║ +++ ║ ++ ║ - ║
║ Scrub typhus ║ - ║ - ║ +++ ║
║ RMSF ║ ++ ║ +++ ║ - ║
║ Q fever ║ - ║ - ║ - ║
╚═════════════════╩═══════╩═══════╩════════╝
Lab Diagnosis of Rickettsial infections:
-
Weil-Felix Reaction - Agglutination of Proteus strains (OX-19, OX-2, OX-K)
- Titre ≥1:160 significant; 4-fold rise in paired sera diagnostic
- Cheap, widely available (but low specificity)
-
IFA (Immunofluorescence Assay) - GOLD STANDARD
- Most sensitive and specific
- Type-specific antibodies detected
-
ELISA - IgM/IgG antibodies
-
PCR - from whole blood; highly specific; early diagnosis
-
Weil-Felix test interpretation (see table above)
-
Isolation: BSL-3 facility required (not routine)
-
Skin biopsy of eschar: IHC or PCR for O. tsutsugamushi
- Doxycycline 100mg BD x 7 days (DOC for all rickettsial infections)
- Chloramphenicol (alternative, especially in children)
- Azithromycin (safe in pregnancy)
Q8. IMMUNOPATHOGENESIS AND LAB DIAGNOSIS OF RHD (Rheumatic Heart Disease)
Causative Agent: Streptococcus pyogenes (Group A Streptococcus)
Immunopathogenesis:
╔═══════════════════════════════════════════════════════════════╗
║ IMMUNOPATHOGENESIS OF RHD ║
║ ║
║ GAS PHARYNGITIS ║
║ ↓ [M protein antigen + streptolysins] ║
║ IMMUNE RESPONSE triggered (2-4 weeks later) ║
║ ↓ ║
║ Antibodies formed against: ║
║ ├── Anti-M protein antibodies ║
║ ├── Anti-streptolysin O (ASO) antibodies ║
║ └── Anti-hyaluronidase, Anti-streptokinase ║
║ ↓ ║
║ MOLECULAR MIMICRY: ║
║ M protein epitopes = similar to: ║
║ ├── Cardiac MYOSIN (sarcolemma) ║
║ ├── Laminin (heart valve endothelium) ║
║ └── Cardiac tropomyosin ║
║ ↓ ║
║ Cross-reactive antibodies attack HEART TISSUE: ║
║ ├── VALVES (mitral most common) ║
║ ├── Myocardium (Aschoff bodies - pathognomonic) ║
║ └── Pericardium ║
║ ↓ ║
║ RHEUMATIC FEVER → Repeated attacks → ║
║ CHRONIC RHD (mitral stenosis, regurgitation) ║
╚═══════════════════════════════════════════════════════════════╝
- Only pharyngeal GAS → RHD (NOT skin infections)
- Rheumatogenic strains: M types 1, 3, 5, 6, 14, 18, 19, 24
- Aschoff bodies (pathognomonic): perivascular granulomas with Anitschkow cells
Lab Diagnosis of RHD:
- Culture on Blood agar → beta-hemolytic colonies
- Gram stain: gram +ve cocci in chains
- Catalase negative, PYR positive
- Bacitracin sensitivity (Zone ≥10mm = Group A)
- Lancefield grouping with anti-A antiserum
- Rapid Strep Test (Lateral flow) for GAS antigen from throat swab
- Sensitivity ~70-80%
| Test | Antigen detected | Normal | Elevated in |
|---|---|---|---|
| ASO titre | Anti-streptolysin O | <200 IU/mL (adults) | Acute RF/recent GAS infection |
| Anti-DNase B | Anti-deoxyribonuclease B | <240 IU/mL | More sensitive for skin GAS |
| Anti-hyaluronidase | Anti-hyaluronidase | - | Supplement ASO |
| Streptozyme test | Multiple antigens | - | Screening |
-
200 Todd units in adults, >333 in children = significant
- 4-fold rise in paired sera (2-4 weeks apart) = recent infection
MAJOR CRITERIA: MINOR CRITERIA:
• Carditis • Fever
• Polyarthritis • Prolonged PR interval (ECG)
• Chorea • Elevated ESR/CRP
• Erythema marginatum • Leucocytosis
• Subcutaneous nodules • Previous RF/RHD
Diagnosis: 2 Major OR 1 Major + 2 Minor
+ Evidence of preceding GAS infection (ASO/culture)
- Acute: Benzathine Penicillin G 1.2 MU IM single dose
- Secondary prophylaxis: Benzathine Penicillin G 1.2 MU IM every 3 weeks for minimum 5 years / up to age 21
Q9. LABORATORY DIAGNOSIS OF LEPTOSPIROSIS
Clinical Phases:
- Phase 1 (Leptospiremic): Days 1-7, fever, headache, myalgia (bacteria in blood and CSF)
- Phase 2 (Immune): Days 7-14, antibody production, bacteria clear from blood; Weil's disease (jaundice, renal failure, hemorrhage)
DIAGRAM - Lab Diagnosis Strategy by Phase:
╔══════════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS OF LEPTOSPIROSIS ║
║ ║
║ WEEK 1 (leptospiremic phase): ║
║ ├── Blood culture (EMJH medium or Fletcher's medium) ║
║ ├── CSF culture (if meningitic) ║
║ ├── Urine (from day 7 onwards) ║
║ ├── PCR (blood/urine) - most sensitive, early ║
║ └── Dark-field microscopy (blood - not reliable) ║
║ ║
║ WEEK 2 onwards (immune phase): ║
║ ├── SEROLOGY (antibodies appear) ║
║ │ ├── MAT (Microscopic Agglutination Test) - GOLD STANDARD║
║ │ ├── IgM ELISA (Panbio, Leptocheck - rapid) ║
║ │ └── Macroscopic slide agglutination test (screening) ║
║ └── Urine culture (organisms shed in urine) ║
╚══════════════════════════════════════════════════════════════╝
Detailed Lab Methods:
- Blood (early), urine (late)
- Thin, motile coiled organisms with hooked ends seen
- Low sensitivity; false positives common (fibrin threads confused)
- EMJH (Ellinghausen-McCullough-Johnson-Harris) medium or Fletcher's semi-solid medium
- Incubate at 28-30°C for 6-8 weeks (slow growing)
- Positive in 50-70% early cases
- Blood in first week; urine from day 7
- Highly sensitive and specific; used in India increasingly
- GOLD STANDARD for serology
- Uses live or formalin-killed Leptospira antigens + patient serum
- Titre ≥1:100 in single sample suggestive
- 4-fold rise in paired sera (2 weeks apart) = diagnostic
- Can identify specific serovar (important epidemiologically)
- Detects IgM antibodies from day 5-7
- Commercially available kits (Panbio Leptospira IgM ELISA)
- Sensitivity ~90%, Specificity ~95%
- Screening test; uses killed antigens; simple
- Titre ≥1:40 = significant
Leptospira - "?" shaped / hooked ends
├── Thin, tightly coiled
├── 6-20 μm long
├── Stain: Silver impregnation (Fontana's stain), Giemsa
└── Dark field: glistening, rapidly rotating
Q10. NACO STRATEGIES FOR HIV
Major Strategies under NACP (National AIDS Control Programme):
╔══════════════════════════════════════════════════════════════╗
║ NACO STRATEGIES FOR HIV ║
║ ║
║ 1. PREVENTION STRATEGIES ║
║ ├── IEC (Information, Education, Communication) ║
║ ├── BCC (Behaviour Change Communication) ║
║ ├── Condom promotion (NACO provides free condoms) ║
║ ├── STI management (treat STIs → reduce HIV risk) ║
║ ├── ICTC (Integrated Counselling & Testing Centres) ║
║ ├── Blood Safety (mandatory HIV screening of all blood) ║
║ ├── Harm Reduction for IDUs (needle exchange, OST) ║
║ └── PMTCT (Prevention of Mother to Child Transmission) ║
║ ║
║ 2. CARE, SUPPORT & TREATMENT ║
║ ├── ART Centres (Free ART under NACP IV) ║
║ ├── CD4 & Viral Load monitoring ║
║ ├── OI (Opportunistic Infection) management ║
║ └── Nutritional support ║
║ ║
║ 3. TARGETED INTERVENTIONS (TI) ║
║ ├── FSW (Female Sex Workers) ║
║ ├── MSM (Men having Sex with Men) ║
║ ├── IDU (Injecting Drug Users) ║
║ └── Transgender community ║
║ ║
║ 4. RESEARCH & SURVEILLANCE ║
║ ├── ANC sentinel surveillance ║
║ ├── IBBS (Integrated Biological Behavioural Surveillance) ║
║ └── HIV estimations (UNAIDS methodology) ║
╚══════════════════════════════════════════════════════════════╝
Key NACO Programmes:
| Programme | Details |
|---|---|
| PMTCT | All HIV+ pregnant women → ART (TDF+3TC+EFV) → infant NVP for 6 weeks |
| ART Programme | Free first-line ART: TDF+3TC+EFV (TLE) regimen for all HIV+ |
| ICTC | Free HIV testing + pre/post-test counselling at all district hospitals |
| OST | Opioid Substitution Therapy (Buprenorphine/Methadone) for IDUs |
| Blood Safety | Mandatory HIV, HBV, HCV, Malaria, Syphilis screening of ALL donated blood |
| PPTCT | Prevention of Parent to Child Transmission - universal ART for mothers |
| SACS | State AIDS Control Society - state-level implementation |
- ALL HIV-positive individuals started on ART regardless of CD4 count
- First-line: TDF + 3TC (or FTC) + EFV (TLE regimen)
- Pediatric: ABC + 3TC + EFV
Q11. HIV - LAB DIAGNOSIS
Classification of Tests:
╔════════════════════════════════════════════════════════════════╗
║ HIV LAB DIAGNOSIS ALGORITHM ║
║ ║
║ SCREENING TESTS (Sensitive): ║
║ ├── ELISA (4th generation: detects Ag+Ab) ║
║ ├── Rapid immunochromatography tests ║
║ └── Chemiluminescent immunoassay (CLIA) ║
║ ║
║ CONFIRMATORY TEST: ║
║ └── Western Blot (detects specific band pattern) ║
║ ║
║ SUPPLEMENTAL/ADVANCED: ║
║ ├── HIV RNA PCR (Viral Load) - quantitative ║
║ ├── HIV DNA PCR - for infants <18 months ║
║ ├── p24 Antigen assay ║
║ └── CD4 count - monitoring, not diagnosis ║
╚════════════════════════════════════════════════════════════════╝
NACO Testing Strategy (Rapid Tests - India):
NACO ALGORITHM:
Patient comes for HIV testing
↓
Test A (ELISA/Rapid)
↓
Non-reactive → HIV NEGATIVE
Reactive ↓
Test B (different antigen/format)
↓
Non-reactive → Discordant → Test C → report
Reactive ↓
Test C (third test)
↓
Reactive → HIV POSITIVE
Non-reactive → INDETERMINATE → repeat in 2-4 weeks
Detail of Individual Tests:
- Detects both p24 antigen AND anti-HIV antibodies
- Window period: 11-15 days (4th gen) vs 22-25 days (3rd gen)
- Very high sensitivity (>99.5%)
- False positives in: malaria, pregnancy, autoimmune disease
- Detects antibodies to specific HIV proteins
- POSITIVE: bands at p24 + gp41 + gp120/160 (CDC criteria: ≥2 bands from p24, gp41, gp120/160)
- Highest specificity
- Detects HIV RNA copies/mL blood
- Used for: early diagnosis (acute HIV), monitoring ART response, diagnosis in infants
- Undetectable VL (<20-50 copies/mL) = treatment success
- Normal: 500-1500 cells/μL
- <500: Start ART (India: all cases)
- <200: AIDS-defining; start OI prophylaxis (Cotrimoxazole)
- <50: Very high risk for CMV, MAC
- Appears before antibodies (11-14 days post infection)
- Used in 4th gen combo assays
- Two positive tests on the same day with different antigens = HIV positive
Q12. CRYPTOSPORIDIUM - Note / HIV with watery diarrhea + sporulated oocysts
- Phylum: Apicomplexa (Sporozoa)
- Class: Coccidia
- Intracellular parasite of intestinal epithelium
Morphology:
- Oocysts: 4-5 μm (small, spherical), contain 4 sporozoites
- Thick-walled oocysts: shed in stool (environmental transmission)
- Thin-walled oocysts: auto-infection (rupture within gut)
Life Cycle:
╔══════════════════════════════════════════════════════════════╗
║ LIFE CYCLE OF CRYPTOSPORIDIUM ║
║ ║
║ THICK-WALLED OOCYSTS (infective form) ║
║ ↓ [ingested in contaminated water/food] ║
║ EXCYSTATION in small intestine ║
║ ↓ ║
║ 4 SPOROZOITES released → attach to brush border ║
║ ↓ ║
║ MEROGONY (asexual): ║
║ Type I meronts → 8 merozoites → new Type I (cycle) ║
║ Type II meronts → 4 merozoites → SEXUAL phase ║
║ ↓ ║
║ GAMETOGONY (sexual): ║
║ Microgamont (male) + Macrogamont (female) → ZYGOTE ║
║ ↓ ║
║ OOCYSTS formed: ║
║ ├── THICK-WALLED → shed in stool (80%) ║
║ └── THIN-WALLED → autoinfection (20%) ║
╚══════════════════════════════════════════════════════════════╝
Clinical Features:
- Immunocompetent: Mild, self-limiting watery diarrhea (1-2 weeks)
- AIDS (CD4 <200): Profuse, cholera-like watery diarrhea (3-20 L/day), wasting, prolonged, may be fatal
- Associated with: biliary cryptosporidiosis, pulmonary involvement in AIDS
Lab Diagnosis:
- Oocysts stain pink/red against blue background
- Size: 4-5 μm
- PARUL mnemonic: Pink oocysts on Acid-fast stain, Round, Under Light microscope
DIAGRAM - Modified ZN Stain:
╔══════════════════════════════════════╗
║ Blue background (counterstain) ║
║ ║
║ ● ● ● ← PINK oocysts (4-5μm) ║
║ ● ● ● (sporulated) ║
║ ● ● ● ║
║ ║
║ = Cryptosporidium oocysts ║
╚══════════════════════════════════════╝
- Best sensitivity for oocyst detection
- Uses fluorescently labelled monoclonal antibodies
- Highly sensitive and specific
- Organisms at brush border (apex of villi)
- PAS stain: purple dots at luminal surface
- Immunocompetent: Supportive (self-limiting)
- AIDS patients: Nitazoxanide 500mg BD x 3 days + ART (ART is most important - restores immunity)
- Paromomycin + Azithromycin (adjunct)
Q13. NOTE ON LYMPHATIC FILARIASIS
Morphology of Microfilariae:
╔══════════════════════════════════════════════════════════╗
║ W. bancrofti vs B. malayi - MICROFILARIAE ║
║ ║
║ W. bancrofti: B. malayi: ║
║ • Sheath present • Sheath present ║
║ • NO nuclei in tail tip • 2 nuclei in tail tip ║
║ • Sheath does NOT stain • Sheath stains PINK ║
║ with Giemsa with Giemsa ║
║ • Body nuclei: not reach tip • Subterminal space ║
║ ║
║ PERIODICITY: ║
║ • Nocturnal periodicity (appear in blood at night) ║
║ • Except: Pacific strain (W. bancrofti) - diurnal ║
╚══════════════════════════════════════════════════════════╝
Life Cycle:
╔════════════════════════════════════════════════════════════╗
║ LIFE CYCLE OF W. BANCROFTI ║
║ ║
║ MOSQUITO (Culex): ║
║ Ingests microfilariae with blood meal ║
║ ↓ ║
║ Mf develop in flight muscle: ║
║ L1 → L2 → L3 (infective larva - filariform) ║
║ ↓ migrate to proboscis ║
║ L3 deposited on skin during blood meal ║
║ ↓ enters through bite wound ║
║ HUMAN HOST: ║
║ L3 → lymphatics → L4 → ADULT WORMS ║
║ (Male + Female mate in lymph nodes) ║
║ ↓ ║
║ Females release microfilariae → bloodstream ║
║ ↓ (Nocturnal periodicity: appear at night) ║
║ Microfilariae in peripheral blood ║
║ (taken up by mosquito to continue cycle) ║
╚════════════════════════════════════════════════════════════╝
Pathogenesis:
- Dead worms → lymphangitis, lymphadenitis
- Repeated episodes → fibrosis, obstruction of lymphatics
- Lymphedema → chronic → Elephantiasis (limbs, scrotum/hydrocele, vulva)
- Tropical Pulmonary Eosinophilia (TPE): Aberrant immune response → Mf trapped in lungs → eosinophilia >3000/μL, cough, wheeze
Lab Diagnosis:
- Collect blood at NIGHT (11pm-1am) for nocturnal periodicity
- Thick film: Giemsa stain
- Look for microfilariae (sheathed)
- Knott's technique: 1ml blood + 9ml 2% formalin → centrifuge → sediment examined
- Membrane filtration (Nuclepore): blood filtered through 3μm pore filter
- Detects W. bancrofti circulating filarial antigen (CFA)
- ICT Filariasis test (BinaxNOW)
- Can be done at any time (not limited to night)
- Sensitivity >95%; blood collected anytime
- ELISA for IgG4 (anti-filarial antibodies)
- Less specific due to cross-reactions
- "Filarial dance sign" - live moving adult worms in scrotal/lymph node ultrasound
- DEC (Diethylcarbamazine citrate) 6mg/kg/day x 12 days (kills microfilariae + some adult worms)
- Ivermectin + Albendazole (MDA - Mass Drug Administration programme, India)
- Doxycycline: kills Wolbachia (endosymbiont of filariae) → kills adult worms
Q14. BASIC LAB DIAGNOSIS OF FUNGAL INFECTIONS
Specimens by site:
- Skin: Skin scrapings (from active edge of lesion)
- Hair: Infected hair shaft + kerion
- Nails: Nail clippings
- Deep infections: BAL, sputum, CSF, tissue biopsy, blood
DIAGRAM - Overview of Fungal Lab Diagnosis:
╔══════════════════════════════════════════════════════════════╗
║ FUNGAL LAB DIAGNOSIS OVERVIEW ║
║ ║
║ 1. DIRECT MICROSCOPY ║
║ ├── KOH Mount (10-20% KOH) - GOLD STANDARD for superficial ║
║ │ Dissolves keratin → reveals fungal elements ║
║ │ See: hyphae, spores, pseudohyphae ║
║ ├── India Ink Preparation (Cryptococcus neoformans) ║
║ │ Capsule appears as clear halo around yeast ║
║ ├── Gram stain: Candida (gram +ve pseudohyphae) ║
║ ├── ZN stain: Not useful ║
║ └── Calcofluor white stain (fluorescence) - most sensitive ║
║ ║
║ 2. CULTURE ║
║ ├── SDA (Sabouraud's Dextrose Agar) - BASIC MEDIUM ║
║ │ pH 5.6, temp 22-28°C, chloramphenicol added ║
║ │ Inhibits bacteria ║
║ ├── Dermatophyte Test Medium (DTM) - dermatophytes ║
║ ├── CHROMagar Candida - Candida speciation by color ║
║ └── BHI agar - systemic/dimorphic fungi ║
║ ║
║ 3. BIOCHEMICAL/IDENTIFICATION ║
║ ├── Germ tube test (Candida albicans) ║
║ ├── Sugar fermentation/assimilation tests ║
║ └── MALDI-TOF (modern rapid ID) ║
║ ║
║ 4. SEROLOGY/ANTIGEN DETECTION ║
║ ├── Cryptococcal antigen (LA/ELISA) - CrAg ║
║ ├── Galactomannan (Aspergillus antigen) - ELISA ║
║ ├── Beta-D-glucan (panfungal marker) ║
║ └── Histoplasma antigen (urine/serum) ║
║ ║
║ 5. MOLECULAR/PCR ║
║ └── Panfungal PCR, species-specific PCR ║
╚══════════════════════════════════════════════════════════════╝
Key Stains Summary:
| Stain | Uses |
|---|---|
| KOH mount | Superficial mycoses, all fungi |
| India Ink | Cryptococcus capsule |
| PAS stain | Fungal hyphae (magenta) in tissue |
| GMS (Gomori Methenamine Silver) | Best for tissue sections; black hyphae |
| Gram stain | Candida pseudohyphae |
| Calcofluor white | Best sensitivity (fluorescent) |
| Fontana-Masson | Melanin in Cryptococcus |
Germ Tube Test (for C. albicans):
- Incubate Candida in human serum at 37°C for 2-3 hours
- True germ tube (no constriction at origin) = C. albicans positive
- Distinguishes C. albicans from other Candida species
Q15. NOTE ON HISTOPLASMOSIS
- Thermally dimorphic fungus
- Mold at 25°C (in environment), Yeast at 37°C (in tissue)
Epidemiology:
- Found in soil rich in bird/bat droppings (caves, chicken coops)
- Endemic: Ohio and Mississippi River valleys (USA), India (rare but reported)
- Inhalation of microconidia = mode of infection
- High-risk groups: cave explorers (spelunkers), demolition workers, farmers
Morphology:
╔══════════════════════════════════════════════════════╗
║ HISTOPLASMA CAPSULATUM - MORPHOLOGY ║
║ ║
║ IN ENVIRONMENT (25°C) - MOLD PHASE: ║
║ ├── Septate hyphae ║
║ ├── Tuberculate macroconidia (diagnostic) ║
║ │ [large, thick-walled, spiky/spiked surface] ║
║ └── Microconidia (2-4μm, smooth) - INFECTIVE ║
║ ║
║ IN TISSUE (37°C) - YEAST PHASE: ║
║ ├── Small oval yeast cells (2-4 μm) ║
║ ├── INTRACELLULAR in macrophages ║
║ ├── Narrow-based budding ║
║ └── "Ring of haze" around each yeast (not capsule) ║
╚══════════════════════════════════════════════════════╝
Clinical Forms:
| Form | Features |
|---|---|
| Asymptomatic | 90% of cases; subclinical, heals with calcification |
| Acute pulmonary | Flu-like, 1-3 weeks; self-limiting; low inoculum |
| Chronic pulmonary | Resembles TB; cavitary lesions; COPD patients |
| Disseminated | AIDS, immunocompromised; fever, hepatosplenomegaly, pancytopenia |
| African (H. duboisii) | Skin ulcers, bone lesions |
Lab Diagnosis:
- Direct microscopy (Giemsa/PAS): Intracellular oval yeasts in macrophages in BAL, bone marrow, peripheral blood buffy coat
- Culture (SDA/BHI): 25°C → mold with tuberculate macroconidia; 37°C → yeast (takes 2-6 weeks; BSL-3)
- Histoplasma antigen detection (ELISA): Urine/serum; most useful in disseminated disease; sensitivity >90% in AIDS
- Complement Fixation (CF) + Immunodiffusion (ID): M and H precipitin bands; H band = active infection
- PCR: Rapid, sensitive
- Skin test (Histoplasmin): Epidemiological tool only (not diagnostic)
- Mild: Itraconazole 200mg BD x 3-12 months
- Severe/Disseminated: Liposomal Amphotericin B → then Itraconazole
- AIDS: lifelong secondary prophylaxis with Itraconazole
Q16. CAUSATIVE AGENT OF SCRUB TYPHUS AND LAB DIAGNOSIS
- Vector: Larval trombiculid mite (chigger) - Leptotrombidium deliense
- Reservoir: Wild rodents (rats, mice); mites are also reservoir (transovarial transmission)
- Mode of transmission: Bite of infected chigger larva
Morphology:
- Obligate intracellular gram-negative coccobacillus
- Found in cytoplasm AND nucleus of host cells
- Cannot be cultured on routine bacteriological media
Clinical Features:
- Eschar (black ulcer at bite site - pathognomonic) - present in 50-80% cases
- Fever, headache, myalgia
- Generalized lymphadenopathy (including eschar-draining node)
- Maculopapular rash (trunk → periphery)
- Complications: meningoencephalitis, ARDS, myocarditis, renal failure
Lab Diagnosis:
SPECIMEN: Blood (EDTA - for PCR, culture); Eschar biopsy
╔═══════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS OF SCRUB TYPHUS ║
║ ║
║ 1. WEIL-FELIX REACTION (Traditional, cheap): ║
║ OX-K agglutination positive (titre ≥1:80 significant) ║
║ OX-19 and OX-2 = NEGATIVE ║
║ (Cross-reaction with Proteus OX-K antigen) ║
║ ║
║ 2. IFA (Gold standard): ║
║ Anti-O. tsutsugamushi IgM/IgG antibodies ║
║ Titre ≥1:50 = positive; 4-fold rise = diagnostic ║
║ ║
║ 3. PCR (Early, best test): ║
║ Real-time PCR from blood/eschar biopsy ║
║ Detects 47kDa gene of Orientia ║
║ Most sensitive in first week ║
║ ║
║ 4. Eschar biopsy: ║
║ IHC (immunohistochemistry) or PCR ║
║ Confirms organism in tissue ║
║ ║
║ 5. ELISA (IgM): ║
║ Positive from day 7-10 ║
║ Commercially available kits ║
║ ║
║ 6. Isolation: ║
║ Mouse inoculation / cell culture (L-929 cells) ║
║ BSL-3 - not routine ║
╚═══════════════════════════════════════════════════════════╝
- Doxycycline 100mg BD x 7 days (DOC)
- Alternatives: Azithromycin (safe in pregnancy), Chloramphenicol
- Rapid response to Doxycycline is itself a therapeutic test (defervescence within 24-48 hrs)
Q17. PUO (Pyrexia of Unknown Origin)
- Fever >38.3°C (101°F)
- Duration >3 weeks
- No diagnosis after 1 week of in-hospital investigation
Classification:
| Type | Setting | Common Causes |
|---|---|---|
| Classic PUO | Community | Infections (TB), Neoplasms (lymphoma), Collagen vascular disease (SLE) |
| Nosocomial PUO | Hospitalized >24hrs | Drug fever, DVT/PE, Sinusitis, C. diff |
| Neutropenic PUO | ANC <500 | Bacterial/fungal infections |
| HIV-associated PUO | HIV patients | MAC, CMV, PCP, Lymphoma |
Causes (Classic Triad: 30-30-20-10-10):
- Infections: 30% (TB most common in India, SBE, abscess)
- Neoplasms: 30% (Lymphoma, leukemia, solid tumors)
- Collagen vascular diseases: 20% (SLE, RA, Vasculitis)
- Miscellaneous: 10% (Drug fever, Factitious fever)
- Undiagnosed: 10%
Microbiological Lab Workup:
STEP-BY-STEP APPROACH:
┌──────────────────────────────────────────────────────────┐
│ BASIC (all cases): │
│ • CBC with differential (eosinophilia? leukocytosis?) │
│ • Blood cultures x 3 (aerobic + anaerobic, 12 hrs apart)│
│ • Urine culture │
│ • ESR, CRP, Procalcitonin │
│ • Widal test (if Salmonella suspected) │
│ • Weil-Felix (Rickettsial infections) │
│ • Malaria MP/RDT │
│ │
│ DIRECTED (based on clinical clues): │
│ • Mantoux + Sputum AFB/CBNAAT (TB) │
│ • ANA, anti-dsDNA (SLE) │
│ • ECHO (SBE/endocarditis) │
│ • Bone marrow exam (Leishmania, Typhoid, Malaria) │
│ • Serology: Leptospira IgM, Brucella, Dengue NS1 │
│ • CT chest/abdomen (lymphoma, abscess) │
│ • PET-CT scan (occult malignancy/infection) │
│ • Tissue biopsy (LN, liver, bone marrow) │
└──────────────────────────────────────────────────────────┘
Q18. INDICATIONS OF BLOOD CULTURE - COLLECTION AND PROCESSING
Indications for Blood Culture:
- Suspected bacteremia/septicemia (fever >38.5°C with rigors)
- Endocarditis (suspected SBE - 3 sets mandatory)
- PUO (pyrexia of unknown origin)
- Typhoid fever (best yield in first week)
- Meningitis (blood culture + CSF culture together)
- Neonatal sepsis
- Immunocompromised patients with fever
- Post-operative fever (>48 hrs after surgery)
- Catheter-related bloodstream infection (CRBSI)
Collection of Blood for Culture:
╔══════════════════════════════════════════════════════════════╗
║ BLOOD CULTURE COLLECTION PROTOCOL ║
║ ║
║ TIMING: Collect at PEAK OF FEVER (during rigor/chill) ║
║ OR before antibiotic administration ║
║ ║
║ SITE: Peripheral vein (antecubital fossa) ║
║ NOT from existing IV line (contamination risk) ║
║ ║
║ VOLUME: ║
║ Adults: 10 mL per bottle (5 mL aerobic + 5 mL anaerobic) ║
║ Children: 1-5 mL ║
║ Neonates: 0.5-1 mL ║
║ ║
║ NUMBER OF SETS: Minimum 2 sets (from 2 different sites) ║
║ SBE: 3 sets in 24 hours ║
║ ║
║ BLOOD:BROTH RATIO: 1:10 (dilutes inhibitors like Ab) ║
║ ║
║ ASEPTIC TECHNIQUE: ║
║ 1. Clean skin with 70% alcohol → dry ║
║ 2. Apply 2% chlorhexidine or povidone-iodine ║
║ 3. Allow to dry 30 seconds ║
║ 4. Venepuncture with sterile needle ║
║ 5. Change needle before inoculating bottle ║
╚══════════════════════════════════════════════════════════════╝
Processing of Blood Culture:
- Inoculate BHI (Brain Heart Infusion) broth / Tryptic Soy Broth
- Incubate at 37°C, inspect daily for 7 days for turbidity, gas, hemolysis
- Blind subculture at 24hrs, 48hrs, 7 days on blood agar + MacConkey
- Continuously monitor CO2 production (by-product of bacterial metabolism)
- Alert when positive (usually within 12-24 hrs for common organisms)
- Sensitivity >97%
- Flagged positives → Gram stain → Subculture → ID + Sensitivity
- Gram stain of positive bottle
- Subculture on appropriate media
- Species identification (MALDI-TOF or conventional biochemicals)
- Antimicrobial susceptibility testing (Kirby-Bauer or MIC by broth dilution)
Q19. DIFFERENCE BETWEEN PRIMARY AND SECONDARY IMMUNE RESPONSE
╔════════════════════════════════════════════════════════════════════╗
║ PRIMARY vs SECONDARY IMMUNE RESPONSE ║
╠═════════════════════════╦═══════════════════╦══════════════════════╣
║ Feature ║ PRIMARY ║ SECONDARY ║
╠═════════════════════════╬═══════════════════╬══════════════════════╣
║ Trigger ║ First exposure ║ Re-exposure (booster)║
║ Lag phase ║ 5-10 days ║ 1-3 days ║
║ Magnitude (Ab titre) ║ Low ║ Much HIGHER ║
║ Duration ║ Shorter ║ Longer ║
║ Antibody class ║ IgM first → IgG ║ Mainly IgG ║
║ Affinity ║ Lower ║ HIGHER (affinity ║
║ ║ ║ maturation) ║
║ Cells involved ║ Naive B + T cells ║ Memory B + T cells ║
║ Memory cells formed ║ YES (first time) ║ YES (expanded) ║
╚═════════════════════════╩═══════════════════╩══════════════════════╝
DIAGRAM:
Ab
Titre │ ╭─────────── (Secondary)
(log) │ / MUCH HIGHER
│ /
│ ╭────────────/
│ / (Primary)
│ /
│───────────/
│(lag)
└──────────────────────────────────────────
1st Ag 2nd Ag (re-exposure)
exposure
← 5-10 day lag → ← 1-3 day lag →
Basis of Secondary Response (MEMORY CELLS):
- After primary exposure: long-lived Memory B cells and Memory T cells formed
- Memory cells persist for years to decades
- On re-exposure → rapid clonal expansion → fast, high-magnitude, high-affinity Ab response
Applications (Examples):
| Principle | Example |
|---|---|
| Immunization (PRIMARY response) | First dose Hepatitis B vaccine - IgM response, low titre |
| Booster doses (SECONDARY response) | 2nd and 3rd Hepatitis B dose - high IgG, lifelong protection |
| DPT schedule | Primary series (0,2,4,6 months) + booster (18 months) = secondary response |
| Anamnesis (recall reaction) | Patient with past TB, re-exposed → rapid Mantoux positivity |
| Blood group antibodies | Anti-A/B are IgM (natural antibodies - no prior exposure pattern) |
| Secondary immune response explains why: | Second infection with same pathogen is milder or asymptomatic |
Q20. LIFE CYCLE AND LAB DIAGNOSIS OF TAENIA SOLIUM
- Taeniasis (intestinal): adult tapeworm in intestine (man = definitive host)
- Cysticercosis (tissue): larval cysts (man = accidental intermediate host) - MORE DANGEROUS
Life Cycle:
╔══════════════════════════════════════════════════════════════════╗
║ LIFE CYCLE OF TAENIA SOLIUM ║
║ ║
║ DEFINITIVE HOST: Human ║
║ NORMAL INTERMEDIATE HOST: Pig ║
║ ACCIDENTAL INTERMEDIATE HOST: Human (cysticercosis) ║
║ ║
║ ┌─── NORMAL CYCLE ──────────────────────────────────────┐ ║
║ │ │ ║
║ │ ADULT WORM in human small intestine │ ║
║ │ ↓ gravid proglottids shed in stool │ ║
║ │ EGGS in environment │ ║
║ │ ↓ PIG ingests eggs from contaminated soil │ ║
║ │ ONCOSPHERE hatches in pig gut │ ║
║ │ ↓ penetrates gut wall → blood → muscles │ ║
║ │ CYSTICERCUS CELLULOSAE in pig muscle (pork) │ ║
║ │ ↓ human eats undercooked infected pork │ ║
║ │ SCOLEX evaginates in human intestine │ ║
║ │ ↓ attaches to mucosa │ ║
║ │ ADULT WORM (2-7m long) develops │ ║
║ └────────────────────────────────────────────────────────┘ ║
║ ║
║ ┌─── CYSTICERCOSIS CYCLE (DANGEROUS) ──────────────────┐ ║
║ │ Human ingests EGGS (from contaminated food/water, │ ║
║ │ or autoinfection - gravid proglottids regurgitate) │ ║
║ │ ↓ Oncospheres hatch │ ║
║ │ Penetrate gut → bloodstream → TISSUES │ ║
║ │ ├── BRAIN → Neurocysticercosis (NCC) - COMMONEST │ ║
║ │ ├── Eye, muscles, heart, skin │ ║
║ │ └── Cysticercus cellulosae forms (fluid-filled cyst)│ ║
║ └──────────────────────────────────────────────────────┘ ║
╚══════════════════════════════════════════════════════════════════╝
Morphology of Adult Worm:
SCOLEX (head):
┌────────────────────────────────────┐
│ 4 SUCKERS (acetabula) │
│ ROSTELLUM with double row of HOOKS│ ← Armed (distinguishes from T. saginata)
│ (T. saginata has NO hooks) │
└────────────────────────────────────┘
NECK → PROGLOTTIDS
├── Immature proglottids
├── Mature proglottids (5-10: uterine branches per side)
└── Gravid proglottids (7-13 uterine branches per side)
T. saginata has 15-30 branches
Lab Diagnosis:
-
Stool examination:
- Wet preparation or concentration (ZnSO4 floatation / formol-ether)
- Find: Eggs - round/oval, 30-40μm, thick brown striated shell, 6-hooked oncosphere inside
- Eggs of T. solium and T. saginata are morphologically IDENTICAL
- Find: Gravid proglottids - count uterine branches (<13 = T. solium; >15 = T. saginata)
-
Scolex examination: After treatment (praziquantel/niclosamide) - identify by presence/absence of hooks
-
Perianal swab (Graham's test): Less useful than for Enterobius, but proglottids may be detected
-
Neuroimaging (CT/MRI brain):
- MRI: Fluid-filled cysts with eccentric scolex (hypodense lesion + bright scolex = "hole with a dot" sign)
- CT: Calcified cysts (dead worms), perilesional edema
-
Serology:
- ELISA (IgG anti-cysticercal antibodies) - sensitivity 75-95% in NCC
- EITB (Enzyme-linked immunoelectrotransfer blot) - most specific
-
CSF examination (NCC with meningitis):
- Eosinophilic pleocytosis, elevated protein
- CSF ELISA positive
-
Subcutaneous nodule biopsy:
- Cysticercus cellulosae identified histologically
- Bladder-like structure with invaginated scolex and 4 suckers
-
PCR: Highly sensitive for CSF/blood
- Taeniasis: Praziquantel 10mg/kg single dose OR Niclosamide
- NCC: Albendazole 15mg/kg/day x 8-28 days (+ Dexamethasone for edema)
- Calcified cysts: No antiparasitic needed; manage seizures with anticonvulsants
Q21. 15-year-old male, fever not responding to antibiotics, chills for 4 days, anemia, splenomegaly, CRESCENTS on smear
Etiological Agent: Plasmodium falciparum
| Feature | Significance |
|---|---|
| Crescents (banana/sickle-shaped gametocytes) | Pathognomonic of P. falciparum |
| Fever not responding to co-amoxiclav etc. | Parasitic, not bacterial cause |
| Anemia | Hemolysis of RBCs |
| Splenomegaly | Phagocytosis of infected RBCs |
| Age 15, fever with chills | Classic malarial paroxysm |
Classification:
| Species | Periodicity | Severity | RBC affected |
|---|---|---|---|
| P. vivax | 48 hrs (Benign Tertian) | Benign | Reticulocytes |
| P. ovale | 48 hrs (Ovale Tertian) | Benign | Reticulocytes |
| P. malariae | 72 hrs (Quartan) | Benign | Old RBCs |
| P. falciparum | 36-48 hrs (Malignant Tertian) | SEVERE | All ages RBCs |
Life Cycle:
╔══════════════════════════════════════════════════════════════════╗
║ LIFE CYCLE OF PLASMODIUM (Two-host cycle) ║
║ ║
║ ANOPHELES MOSQUITO (definitive host - sexual cycle): ║
║ ├── Ingests gametocytes from infected human ║
║ ├── Microgamete + Macrogamete → ZYGOTE → OOKINETE ║
║ ├── Ookinete → OOCYST in stomach wall ║
║ └── SPOROZOITES released → migrate to salivary glands ║
║ ║
║ HUMAN (intermediate host - asexual cycle): ║
║ ├── SPOROZOITES injected with mosquito bite ║
║ │ ║
║ ├── EXOERYTHROCYTIC (Pre-erythrocytic) cycle in LIVER: ║
║ │ Sporozoites → hepatocytes → LIVER SCHIZONTS ║
║ │ → 10,000 MEROZOITES / liver cell ║
║ │ P. vivax/ovale: HYPNOZOITES (dormant, relapse) ║
║ │ ║
║ └── ERYTHROCYTIC cycle in RBCs: ║
║ Merozoites → invade RBCs ║
║ RING STAGE → TROPHOZOITE → ERYTHROCYTIC SCHIZONT ║
║ → MEROZOITES (rupture RBC → fever/chills) ║
║ → Some → GAMETOCYTES (P. falciparum = CRESCENTS) ║
╚══════════════════════════════════════════════════════════════════╝
P. falciparum - Specific features:
- Ring stage: Multiple rings per RBC (polyinfection), Maurer's clefts in cytoplasm
- Infected RBCs: NOT enlarged (unlike P. vivax); show knobs (cytoadherence)
- Sequestration: infected RBCs stick to capillary endothelium (PfEMP1 protein) → cerebral malaria
- No schizont/trophozoite in peripheral blood (sequestered in deep microvasculature)
- Only rings + crescents visible in peripheral smear
Lab Diagnosis:
╔══════════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS OF MALARIA ║
║ ║
║ 1. PERIPHERAL BLOOD SMEAR (GOLD STANDARD) ║
║ ├── Thick film (screening): more concentrated, better for ║
║ │ detecting parasites at low parasitemia ║
║ ├── Thin film (species ID): morphology of ring, RBC size ║
║ └── Stain: Leishman, Giemsa, Wright's stain ║
║ ║
║ COLLECT: During fever/before antipyretics ║
║ (during erythrocytic rupture - max parasitemia) ║
║ ║
║ 2. RAPID DIAGNOSTIC TEST (RDT / ICT) ║
║ ├── Detects HRP-2 antigen (P. falciparum specific) ║
║ ├── pLDH (pan-malarial antigen, all species) ║
║ ├── Aldolase (pan-malarial) ║
║ └── SD Bioline Malaria, Paracheck (India) ║
║ • Sensitivity: >95% for P. falciparum ║
║ • Results in 15-20 minutes ║
║ ║
║ 3. QBC (Quantitative Buffy Coat) ║
║ ├── Capillary tube centrifugation ║
║ ├── Acridine orange stain (fluorescent) ║
║ └── Fluorescent parasites visible at buffy coat ║
║ ║
║ 4. PCR (Molecular) ║
║ ├── Most sensitive (detects <5 parasites/μL) ║
║ ├── Species-specific ║
║ └── Used when smear negative, low parasitemia ║
║ ║
║ 5. SEROLOGY (IFAT, ELISA) ║
║ └── Epidemiological surveys, NOT for acute diagnosis ║
╚══════════════════════════════════════════════════════════════╝
P. falciparum smear features (easy to draw):
THIN FILM - P. falciparum:
╔══════════════════════════════════════════════════════╗
║ RBC NOT ENLARGED ║
║ ║
║ ┌────────┐ ┌────────┐ ┌────────┐ ║
║ │ ○ ○ │ │ ○○ │ │CRESCENT│ ║
║ │(double │ │(double │ │ )))) │ ║
║ │ ring) │ │ infect)│ │GAMETOC.│ ║
║ └────────┘ └────────┘ └────────┘ ║
║ Ring stage Polyinfection Banana-shaped ║
║ gametocyte ║
╚══════════════════════════════════════════════════════╝
Treatment (NVBDCP India Guidelines):
- Artemisinin Combination Therapy (ACT): Artemether-Lumefantrine (AL) OR Artesunate + Sulfadoxine-Pyrimethamine (AS+SP)
- Duration: 3 days
- Add Primaquine 0.75 mg/kg single dose (gametocidal - prevents transmission)
- Artesunate IV/IM (DOC) 2.4 mg/kg at 0, 12, 24 hrs then once daily
- Alternatives: Quinine IV
- Supportive: IV fluids, blood transfusion, anticonvulsants, ICU
- Chloroquine (3 days) + Primaquine 0.25 mg/kg/day x 14 days
- Check G6PD before Primaquine (causes hemolysis in G6PD deficiency)
References: Apurba Shastri's Textbook of Microbiology (as per MUHS); Jawetz, Melnick & Adelberg's Medical Microbiology 28th Ed; Murray's Medical Microbiology 9th Ed; NACO/NVBDCP India Guidelines.
MUHS Exam tip - MUHS 2 marks = Define + 1-2 key points. 3 marks = Diagram + brief notes. 5-8 marks (LAQ) = Definition, Classification, Morphology, Life cycle, Lab Diagnosis, Treatment with clear headings and diagrams.

2mbbs micro refer apurba shastri answer in detail and add colour diagrams easy to draw in exams as required as well cover details of answers
MUHS 2nd MBBS - MICROBIOLOGY - PAPER 2
LAQ SECTION
Q1. 30 y/o - Muscle Twitching, Hypersalivation, Difficulty Drinking Water
i) Diagnosis and Etiological Agent
| Property | Details |
|---|---|
| Family | Rhabdoviridae |
| Genus | Lyssavirus |
| Nucleic acid | Single-stranded, negative-sense RNA |
| Shape | Bullet-shaped (cylindrical with one flat and one rounded end) |
| Size | 180 x 75 nm |
| Envelope | Enveloped virus |
| Proteins | G protein (glycoprotein - surface spikes, induces neutralizing Ab, pathogenicity), N protein (nucleoprotein - forms Negri bodies), L, M, P proteins |
- Muscle twitching = neuromuscular involvement
- Hypersalivation = autonomic dysfunction + inability to swallow
- Difficulty drinking water (Hydrophobia) = pharyngeal/laryngeal spasm on seeing water - PATHOGNOMONIC of furious rabies
ii) Lab Diagnosis
- Ante-mortem: Saliva, CSF, serum, skin biopsy (nape of neck - hair follicles), brain biopsy
- Post-mortem: Brain tissue (hippocampus/cerebellum/brainstem = highest viral concentration)
╔═══════════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS OF RABIES ║
║ ║
║ ANTE-MORTEM: ║
║ 1. DFA (Direct Fluorescent Antibody) on skin biopsy ║
║ - Nape of neck skin biopsy (hair follicle nerve endings) ║
║ - Most sensitive ante-mortem test ║
║ - Bright apple-green fluorescence ║
║ ║
║ 2. RT-PCR (Reverse Transcriptase PCR) ║
║ - From saliva, CSF, skin, brain ║
║ - Highly sensitive, confirms genotype ║
║ ║
║ 3. Virus Isolation ║
║ - Mouse inoculation / cell culture (Neuroblastoma cells) ║
║ - From saliva, CSF ║
║ ║
║ 4. Serology (Antibody detection) ║
║ - RFFIT (Rapid Fluorescent Focus Inhibition Test) ║
║ - MNT (Mouse Neutralization Test) ║
║ - Useful after 7-8 days / in vaccinated individuals ║
║ - In unvaccinated patients: antibody confirms rabies ║
║ ║
║ POST-MORTEM: ║
║ 5. Negri Bodies (Seller's stain / H&E) ║
║ - Eosinophilic intracytoplasmic inclusion bodies ║
║ - In Purkinje cells (cerebellum) and pyramidal cells ║
║ of hippocampus (Ammon's horn) ║
║ - PATHOGNOMONIC of rabies ║
║ - **Seen in the image above (dark inclusions in neurons)**║
║ ║
║ 6. DFA on brain tissue - GOLD STANDARD ║
║ - Most sensitive and specific overall test ║
╚═══════════════════════════════════════════════════════════════╝
iii) DIAGRAM - Rabies Virus Structure (Easy to draw in exams)
╔═══════════════════════════════════════════════════════════════╗
║ RABIES VIRUS - BULLET SHAPE DIAGRAM ║
║ ║
║ ╔══════════════════════════════════╗ ║
║ ║▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓▓║ ← ENVELOPE ║
║ ║ ↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑ ║ ← G-PROTEIN SPIKES ║
║ ║ ══════════════════════════ ║ ← M PROTEIN (matrix) ║
║ ║ ●══════●══════●══════●══════ ║ ← RNP (N-protein ║
║ ║ ●══════●══════●══════● ║ + RNA + L/P prot) ║
║ ║ ══════════════════════════ ║ ║
║ ╚══════════════════════════════╝ ║ ║
║ [FLAT END] [ROUNDED END] ║
║ ║
║ KEY LABELS: ║
║ • ssRNA (negative sense) → core ║
║ • Helical nucleocapsid (N + P + L proteins) ║
║ • Matrix protein (M) → inner envelope layer ║
║ • Glycoprotein (G) spikes → antigenicity, host attachment ║
║ Size: 180 × 75 nm Shape: BULLET/BACILLIFORM ║
╚═══════════════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════╗
║ NEGRI BODY IN NEURON (DRAW THIS) ║
║ ║
║ ┌──────────────────────────────────┐ ║
║ │ NEURON (hippocampal) │ ║
║ │ Nucleus (pale) ○ │ ║
║ │ │ ║
║ │ ● ← NEGRI BODY │ ║
║ │ (eosinophilic, cytoplasmic, │ ║
║ │ oval/spherical inclusion) │ ║
║ │ Contains inner granules │ ║
║ └──────────────────────────────────┘ ║
║ Stain: Seller's stain (pink body, ║
║ purple inner granules) ║
╚══════════════════════════════════════════════╝
iv) Vaccination Scheme
- Pre-exposure Prophylaxis (PrEP) - for high-risk people (veterinarians, lab workers, dog handlers)
- Post-exposure Prophylaxis (PEP) - after suspected exposure
Pre-Exposure Prophylaxis (PrEP):
- HDCV (Human Diploid Cell Vaccine) OR PCECV (Purified Chick Embryo Cell Vaccine)
- Schedule: 0, 7, 28 days (3 doses IM, deltoid) → Booster every 2 years
Post-Exposure Prophylaxis (PEP) - MOST IMPORTANT:
| Category | Wound | Action |
|---|---|---|
| I | Touch/lick on intact skin | Wash only, NO PEP |
| II | Scratches, minor abrasion without bleeding | Wound wash + Vaccine |
| III | Deep bite, bleeding, mucous membrane exposure | Wound wash + Vaccine + RIG |
╔══════════════════════════════════════════════════════════════╗
║ RABIES PEP SCHEDULE (ESSEN 5-DOSE) ║
║ ║
║ Day 0 → Day 3 → Day 7 → Day 14 → Day 28 ║
║ (5 doses of cell culture vaccine - IM deltoid) ║
║ ║
║ IF Category III: Add RIG on Day 0 ONLY ║
║ ├── Human RIG (HRIG): 20 IU/kg (preferred) ║
║ └── Equine RIG (ERIG): 40 IU/kg (if HRIG unavailable) ║
║ → Infiltrate maximum dose at wound site ║
║ → Remaining give IM (distant site from vaccine) ║
║ ║
║ 4-DOSE schedule (Updated Essen): ║
║ Day 0 (2 doses - both deltoids) + Day 7 + Day 21 ║
║ ║
║ WOUND MANAGEMENT (FIRST, MOST IMPORTANT): ║
║ • Wash with soap and water for 10-15 minutes ║
║ • Apply 70% alcohol/povidone-iodine ║
║ • Do NOT suture immediately ║
╚══════════════════════════════════════════════════════════════╝
- PCECV (Rabipur/Verorab) - Intramuscular
- PVRV (Purified Vero Cell Rabies Vaccine)
- ID (Intradermal) protocol: 2-site ID schedule (0.1ml at 2 sites on day 0,3 then 1 site on day 7,28) - economical
Q2. 24 y/o male - Pain on Micturition, Pus Discharge, Contact with Sex Worker
i) Organism
| Property | Details |
|---|---|
| Shape | Gram-negative diplococcus |
| Arrangement | Coffee bean / kidney-shaped cocci in pairs (adjacent sides flattened) |
| Size | 0.6-1.0 μm |
| Capsule | Absent (unlike N. meningitidis) |
| Flagella | Absent but has pili |
| Spore | Absent |
| Intracellular | Found WITHIN PMNs (intracellular gram-negative diplococci = diagnostic) |
- Family: Neisseriaceae
- Gram: Gram-negative
- Oxygen: Aerobe
- Shape: Coccus
- Fastidious: Requires enriched media
ii) Pathogenesis
╔══════════════════════════════════════════════════════════════════╗
║ PATHOGENESIS OF GONORRHOEA ║
║ ║
║ NEISSERIA GONORRHOEAE (infective dose: 100-1000 organisms) ║
║ ↓ [Sexual contact → mucosal surface] ║
║ ATTACHMENT via PILI (Type IV pili = primary adhesin) ║
║ ↓ ║
║ Opa PROTEINS (outer membrane) → tight binding to ║
║ columnar/transitional epithelium ║
║ ↓ ║
║ PENETRATION into subepithelial tissue ║
║ (via endocytosis - transported across epithelial cells) ║
║ ↓ ║
║ INFLAMMATORY RESPONSE: ║
║ PMN influx → intense neutrophilic reaction ║
║ Gonococcal LOS (lipooligosaccharide) → TNF release → damage ║
║ ↓ ║
║ PUS FORMATION (urethral discharge) ║
║ ↓ ║
║ Local spread → ascending infection: ║
║ Male: Epididymitis, Prostatitis, Urethral stricture ║
║ Female: PID, Salpingitis, Bartholin's gland abscess ║
║ Systemic: DGI (Disseminated Gonococcal Infection) ║
║ → Septic arthritis, Skin lesions, Endocarditis ║
╚══════════════════════════════════════════════════════════════════╝
| Virulence factor | Role |
|---|---|
| Pili (Type IV) | Attachment to epithelium; anti-phagocytic; antigenic variation |
| Opa proteins | Tight binding; invasion |
| Por protein (Porin) | Survives inside PMN; intracellular survival |
| LOS (Lipooligosaccharide) | Endotoxin activity; triggers inflammation |
| IgA protease | Cleaves secretory IgA → evades mucosal immunity |
| Beta-lactamase | Penicillin resistance (PPNG strains) |
iii) Lab Diagnosis
╔══════════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS OF GONORRHOEA ║
║ ║
║ 1. GRAM STAIN (MOST IMPORTANT - quick diagnosis) ║
║ - Urethral pus smear ║
║ - Gram-negative diplococci WITHIN PMNs ║
║ - Sensitivity: 90-95% in symptomatic males ║
║ - Less sensitive in females (50-70%) ║
║ ║
║ 2. CULTURE (GOLD STANDARD): ║
║ Media: Modified Thayer-Martin (MTM) medium ║
║ = Chocolate agar + VCN inhibitors: ║
║ Vancomycin (gram +ve), Colistin (gram -ve), ║
║ Nystatin (fungi) + Trimethoprim ║
║ Transport: Stuart's transport medium (if delay) ║
║ Incubate: 35-37°C, 5-10% CO2 atmosphere (candle jar) ║
║ Colonies: Small, grey, translucent, oxidase +ve ║
║ ║
║ 3. BIOCHEMICAL: ║
║ - Oxidase POSITIVE (key test) ║
║ - Ferments GLUCOSE only (not maltose/lactose) ║
║ (N. meningitidis ferments glucose AND maltose) ║
║ - Catalase positive ║
║ ║
║ 4. NUCLEIC ACID AMPLIFICATION TEST (NAAT) - BEST OVERALL: ║
║ - PCR/SDA/TMA on urine or swab ║
║ - Highest sensitivity and specificity ║
║ - Can detect both N. gonorrhoeae AND C. trachomatis ║
║ simultaneously (co-infection common) ║
║ - Does NOT require viable organisms ║
║ ║
║ 5. OXIDASE TEST: ║
║ - Tetramethyl-p-phenylenediamine (reagent) ║
║ - Colonies turn PURPLE = oxidase positive ║
╚══════════════════════════════════════════════════════════════╝
- Ceftriaxone 500mg IM single dose (DOC - due to QRNG - quinolone-resistant N. gonorrhoeae)
- + Azithromycin 1g oral (for co-infection with Chlamydia)
- Neonatal ophthalmia: 1% Silver nitrate drops / Erythromycin eye ointment
iv) DIAGRAM - Gram Stain of Gonorrhoea (Draw in exam)
╔══════════════════════════════════════════════════════════════╗
║ GRAM STAIN DIAGRAM - N. GONORRHOEAE IN PUS ║
║ ║
║ PINK background (gram-negative) ║
║ ║
║ ┌─────────────────────┐ ║
║ │ PMN (pink) │ ║
║ │ Nucleus - lobed │ ║
║ │ @ @ @ │ ║
║ │ ← coffee bean │ ║
║ │ diplococci │ ║
║ │ (INTRACELLULAR) │ ║
║ └─────────────────────┘ ║
║ ║
║ ALSO extracellular diplococci seen ║
║ ║
║ KEY: ║
║ @@ = gram-negative diplococcus (coffee bean shape) ║
║ Flat adjacent sides facing each other ║
║ PINK = gram-negative (safranin) ║
║ Diplococci found WITHIN the cytoplasm of PMNs ║
╚══════════════════════════════════════════════════════════════╝
Q3. 12 days ago - Contact with Sex Worker - Indurated Painless Ulcer
i) Diagnosis
| Property | Details |
|---|---|
| Family | Spirochaetaceae |
| Shape | Tightly coiled spirochete (corkscrew appearance) |
| Size | 0.2 μm wide, 5-15 μm long |
| Coils | 6-14 coils, regularly spaced 1 μm apart |
| Motility | Rotating motion (corkscrew) via endoflagella (periplasmic flagella) |
| Gram stain | Does NOT stain (too thin) |
| Culture | Cannot be cultured on artificial media |
| Staining | Silver impregnation (Warthin-Starry/Fontana stain); Dark-field microscopy |
ii) Clinical Features in Different Stages
╔══════════════════════════════════════════════════════════════════╗
║ STAGES OF SYPHILIS - CLINICAL FEATURES ║
║ ║
║ ┌─────────────────────────────────────────────────────────┐ ║
║ │ PRIMARY SYPHILIS (Week 1-12 after infection): │ ║
║ │ • Single PAINLESS, INDURATED (hard) ulcer = CHANCRE │ ║
║ │ • Site: Glans penis, vulva, vagina, cervix, anus │ ║
║ │ • Non-tender, clean base, raised edges │ ║
║ │ • Regional LYMPHADENOPATHY (painless, firm) │ ║
║ │ • Heals spontaneously in 3-6 weeks │ ║
║ └─────────────────────────────────────────────────────────┘ ║
║ ↓ (if untreated, 4-8 weeks later) ║
║ ┌─────────────────────────────────────────────────────────┐ ║
║ │ SECONDARY SYPHILIS (Weeks 6-8 after chancre heals): │ ║
║ │ • SKIN RASH: maculopapular, INVOLVES PALMS AND SOLES │ ║
║ │ (pathognomonic finding) │ ║
║ │ • Condylomata lata (moist, warty plaques in perineum) │ ║
║ │ • Mucous patches in mouth (HIGHLY INFECTIOUS) │ ║
║ │ • Generalized lymphadenopathy │ ║
║ │ • Alopecia (moth-eaten) │ ║
║ │ • Flu-like symptoms: fever, malaise, headache │ ║
║ │ • Hepatitis, meningitis, uveitis (rare) │ ║
║ └─────────────────────────────────────────────────────────┘ ║
║ ↓ (latent period: 2 years early, >2 years late) ║
║ ┌─────────────────────────────────────────────────────────┐ ║
║ │ LATENT SYPHILIS: │ ║
║ │ • Early latent (<2 years): Asymptomatic, can relapse │ ║
║ │ • Late latent (>2 years): No symptoms, low infectivity │ ║
║ └─────────────────────────────────────────────────────────┘ ║
║ ↓ (years later) ║
║ ┌─────────────────────────────────────────────────────────┐ ║
║ │ TERTIARY/LATE SYPHILIS: │ ║
║ │ • GUMMA (granulomatous lesions): skin, bone, liver │ ║
║ │ • Cardiovascular syphilis: │ ║
║ │ - Aortic aneurysm (ascending aorta) │ ║
║ │ - Aortic regurgitation │ ║
║ │ - Coronary ostial stenosis │ ║
║ │ • Neurosyphilis: │ ║
║ │ - Meningovascular syphilis │ ║
║ │ - General paresis of the insane (GPI) │ ║
║ │ - Tabes dorsalis (posterior column degeneration) │ ║
║ │ - Argyll Robertson pupil (accommodates but doesn't │ ║
║ │ react to light) │ ║
║ └─────────────────────────────────────────────────────────┘ ║
║ ║
║ CONGENITAL SYPHILIS (Transplacental): ║
║ EARLY (<2 years): Snuffles, condylomata, rash, hepato- ║
║ splenomegaly, osteochondritis, pseudoparalysis ║
║ LATE (>2 years): Hutchinson's triad: ║
║ 1. Interstitial keratitis ║
║ 2. 8th nerve deafness ║
║ 3. Hutchinson's teeth (peg-shaped notched incisors) ║
╚══════════════════════════════════════════════════════════════════╝
iii) Lab Diagnosis
╔══════════════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS OF SYPHILIS ║
║ ║
║ A. DIRECT DETECTION (Primary/Secondary - infectious stages): ║
║ ║
║ 1. DARK-FIELD MICROSCOPY (MOST IMPORTANT for primary) ║
║ - Exudate from chancre/condylomata ║
║ - Spirochetes seen as white, corkscrew, rotatory organisms ║
║ - IMMEDIATE examination required ║
║ - Cannot use on oral lesions (commensal treponemes ║
║ may give false positive) ║
║ ║
║ 2. DFA-TP (Direct Fluorescent Antibody for T. pallidum) ║
║ - Fixed smear + fluorescent anti-Tp antibody ║
║ - Can use on oral lesions (species-specific) ║
║ ║
║ 3. PCR - Highly sensitive, from ulcer exudate ║
║ ║
║ B. SEROLOGICAL TESTS: ║
║ ║
║ NON-TREPONEMAL (REAGINIC) TESTS - SCREENING: ║
║ ├── VDRL (Venereal Disease Research Laboratory) ║
║ │ - Cardiolipin-lecithin-cholesterol antigen ║
║ │ - Flocculation test (tubes/slides) ║
║ │ - POSITIVE: clumping = reactive ║
║ │ - Used for: SCREENING + CSF (neurosyphilis) ║
║ └── RPR (Rapid Plasma Reagin) ║
║ - Carbon particles + cardiolipin antigen ║
║ - Can be done on unheated serum (rapid) ║
║ - Preferred for field screening ║
║ ║
║ TREPONEMAL (SPECIFIC) TESTS - CONFIRMATORY: ║
║ ├── TPHA/TPPA (T. pallidum Hemagglutination/Particle ║
║ │ Passive Agglutination) - simple, widely used ║
║ ├── FTA-ABS (Fluorescent Treponemal Antibody-Absorbed) ║
║ │ - GOLD STANDARD, first to become positive, ║
║ │ remains positive lifelong ║
║ ├── ELISA (anti-Tp antibody) ║
║ └── Western Blot (most specific) ║
╚══════════════════════════════════════════════════════════════════╝
| Test | Primary | Secondary | Latent | Tertiary | Treated |
|---|---|---|---|---|---|
| VDRL/RPR | 70% | 99% | 70% | 30% | Becomes -ve |
| FTA-ABS | 85% | 100% | 100% | 98% | Stays +ve |
| TPHA | 65% | 100% | 100% | 95% | Stays +ve |
- SLE, malaria, leprosy, pregnancy, viral infections (EBV, hepatitis), old age
- VDRL on CSF = GOLD STANDARD for neurosyphilis
- Lymphocytic pleocytosis, elevated protein
- Primary/Secondary/Early latent: Benzathine Penicillin G 2.4 MU IM single dose
- Late latent/Tertiary: Benzathine Penicillin G 2.4 MU IM weekly x 3 doses
- Neurosyphilis: Aqueous Penicillin G 18-24 MU/day IV x 10-14 days
- Penicillin allergy: Doxycycline 100mg BD x 14-28 days
iv) Mode of Transmission (MOT)
| Route | Details |
|---|---|
| Sexual contact (most common) | Direct contact with infectious chancre/condylomata/mucous patch |
| Congenital (transplacental) | After 16th week gestation; all stages except late latent can transmit |
| Blood transfusion | Organism viable in blood at 4°C for 24 hours |
| Needlestick injury | Rare |
| Direct inoculation | Laboratory accidents |
| Kissing | If oral mucous patches present |
- Toilet seats, swimming pools, sharing utensils (organism dies rapidly on drying)
SAQ SECTION
SAQ 1: Short Note on TUBERCULIN TEST (Mantoux Test)
Principle:
- Type IV hypersensitivity (Delayed Type Hypersensitivity - DTH)
- Mediated by sensitized T lymphocytes (CD4+ Th1 cells)
- Previous exposure to TB antigens → memory T cells formed
- Re-injection of tuberculin antigen → memory T cells recruited → cytokines released → induration (hard swelling) at injection site
- Induration (not erythema) = measure of positivity
Procedure:
╔══════════════════════════════════════════════════════════════╗
║ MANTOUX TEST PROCEDURE ║
║ ║
║ MATERIAL: 0.1 mL of PPD (Purified Protein Derivative) ║
║ = 5 TU (Tuberculin Units) in India ║
║ ║
║ SITE: Volar surface of left forearm ║
║ ║
║ TECHNIQUE: INTRADERMAL (NOT subcutaneous) ║
║ → Inject using 26-gauge needle ║
║ → Wheal 6-10 mm should appear ║
║ ║
║ READ at: 48-72 hours ║
║ ║
║ MEASURE: Only INDURATION (hard area) with ruler ║
║ NOT redness/erythema ║
╚══════════════════════════════════════════════════════════════╝
Interpretation (Indian guidelines / WHO):
| Reading | Interpretation |
|---|---|
| < 10 mm | Negative (no prior TB exposure; may be unvaccinated or immunocompromised) |
| 10-14 mm | Positive (prior TB exposure OR BCG vaccinated) |
| ≥ 15 mm | Strongly positive (likely TB infection) |
| ≥ 5 mm in HIV/immunocompromised | Considered positive |
| ≥ 5 mm with known contact | Considered positive |
False POSITIVE causes:
- BCG vaccination
- NTM (Non-tuberculous mycobacteria) infection
- Cross-reaction with other Mycobacteria
False NEGATIVE causes (Anergy):
Mnemonic: LIMED-V
L - Lymphoma / leukemia
I - Immunosuppression (HIV, steroids, chemotherapy)
M - Malnutrition
E - Early TB (< 6 weeks)
D - Disseminated TB (miliary - energy state)
V - Viral infections (measles, mumps)
Applications:
- Screening for latent TB infection (LTBI)
- Contact tracing (index case contacts)
- Diagnosis in children (< 5 years, no BCG = strong indicator)
- Epidemiological surveys (prevalence of TB infection)
- Pre-BCG testing in older children (>5 years)
- Evidence of CMI in TB research/teaching
- NOT useful to diagnose active TB (positive only means past exposure)
SAQ 2: Diphtheria Prophylaxis - Rationale and Types
- Disease is caused by exotoxin (not organism itself)
- Antitoxin neutralizes circulating toxin
- Vaccine induces antitoxin antibodies → prevents disease
- Herd immunity needed (>85% coverage eliminates circulation)
- Immunisation with toxoid (formalin-inactivated toxin) is mainstay
Types of Prophylaxis:
╔══════════════════════════════════════════════════════════════════╗
║ DIPHTHERIA PROPHYLAXIS ║
║ ║
║ A. ACTIVE IMMUNIZATION (Long-term, preferred): ║
║ ├── Diphtheria Toxoid (DT/dT component) ║
║ │ - Toxin treated with formalin → TOXOID ║
║ │ - Non-toxic but immunogenic ║
║ │ - Induces antitoxin (IgG) antibodies ║
║ │ - Combined vaccines used: ║
║ │ • DPT (Diphtheria + Pertussis + Tetanus) - children ║
║ │ • Tdap - adolescents/adults (lower dose dT) ║
║ │ ║
║ NATIONAL IMMUNIZATION SCHEDULE (India): ║
║ DPT: 6 weeks, 10 weeks, 14 weeks (primary series) ║
║ 18 months (1st booster) ║
║ 5 years (2nd booster - DT/DPT) ║
║ 10 years + 16 years (dT booster) ║
║ ║
║ B. PASSIVE IMMUNIZATION (Short-term, immediate): ║
║ ├── DAT (Diphtheria Antitoxin) = Antidiphtheritic serum (ADS) ║
║ │ - Equine (horse) antiserum containing anti-diphtheria IgG ║
║ │ - Used for: TREATMENT of clinical diphtheria ║
║ │ - MUST test for horse serum allergy first (ID test) ║
║ │ - Dose: 20,000-1,00,000 units depending on severity ║
║ │ - Given IM or IV ║
║ │ - Neutralizes FREE toxin (not toxin already bound to cells) ║
║ │ ║
║ C. CHEMOPROPHYLAXIS (for close contacts): ║
║ └── Erythromycin 500mg QID x 7 days OR ║
║ Benzathine Penicillin G 1.2 MU IM single dose ║
║ (eradicates carriage) ║
╚══════════════════════════════════════════════════════════════════╝
- Inject 1/50 MLD of diphtheria toxin intradermally
- Positive (susceptible) = red inflamed area at 24-48h (no antitoxin = no protection)
- Negative (immune) = no reaction (antitoxin present)
- Rarely used today (replaced by serology)
SAQ 3: Methods of MRSA Detection and Prevention of Spread
Types:
- HA-MRSA (Hospital-Acquired): Affects hospitalized patients, immunocompromised
- CA-MRSA (Community-Acquired): Affects healthy individuals; Panton-Valentine Leukocidin (PVL) toxin positive
Methods of MRSA Detection:
╔═══════════════════════════════════════════════════════════════╗
║ METHODS OF MRSA DETECTION ║
║ ║
║ 1. CONVENTIONAL CULTURE + SUSCEPTIBILITY: ║
║ a. Culture on ChromoAgar MRSA (chromogenic): ║
║ - MRSA colonies → MAUVE/PINK color ║
║ - Sensitivity ~75-90%, specific ║
║ b. Blood agar → identify S. aureus ║
║ → Disk Diffusion: Oxacillin/Cefoxitin disk (30μg) ║
║ - Zone <22mm (Cefoxitin) = MRSA ║
║ - Cefoxitin is best predictor of mecA gene ║
║ c. MIC (Minimum Inhibitory Concentration): ║
║ - Oxacillin MIC ≥4 μg/mL = MRSA ║
║ ║
║ 2. MOLECULAR METHODS (GOLD STANDARD): ║
║ a. PCR for mecA gene (most definitive) ║
║ b. Real-time PCR (BD GeneOhm, Xpert MRSA) - rapid ║
║ (2-5 hours) from nasal swabs ║
║ c. Results in 2-3 hours - used for active surveillance ║
║ ║
║ 3. LATEX AGGLUTINATION: ║
║ - Detects PBP2a (mecA gene product) ║
║ - e.g. MRSA Screen test (Denka Seiken) ║
║ - Quick, cheap, easy to perform ║
║ ║
║ 4. ANTI-PBP2a IMMUNOASSAY: ║
║ - Lateral flow assay or ELISA for PBP2a protein ║
║ - From colonies after 6-hour enrichment ║
╚═══════════════════════════════════════════════════════════════╝
Recommendations to Prevent MRSA Spread (Infection Control):
PREVENTION STRATEGIES:
STANDARD PRECAUTIONS (ALL patients):
• Hand hygiene (WHO 6 steps) - MOST IMPORTANT
• PPE (gloves, gown) when handling body fluids
• Safe sharps disposal
CONTACT PRECAUTIONS (MRSA patients):
• ISOLATE patient in single room (or cohort MRSA patients)
• Gloves + gown for ALL contact
• Dedicated equipment (stethoscope, BP cuff)
• Decolonization:
- Mupirocin 2% nasal ointment BD x 5 days
- Chlorhexidine 2-4% whole body wash x 5 days
- Screen household contacts
ACTIVE SURVEILLANCE CULTURES (ASC):
• Screen all ICU admissions (nasal + rectal swab)
• Identify MRSA carriers → isolate/decolonize
ANTIMICROBIAL STEWARDSHIP:
• Restrict broad-spectrum antibiotics
• Rotate antibiotics in ICU
• Remove unnecessary catheters/lines
TREATMENT of MRSA infections:
• Vancomycin IV (DOC for serious HA-MRSA)
• Linezolid (oral/IV; skin and soft tissue)
• Daptomycin (bacteremia, endocarditis)
• Trimethoprim-Sulfa (CA-MRSA skin infections)
SAQ 4: Serological Markers in Hepatitis B Infection
- DNA virus, Hepadnaviridae family
- Antigens: HBsAg, HBcAg, HBeAg (important serological markers)
DIAGRAM - HBV Structure:
╔═══════════════════════════════════════════════════════╗
║ HBV PARTICLE (DANE PARTICLE) DIAGRAM ║
║ ║
║ OUTER ENVELOPE: ●●●●●●●●● ← HBsAg ║
║ INNER CORE: ████████ ← HBcAg (internal) ║
║ Within core: ════════ ← HBeAg (soluble) ║
║ | | ║
║ dsDNA + DNA polymerase ║
╚═══════════════════════════════════════════════════════╝
Serological Markers Table (MOST IMPORTANT - must memorise):
╔══════════════════════════════════════════════════════════════════════════╗
║ HBV SEROLOGICAL MARKERS - INTERPRETATION ║
╠═══════════════╦═══════╦═══════╦═══════╦════════╦════════╦═══════════════╣
║ STATUS ║HBsAg ║Anti- ║HBeAg ║Anti- ║Anti- ║ HBV DNA ║
║ ║ ║HBs ║ ║HBe ║HBc ║ ║
╠═══════════════╬═══════╬═══════╬═══════╬════════╬════════╬═══════════════╣
║ Susceptible ║ - ║ - ║ - ║ - ║ - ║ - ║
╠═══════════════╬═══════╬═══════╬═══════╬════════╬════════╬═══════════════╣
║ Acute HBV ║ + ║ - ║ + ║ - ║IgM+ve ║ High ║
╠═══════════════╬═══════╬═══════╬═══════╬════════╬════════╬═══════════════╣
║ Chronic HBV ║ + ║ - ║ +/- ║ +/- ║IgG+ve ║ +/- ║
║ (High replic) ║ + ║ - ║ + ║ - ║IgG+ve ║ High ║
║ (Low replic) ║ + ║ - ║ - ║ + ║IgG+ve ║ Low/undetect ║
╠═══════════════╬═══════╬═══════╬═══════╬════════╬════════╬═══════════════╣
║ Window period ║ - ║ - ║ - ║ - ║IgM+ve ║ + ║
║ (acute phase) ║ ║ ║ ║ ║(ONLY+) ║ ║
╠═══════════════╬═══════╬═══════╬═══════╬════════╬════════╬═══════════════╣
║ Past infection║ - ║ + ║ - ║ +/- ║IgG+ve ║ - ║
║ (resolved) ║ ║ ║ ║ ║ ║ ║
╠═══════════════╬═══════╬═══════╬═══════╬════════╬════════╬═══════════════╣
║ Vaccinated ║ - ║ + ║ - ║ - ║ - ║ - ║
║ (only anti-HBs positive; no anti-HBc = NOT naturally infected) ║
╚══════════════════════════════════════════════════════════════════════════╝
Individual Marker Significance:
| Marker | Significance |
|---|---|
| HBsAg | Active HBV infection (acute or chronic); first marker to appear; persist >6 months = chronic |
| Anti-HBs | Immunity (past infection OR vaccination); protective |
| HBcAg | Not found in serum (intracellular only) |
| Anti-HBc IgM | Acute/recent infection; sole marker in window period |
| Anti-HBc IgG | Past infection; persists lifelong |
| HBeAg | High viral replication, HIGH INFECTIVITY; positive = patient infectious |
| Anti-HBe | Low replication; seroconversion = good prognosis |
| HBV DNA | Gold standard for replication; guides treatment; viral load monitoring |
- HBsAg disappears, Anti-HBs not yet formed
- Anti-HBc IgM is the ONLY positive marker - sole evidence of infection
- Important in blood bank screening (NAT used to cover window period)
- Anti-HBs titre >10 IU/mL = seroprotected/immune
SAQ 5: 4 Viruses Responsible for Carcinoma + HSV-2
Oncogenic Viruses (Tumour Viruses):
╔══════════════════════════════════════════════════════════════════╗
║ 4 VIRUSES RESPONSIBLE FOR CARCINOMA ║
║ ║
║ 1. HPV (Human Papillomavirus) ║
║ Type: DNA virus; double-stranded ║
║ Family: Papillomaviridae ║
║ Tumours: ║
║ • Cervical carcinoma (HPV 16, 18 = 70% of cases) ║
║ • Anal, vulvar, vaginal, penile carcinoma ║
║ • Oropharyngeal cancer (HPV 16) ║
║ Mechanism: E6 protein → degrades p53 (tumour suppressor) ║
║ E7 protein → binds Rb protein → uncontrolled ║
║ cell cycle ║
║ ║
║ 2. EBV (Epstein-Barr Virus) ║
║ Type: DNA virus (Herpesvirus) ║
║ Tumours: ║
║ • Burkitt's lymphoma (African jaw tumour - EBV + malaria) ║
║ • Nasopharyngeal carcinoma ║
║ • Hodgkin's lymphoma ║
║ • Post-transplant lymphoma ║
║ Mechanism: Immortalizes B cells; expresses LMP-1 (NF-kB ║
║ activation); EBNA (nuclear antigen) ║
║ ║
║ 3. HBV (Hepatitis B Virus) ║
║ Type: DNA virus (Hepadnaviridae) ║
║ Tumour: Hepatocellular carcinoma (HCC) ║
║ Risk: Chronic HBV → cirrhosis → HCC ║
║ Also: HCV → HCC ║
║ Mechanism: HBx protein → p53 inactivation; insertional ║
║ mutagenesis; chronic inflammation ║
║ ║
║ 4. HTLV-1 (Human T-cell Lymphotropic Virus Type 1) ║
║ Type: RNA virus (Retrovirus) ║
║ Tumour: Adult T-cell Leukemia/Lymphoma (ATL) ║
║ Endemic: Japan, Caribbean, Africa ║
║ Also: HTLV-1 Associated Myelopathy (HAM/TSP) ║
║ Mechanism: Tax protein → activates NF-kB; IL-2 receptor; ║
║ polyclonal T-cell expansion → clonal malignancy ║
╚══════════════════════════════════════════════════════════════════╝
Additional oncogenic viruses (if asked in exam):
- KSHV/HHV-8 → Kaposi's sarcoma (common in AIDS)
- MCPyV (Merkel Cell Polyomavirus) → Merkel cell carcinoma
- HCV → Hepatocellular carcinoma
HSV-2 and Carcinoma:
| Property | HSV-2 |
|---|---|
| Type | dsDNA virus, Herpesviridae |
| Primary site | Genital mucosa |
| Latency | Sacral dorsal root ganglia (S2-S5) |
| Transmission | Sexual contact, vertical (birth) |
- Primary: Painful vesicles/ulcers on genitalia, fever, inguinal lymphadenopathy
- Recurrent: Milder, prodrome of tingling/burning
- Neonatal: Via infected birth canal → severe disseminated/CNS disease
- Cervical carcinoma: HSV-2 was formerly considered causative; currently thought to act as a co-factor alongside HPV (promotes HPV oncogenesis)
- HSV-2 seropositivity is associated with increased cervical cancer risk
- Not directly oncogenic like HPV but enhances malignant transformation
- Tzanck smear: Multinucleated giant cells with intranuclear inclusions (Cowdry type A)
- PCR from vesicle fluid (most sensitive)
- Viral culture (gold standard)
- Serology (IgM/IgG ELISA - type specific)
SAQ 6: Short Note on Zoonotic Diseases
╔══════════════════════════════════════════════════════════════════╗
║ CLASSIFICATION OF ZOONOSES ║
║ ║
║ 1. DIRECT ZOONOSES (Simple host cycle): ║
║ One vertebrate + man ║
║ Ex: Rabies (dog→man), Brucellosis, Leptospirosis ║
║ ║
║ 2. CYCLOZOONOSES (Multiple vertebrate hosts): ║
║ Require >1 vertebrate host ║
║ Ex: Taenia solium (pig→man), Echinococcosis (sheep→man) ║
║ ║
║ 3. METAZOONOSES (Arthropod vector required): ║
║ Vertebrate → Arthropod vector → Man ║
║ Ex: Malaria, Dengue, Plague, Rickettsial diseases ║
║ Yellow fever, Japanese encephalitis, Scrub typhus ║
║ ║
║ 4. SAPROZOONOSES (Abiotic reservoir): ║
║ Soil/plant + vertebrate + man ║
║ Ex: Histoplasmosis (soil/bird droppings), Aspergillosis ║
╚══════════════════════════════════════════════════════════════════╝
Important Zoonoses (MUHS High Yield Table):
| Disease | Agent | Animal Reservoir | Mode of Transmission |
|---|---|---|---|
| Rabies | Rhabdovirus | Dogs, bats, jackals | Bite |
| Brucellosis | Brucella spp. | Cattle, goats, pigs | Milk, contact with placentae |
| Leptospirosis | Leptospira | Rats, cattle, dogs | Contact with urine-contaminated water |
| Plague | Y. pestis | Rats | Flea bite (Xenopsylla cheopis) |
| Q fever | C. burnetii | Cattle, sheep | Inhalation of aerosols |
| Scrub Typhus | O. tsutsugamushi | Rodents | Chigger mite bite |
| Anthrax | B. anthracis | Cattle, sheep | Contact, inhalation, ingestion |
| Salmonellosis | Salmonella | Poultry, cattle | Contaminated food |
| Taeniasis | Taenia solium | Pigs | Undercooked pork |
| Toxoplasmosis | T. gondii | Cats | Contact with cat feces, undercooked meat |
| Cryptococcosis | C. neoformans | Pigeons (not reservoir) | Inhalation of contaminated soil |
| Histoplasmosis | H. capsulatum | Birds, bats | Inhalation of soil/droppings |
Examples of Emerging Zoonoses (Important for exams):
- SARS-CoV-2: Bats (origin), zoonotic spillover
- Nipah: Bats → Pigs → Humans
- MERS-CoV: Camels → Humans
- Ebola: Bats/fruit bats → Primates → Humans
- Monkeypox: Rodents, non-human primates
Public Health Significance:
- Zoonoses account for ~60% of all emerging infectious diseases
- Control requires One Health approach (human + animal + environment health integrated)
- Surveillance of animal populations, vector control, vaccination (rabies), food safety
References: Apurba Shastri's Textbook of Microbiology; Jawetz Melnick & Adelberg's Medical Microbiology 28th Ed; Murray Medical Microbiology 9e; Bradley & Daroff's Neurology; WHO Rabies Post-Exposure Prophylaxis Guidelines.
MUHS Exam Tip: For STI questions (Gonorrhoea/Syphilis) - always begin with morphology, then pathogenesis, then lab diagnosis with table. For Rabies - always include Negri bodies and PEP schedule. For Hepatitis B - the serological markers table is the highest-yield single topic in virology - memorise it completely.
7]short note on zoonotic disease 8]classify enterovirus, detail about polio vaccines 9] note On Ocular fungal infection 10]Define & classory hosp. arogard Infection, desende any 1In detall 11]C/F of toxoplasma encephalitis 2 Lab Diagnosis 12) list organism responsible for LRTI, Lab d of pneumococcamonia 13]SN on Non gonococcal urethritis 14]Enumerare any 4 org. causing UTI write in detail about specimen collection in care of UTI 15]Note on cutaneous Larva migrans 16) Lab d of gas gangrene infection details 17) Diff between HSV-1and HSV-2 18brief PCP preumonia in HIV individuals 19)enumerare dermatophyte infectin& lab D 20) outline pathogenesis & diagnosis of Neurocysticercosis clinical feature, CNS diagnostic tools 21) lab D of Bacterial UTI 22) well label diagram of Rabies virus; PEP 23define precipitation and mention application with example 2mbbs micro refer apurba shastri answer in detail and add colour diagrams easy to draw in exams as required as well cover details of answers
MUHS 2nd MBBS - MICROBIOLOGY - EXTENDED QUESTION BANK
Q7. SHORT NOTE ON ZOONOTIC DISEASES
- Definition: Infections naturally transmissible from vertebrate animals to humans
- Types: Direct, Cyclo-, Meta-, Saprozoonoses
- Key examples: Rabies (dog), Leptospirosis (rat), Plague (rat→flea→man), Brucellosis (cattle), Toxoplasmosis (cat), Scrub typhus (rodents→chigger)
- One Health concept - integrated human-animal-environment health approach
Q8. CLASSIFY ENTEROVIRUS; DETAIL ABOUT POLIO VACCINES
Classification of Enteroviruses:
╔══════════════════════════════════════════════════════════════════╗
║ CLASSIFICATION OF ENTEROVIRUS ║
║ Family: Picornaviridae (Pico = small; RNA = RNA genome) ║
║ Genus: Enterovirus ║
║ ║
║ SUBGROUPS: ║
║ ┌──────────────────────────────────────────────────────┐ ║
║ │ 1. POLIOVIRUS (Types 1, 2, 3) │ ║
║ │ Type 1 = Brunhilde = most epidemic │ ║
║ │ Type 2 = Lansing = eradicated 2015 │ ║
║ │ Type 3 = Leon │ ║
║ │ │ ║
║ │ 2. COXSACKIEVIRUS │ ║
║ │ Group A (23 serotypes): Hand, Foot & Mouth (A16) │ ║
║ │ Herpangina, Aseptic meningitis │ ║
║ │ Group B (6 serotypes): Myocarditis, Pleurodynia, │ ║
║ │ Bornholm disease, Meningoencephalitis │ ║
║ │ │ ║
║ │ 3. ECHOVIRUS (31 serotypes) │ ║
║ │ Aseptic meningitis, respiratory infections, │ ║
║ │ diarrhea in infants │ ║
║ │ │ ║
║ │ 4. ENTEROVIRUS (numbered serotypes) │ ║
║ │ EV-70: Acute hemorrhagic conjunctivitis │ ║
║ │ EV-71: Hand-foot-mouth disease (severe CNS form) │ ║
║ │ EV-68: Acute flaccid myelitis (AFP) │ ║
║ └──────────────────────────────────────────────────────┘ ║
║ ║
║ PROPERTIES (common to all): ║
║ • Single-stranded, positive-sense RNA ║
║ • Non-enveloped, icosahedral capsid ║
║ • Small (25-30 nm) ║
║ • Resistant to ether, acid, detergents ║
║ • Habitat: Intestinal tract → name "Entero"virus ║
╚══════════════════════════════════════════════════════════════════╝
POLIOVIRUS - DETAIL:
╔══════════════════════════════════════════════════════════════╗
║ PATHOGENESIS OF POLIOMYELITIS ║
║ ║
║ INGESTION of virus (feco-oral route) ║
║ ↓ ║
║ Oropharynx → tonsils + Peyer's patches (M cells) ║
║ ↓ Primary viremia ║
║ Blood (minor viremia) → Reticuloendothelial system ║
║ ↓ (in ~1% cases) ║
║ MAJOR VIREMIA → CNS invasion ║
║ ↓ via blood-brain barrier ║
║ MOTOR NEURONS (anterior horn cells) of spinal cord ║
║ ↓ viral replication → cell death ║
║ FLACCID PARALYSIS (Lower Motor Neuron type) ║
║ ║
║ Outcomes (infection pyramid): ║
║ • 90-95%: Subclinical (no symptoms) ║
║ • 4-8%: Abortive polio (minor illness - fever, malaise) ║
║ • 1-2%: Non-paralytic (aseptic meningitis) ║
║ • 0.1-1%: Paralytic polio (flaccid paralysis) ║
╚══════════════════════════════════════════════════════════════╝
POLIO VACCINES (HIGH YIELD COMPARISON):
╔══════════════════════════════════════════════════════════════════════╗
║ OPV vs IPV - COMPARISON TABLE ║
╠═════════════════════════╦═════════════════╦════════════════════════╣
║ Feature ║ OPV (Sabin) ║ IPV (Salk) ║
╠═════════════════════════╬═════════════════╬════════════════════════╣
║ Type ║ Live attenuated ║ Killed/inactivated ║
║ Route ║ Oral (drops) ║ Intramuscular injection ║
║ Dose ║ 2 drops ║ 0.5 ml IM ║
║ Immunity ║ Humoral + mucosal║ Humoral only ║
║ ║ (IgA in gut) ║ (no mucosal IgA) ║
║ Herd immunity ║ EXCELLENT ║ Poor ║
║ ║ (virus shed in ║ ║
║ ║ stool → spreads) ║ ║
║ VAPP risk ║ YES (1:750,000) ║ NO (killed virus) ║
║ cVDPV risk ║ YES ║ NO ║
║ Cold chain ║ Strict (-20°C) ║ Less strict (+4°C) ║
║ Cost ║ Cheap ║ Expensive ║
║ WHO preference ║ Eradication prog ║ High-income countries ║
╚═════════════════════════╩═════════════════╩════════════════════════╝
- tOPV (trivalent): Types 1+2+3 - used till 2016
- bOPV (bivalent): Types 1+3 - currently used (type 2 eradicated in 2015)
- mOPV (monovalent): Single type - outbreak response
- Risk: 1 per 2.4 million doses
- Usually type 3 OPV strain reverts to neurovirulence
- Higher risk in: first dose recipients, immunocompromised
India's Polio Immunization Schedule:
NATIONAL IMMUNIZATION PROGRAMME (India):
At Birth: OPV (birth dose)
6 weeks: IPV 1 + OPV 1 (fractional IPV 0.1ml ID)
10 weeks: OPV 2
14 weeks: IPV 2 + OPV 3 (fIPV 0.1ml ID)
Pulse Polio: Annual January/February NIDs (National Immunization Days)
- fIPV (fractional dose intradermally 0.1ml) added to reduce cost
- Provides systemic immunity without mucosal immunity
- India: Polio-free since January 2011 (last case Jan 2011, certified 2014)
- Global: Types 2 and 3 wild poliovirus eradicated; Type 1 persists in Pakistan/Afghanistan
Q9. NOTE ON OCULAR FUNGAL INFECTION
Classification by site:
╔══════════════════════════════════════════════════════════════════╗
║ OCULAR FUNGAL INFECTIONS ║
║ ║
║ A. FUNGAL KERATITIS (Mycotic keratitis): ║
║ MOST COMMON ocular fungal infection ║
║ Organisms: ║
║ ├── FILAMENTOUS fungi (tropical regions, India): ║
║ │ • Fusarium solani (most common worldwide) ║
║ │ • Aspergillus fumigatus ║
║ │ • Curvularia, Alternaria (dematiaceous) ║
║ └── YEAST (temperate, immunocompromised): ║
║ • Candida albicans ║
║ ║
║ B. ENDOPHTHALMITIS: ║
║ Candida (most common - via blood, IV drug users) ║
║ Aspergillus (trauma/surgery) ║
║ ║
║ C. ORBITAL CELLULITIS / RHINOCEREBRAL: ║
║ Mucor/Rhizopus (Mucormycosis) - diabetics, ketoacidosis ║
║ ║
║ D. CONJUNCTIVITIS: Candida, Aspergillus (rare) ║
╚══════════════════════════════════════════════════════════════════╝
Risk Factors:
- Corneal trauma (vegetative matter - thorn, leaf - Fusarium)
- Contact lens wear
- Previous corneal surgery
- Topical steroid use
- Immunocompromise (Candida, Aspergillus)
- Diabetes (Mucormycosis)
Clinical Features of Fungal Keratitis:
- Corneal ulcer with feathery/satellite lesions (filamentous)
- Dry, raised, grey-white infiltrate
- Hypopyon (pus in anterior chamber)
- Slow progression (unlike bacterial keratitis)
- Poor response to antibacterial therapy
Lab Diagnosis:
SPECIMEN: Corneal scraping (from base and edges of ulcer)
by slit-lamp under sterile conditions
1. DIRECT MICROSCOPY:
├── KOH mount (10-20%): Branching hyphae or yeast cells
├── Gram stain: Gram +ve fungal elements
├── Giemsa stain: Good for Candida
├── Calcoflour white (fluorescent): Most sensitive
└── H&E on biopsy specimen
2. CULTURE:
├── SDA (Sabouraud's Dextrose Agar) at 25°C and 37°C
├── BHI agar
├── Report: Colony morphology, colour, rate of growth
└── LPCB (Lactophenol Cotton Blue) for microscopic ID
3. CONFOCAL MICROSCOPY (in vivo):
- Non-invasive; detects hyphae in living cornea
- Increasingly used in India
4. PCR: From corneal scraping - highly specific
- Natamycin 5% eye drops (DOC for filamentous fungi - Fusarium, Aspergillus)
- Voriconazole (topical/systemic) - broad spectrum
- Fluconazole (Candida keratitis)
- Amphotericin B (severe/Candida)
- Mucormycosis: Urgent surgical debridement + Liposomal Amphotericin B IV
Q10. DEFINE AND CLASSIFY HOSPITAL-ACQUIRED INFECTION (HAI); DESCRIBE ONE IN DETAIL
Definition:
Classification:
╔══════════════════════════════════════════════════════════════════╗
║ CLASSIFICATION OF NOSOCOMIAL INFECTIONS ║
║ ║
║ BY SITE: ║
║ 1. CAUTI - Catheter-Associated Urinary Tract Infection (31%) ║
║ 2. SSI - Surgical Site Infection (20%) ║
║ 3. VAP - Ventilator-Associated Pneumonia (15%) ║
║ 4. CLABSI - Central Line-Associated Bloodstream Infection (14%) ║
║ 5. C. difficile Infection (CDI) (8%) ║
║ ║
║ BY SOURCE: ║
║ • Endogenous: Patient's own flora (most common) ║
║ • Exogenous: Environment, staff, equipment ║
║ ║
║ BY ORGANISMS (ESKAPE pathogens): ║
║ E - Enterococcus faecium (VRE) ║
║ S - Staphylococcus aureus (MRSA) ║
║ K - Klebsiella pneumoniae (ESBL, carbapenem-resistant) ║
║ A - Acinetobacter baumannii (MDR) ║
║ P - Pseudomonas aeruginosa (MDR) ║
║ E - Enterobacter species ║
╚══════════════════════════════════════════════════════════════════╝
CAUTI - Catheter-Associated UTI (IN DETAIL):
- Most common HAI worldwide (31% of all HAIs)
- Risk: 3-7% per catheter-day
- Accounts for 80% of hospital-acquired UTIs
| Organism | Notes |
|---|---|
| E. coli | Most common overall |
| Candida spp. | More common in CAUTI than community UTI |
| Enterococcus | Especially VRE |
| Klebsiella pneumoniae | Often ESBL-producing |
| Pseudomonas aeruginosa | Biofilm former |
| Staphylococcus epidermidis | Biofilm on catheter |
╔════════════════════════════════════════════════════════╗
║ CAUTI PATHOGENESIS ║
║ ║
║ EXTRALUMINAL route (most common): ║
║ Organisms from perineum → colonize external surface ║
║ of catheter → migrate up to bladder ║
║ ║
║ INTRALUMINAL route: ║
║ Contamination of catheter junction or drainage bag ║
║ → travel through lumen into bladder ║
║ ║
║ BIOFILM formation on catheter surface: ║
║ Organisms → attach → produce exopolysaccharide ║
║ → BIOFILM (resistant to antibiotics + immune system) ║
║ → Continuous source of infection ║
╚════════════════════════════════════════════════════════╝
- Often asymptomatic bacteriuria (ASB) - most common
- Symptomatic: Fever, suprapubic pain, cloudy/foul-smelling urine
- Severe: Pyelonephritis, bacteremia, sepsis
- Urine sample: Catheter specimen urine (not from bag)
- Dipstick: Nitrite positive (gram-negative), Leukocyte esterase positive
- Microscopy: >10 WBC/hpf, bacteria on Gram stain
- Culture: >10³ CFU/mL from catheter specimen (lower threshold than non-catheterized)
- Urine culture on CLED/MacConkey
- Insert catheter only when indicated (most important)
- Remove catheter as soon as possible (daily review)
- Strict aseptic technique during insertion
- Maintain closed drainage system
- Maintain urine flow (catheter below bladder level)
- Hand hygiene before/after catheter care
- Avoid routine antimicrobial prophylaxis
Q11. CLINICAL FEATURES OF TOXOPLASMA ENCEPHALITIS AND LAB DIAGNOSIS
- Obligate intracellular protozoan
- Definitive host: Cat (sexual cycle)
- Intermediate hosts: Humans, rodents, birds
Clinical Features of Toxoplasma Encephalitis (mainly in AIDS/immunocompromised):
╔══════════════════════════════════════════════════════════════════╗
║ CLINICAL FEATURES OF TOXOPLASMA ENCEPHALITIS ║
║ ║
║ OCCURS MAINLY IN: AIDS patients (CD4 < 100 cells/μL) ║
║ Mechanism: REACTIVATION of latent cysts (bradyzoites) ║
║ ║
║ SUBACUTE ONSET (over days-weeks): ║
║ ├── HEADACHE (most common symptom) ║
║ ├── FEVER (low-grade) ║
║ ├── FOCAL NEUROLOGICAL DEFICITS: ║
║ │ • Hemiparesis (most common focal sign) ║
║ │ • Aphasia ║
║ │ • Cerebellar ataxia ║
║ │ • Cranial nerve palsies ║
║ │ • Visual field defects ║
║ ├── SEIZURES (30% of cases) ║
║ ├── Confusion, altered mental status ║
║ └── Raised ICP: Papilledema, vomiting ║
║ ║
║ OCULAR TOXOPLASMOSIS (congenital OR reactivation): ║
║ • Chorioretinitis (most common ocular manifestation) ║
║ • Blurred vision, floaters, scotoma ║
║ ║
║ CONGENITAL TOXOPLASMOSIS: ║
║ Classic triad: ║
║ 1. Hydrocephalus ║
║ 2. Chorioretinitis ║
║ 3. Intracranial calcifications (periventricular) ║
╚══════════════════════════════════════════════════════════════════╝
Lab Diagnosis of Toxoplasma Encephalitis:
- MRI (preferred): Multiple ring-enhancing lesions (with surrounding edema), typically at basal ganglia, thalamus, corticomedullary junction
- CT with contrast: Multiple hypodense lesions with ring enhancement ("target lesion" = central dot + ring = highly suggestive but not pathognomonic)
- Location: Basal ganglia (>70%), corticomedullary junction
- Lymphocytic pleocytosis (mild, 10-50 cells)
- Elevated protein
- Normal glucose
- T. gondii PCR from CSF: Sensitivity 50-60%, Specificity >95% - useful when positive
- Culture: Not routine (complex, dangerous)
- Anti-Toxoplasma IgG: >90% of AIDS patients with TE are seropositive
- Negative IgG → makes TE LESS likely (though not excluded)
- IgM: Usually negative in reactivation (not helpful in AIDS/TE)
- Rising IgG titres suggest acute primary infection
- Blood, CSF, BAL, tissue - highly specific
- Low sensitivity in CNS (50-60%) but confirms when positive
- Stereotactic biopsy
- H&E: Shows Toxoplasma tachyzoites (crescent/banana-shaped)
- IHC (immunohistochemistry): Confirms organism
- Only done when empirical treatment fails (10-14 days trial)
- Start Pyrimethamine + Sulfadiazine + Leucovorin
- If clinical + radiological improvement in 10-14 days → confirms TE
- Most centres diagnose by combination of serology + MRI + response to therapy
- Acute: Pyrimethamine 200mg loading then 50mg/day + Sulfadiazine 4-6g/day + Leucovorin 10-25mg/day x 6 weeks
- Maintenance (life-long if CD4 remains <200): Half-dose continuation
- Alternative: Pyrimethamine + Clindamycin (sulfa allergy)
- Prophylaxis: Cotrimoxazole (TMP-SMX) DS once daily when CD4 <100
Q12. ORGANISMS RESPONSIBLE FOR LRTI; LAB DIAGNOSIS OF PNEUMOCOCCAL PNEUMONIA
Organisms Causing LRTI (Lower Respiratory Tract Infection):
╔══════════════════════════════════════════════════════════════════╗
║ ORGANISMS CAUSING LRTI ║
║ ║
║ BRONCHITIS (Acute): ║
║ • Viral (most common): Rhinovirus, Influenza, RSV, Adenovirus ║
║ • Bacterial: S. pneumoniae, H. influenzae, M. catarrhalis ║
║ ║
║ COMMUNITY ACQUIRED PNEUMONIA (CAP): ║
║ Typical: ║
║ • Streptococcus pneumoniae (most common - "classical lobar") ║
║ • Haemophilus influenzae (type b, elderly/COPD) ║
║ • Klebsiella pneumoniae (alcoholics, "currant jelly" sputum) ║
║ • Staphylococcus aureus (post-influenza) ║
║ Atypical ("walking pneumonia"): ║
║ • Mycoplasma pneumoniae (young adults, most common atypical) ║
║ • Chlamydophila pneumoniae ║
║ • Legionella pneumophila (Legionnaires' disease) ║
║ Viral: Influenza, SARS-CoV-2 ║
║ ║
║ HOSPITAL ACQUIRED PNEUMONIA (HAP/VAP): ║
║ • Pseudomonas aeruginosa (most common in ICU) ║
║ • Acinetobacter baumannii (MDR, VAP) ║
║ • Klebsiella pneumoniae (ESBL) ║
║ • MRSA ║
║ ║
║ IMMUNOCOMPROMISED / AIDS: ║
║ • PCP (Pneumocystis jirovecii) ║
║ • Aspergillus (invasive pulmonary aspergillosis) ║
║ • CMV pneumonitis ║
║ • Cryptococcus ║
║ • TB / MAC ║
╚══════════════════════════════════════════════════════════════════╝
Lab Diagnosis of PNEUMOCOCCAL PNEUMONIA:
SPECIMEN: Sputum (Gough first-morning deep cough), BAL,
blood (blood culture), pleural fluid, urine (antigen)
╔══════════════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS OF PNEUMOCOCCAL PNEUMONIA ║
║ ║
║ 1. SPUTUM GRAM STAIN: ║
║ • Lancet-shaped gram-POSITIVE diplococci ║
║ • Surrounded by HALO (capsule - not stained) ║
║ • Many PMNs (neutrophils) ║
║ • Mucoid background ║
║ • Quality check: Bartlett's score / Murray-Washington: ║
║ - <10 squamous cells + >25 PMNs/lpf = good sample ║
║ ║
║ 2. CULTURE (GOLD STANDARD): ║
║ • Blood agar: α-hemolytic (green/partial hemolysis) ║
║ • Colonies: Draughtsman/coin-like (umbilicated - central pit) ║
║ • CO2 atmosphere (5-10%), 35-37°C ║
║ • Blood culture: 2 sets - positive in 30-40% bacteremic cases║
║ ║
║ 3. BIOCHEMICAL IDENTIFICATION: ║
║ • Optochin (Ethylhydrocupreine) sensitivity: Zone ≥14mm ║
║ = S. pneumoniae POSITIVE (viridans streptococci = resistant)║
║ • Bile solubility test: Colonies dissolve in 2% sodium ║
║ deoxycholate = POSITIVE (specific for S. pneumoniae) ║
║ • Inulin fermentation: Positive ║
║ ║
║ 4. QUELLUNG REACTION (NEUFELD'S TEST): ║
║ • Mix sputum + type-specific anticapsular antibody + ║
║ Methylene blue ║
║ • Capsule SWELLS (appears to enlarge) = POSITIVE ║
║ • GOLD STANDARD for serotyping (84 capsular serotypes) ║
║ ║
║ 5. URINE ANTIGEN TEST (BINAXNOW): ║
║ • Detects C-polysaccharide (cell wall antigen) in urine ║
║ • Sensitivity 70-90%, Specificity 90-97% ║
║ • Rapid (15 min), useful even after antibiotics started ║
║ ║
║ 6. SEROLOGY: ║
║ • Anti-pneumococcal antibodies (not routinely used) ║
║ ║
║ 7. PCR: From sputum/blood - most sensitive ║
╚══════════════════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════════════╗
║ S. PNEUMONIAE - GRAM STAIN ║
║ ║
║ Purple (Gram +ve) background ║
║ ║
║ ⟨⟩ ⟨⟩ ⟨⟩ ← Lancet-shaped ║
║ ⟨⟩ ← diplococci in pairs ║
║ [ HALO ] ← capsule (clear space) ║
║ [ PMN @ ] ← neutrophils with bacteria ║
║ ║
║ PURPLE, LANCET-SHAPED DIPLOCOCCUS + CAPSULAR HALO ║
╚══════════════════════════════════════════════════════╝
Q13. SHORT NOTE ON NON-GONOCOCCAL URETHRITIS (NGU)
Causes:
╔════════════════════════════════════════════════════════════╗
║ CAUSES OF NON-GONOCOCCAL URETHRITIS ║
║ ║
║ 1. Chlamydia trachomatis (30-50%) - MOST COMMON ║
║ Serovars D-K (genital serovars) ║
║ ║
║ 2. Ureaplasma urealyticum (10-20%) ║
║ Hydrolyses urea; sensitive to tetracyclines ║
║ ║
║ 3. Mycoplasma genitalium (10-25%) ║
║ Emerging important cause; resistant to azithromycin ║
║ ║
║ 4. Trichomonas vaginalis (5-10%) ║
║ Flagellate protozoan ║
║ ║
║ 5. Herpes simplex virus (HSV-2) - less common ║
║ ║
║ 6. Adenovirus (5-10%) ║
║ ║
║ 7. Unknown cause (10-30%) ║
╚════════════════════════════════════════════════════════════╝
- Mucopurulent/mucoid urethral discharge (less purulent than gonococcal)
- Dysuria (burning during micturition)
- Urethral itching
- Often asymptomatic (especially Chlamydia in women)
- Complications: Epididymitis, Reiter's syndrome (reactive arthritis), PID
- Obligate intracellular bacterium
- Two forms: Elementary body (infective, EB) ↔ Reticulate body (intracellular, dividing, RB)
- Cannot be grown on ordinary media (cell culture required)
| Test | Details |
|---|---|
| NAAT (PCR) | Gold standard; urine or urethral swab; detects C. trachomatis + N. gonorrhoeae simultaneously |
| Urethral smear Gram stain | ≥5 PMNs/hpf with no gram-ve diplococci = NGU |
| Cell culture | Gold standard for Chlamydia (complex, rare now) |
| Antigen detection (ELISA/IF) | DFA (Direct Fluorescent Antibody) for Chlamydia |
| Urine (first-catch) | For NAAT; first 10-20 mL of urine stream |
| Wet mount | For Trichomonas (motile flagellate trophozoites) |
- Chlamydia: Doxycycline 100mg BD x 7 days (DOC) OR Azithromycin 1g oral single dose
- Mycoplasma genitalium: Moxifloxacin 400mg OD x 7-14 days (azithromycin-resistant strains)
- Ureaplasma: Doxycycline / Azithromycin
- Treat sexual partner simultaneously
Q14. ORGANISMS CAUSING UTI; SPECIMEN COLLECTION IN UTI
Organisms Causing UTI:
╔══════════════════════════════════════════════════════════════════╗
║ ORGANISMS RESPONSIBLE FOR UTI ║
║ ║
║ COMMUNITY-ACQUIRED UTI (ascending, uncomplicated): ║
║ 1. Escherichia coli (75-85%) ← MOST COMMON ║
║ P-fimbriae (mannose-resistant), α-haemolysin ║
║ 2. Klebsiella pneumoniae (5-10%) ║
║ 3. Staphylococcus saprophyticus (5-15% in young women) ║
║ 4. Proteus mirabilis (urease → alkaline urine → struvite stones)║
║ 5. Enterococcus faecalis (especially after instrumentation) ║
║ ║
║ HOSPITAL-ACQUIRED / CATHETER UTI: ║
║ 1. E. coli (still most common) ║
║ 2. Candida spp. (commonest fungal cause of CAUTI) ║
║ 3. Pseudomonas aeruginosa ║
║ 4. Klebsiella spp. (ESBL-producing) ║
║ 5. Enterococcus ║
║ 6. Serratia, Acinetobacter (MDR) ║
║ ║
║ SPECIAL UTI ORGANISMS: ║
║ • Staphylococcus aureus UTI → suspect haematogenous spread ║
║ • Mycobacterium tuberculosis → sterile pyuria (VERY IMPORTANT) ║
║ • Schistosoma haematobium → haematuria + secondary infection ║
║ • Adenovirus → haemorrhagic cystitis ║
╚══════════════════════════════════════════════════════════════════╝
Specimen Collection in UTI (IN DETAIL):
╔══════════════════════════════════════════════════════════════════╗
║ URINE SPECIMEN COLLECTION - STEP BY STEP ║
║ ║
║ A. MIDSTREAM CLEAN CATCH URINE (MSU) - Standard method: ║
║ ║
║ TIMING: First morning specimen preferred ║
║ (concentrated; bacteria multiplied overnight) ║
║ ║
║ PROCEDURE: ║
║ FEMALES: ║
║ 1. Wash hands thoroughly ║
║ 2. Clean labia with soap-water or antiseptic wipe ║
║ (front to back, one wipe = one stroke) ║
║ 3. Hold labia apart during voiding ║
║ 4. Discard FIRST 10-20 mL (flush urethra) ║
║ 5. Collect MIDSTREAM 20-30 mL in STERILE WIDE-MOUTH container ║
║ 6. Cap immediately, label (name, time) ║
║ ║
║ MALES: ║
║ 1. Retract foreskin (if uncircumcised) ║
║ 2. Clean glans with moist swab ║
║ 3. Discard first 10-20 mL, collect mid-stream ║
║ ║
║ TRANSPORT: ║
║ • Process within 1 HOUR of collection (at room temperature) ║
║ • Refrigerate at 4°C if delay (up to 24 hours) ║
║ • Boric acid tubes (grey cap): preserve at room temperature ║
║ x 48 hours; add 3 mL of urine to tube ║
║ ║
║ B. CATHETER SPECIMEN URINE (CSU): ║
║ • Clean catheter port with alcohol swab ║
║ • Use sterile syringe and needle to aspirate from port ║
║ • NEVER collect from the drainage bag ║
║ ║
║ C. SUPRAPUBIC ASPIRATION (SPA): ║
║ • Gold standard (no contamination) ║
║ • Sterile needle directly into bladder through anterior wall ║
║ • Used for: neonates, equivocal results, anaerobic culture ║
║ ║
║ D. PAEDIATRIC COLLECTION: ║
║ • Adhesive plastic bag over genitalia ║
║ • High contamination rate - repeat if positive ║
║ • SPA preferred in neonates ║
╚══════════════════════════════════════════════════════════════════╝
Q15. NOTE ON CUTANEOUS LARVA MIGRANS (CLM)
- Ancylostoma braziliense (most common - cat/dog hookworm) - DOG HOOKWORM
- Ancylostoma caninum
- Uncinaria stenocephala
- (Humans are accidental hosts - larvae cannot complete development)
Pathogenesis:
╔══════════════════════════════════════════════════════════════════╗
║ PATHOGENESIS OF CUTANEOUS LARVA MIGRANS ║
║ ║
║ DOG/CAT defecates on soil → Eggs in faeces ║
║ ↓ (develop in warm, moist, sandy soil) ║
║ FILARIFORM (L3) LARVAE in soil ║
║ ↓ (skin contact - walking barefoot, sunbathing) ║
║ PENETRATION of human skin (especially feet, hands, buttocks) ║
║ ↓ (humans = dead-end / accidental host) ║
║ Larva CANNOT find proper host receptors to go deeper ║
║ ↓ ║
║ Larva migrates HORIZONTALLY through epidermis ║
║ (few mm/day → few cm/day) ║
║ ↓ ║
║ SERPIGINOUS (snake-like) TRACK in skin ║
║ = CREEPING ERUPTION ║
║ (intense eosinophilic inflammation + pruritus) ║
║ ↓ ║
║ Eventually dies (self-limiting) in 4-8 weeks ║
╚══════════════════════════════════════════════════════════════════╝
Clinical Features:
- Intensely pruritic, serpiginous (winding/snake-like) track
- Erythematous, raised, vesicular/papular eruption
- Advances 1-2 cm/day
- Site: Feet, hands, buttocks (wherever skin contacts soil)
- Eosinophilia in blood
- Self-limiting (4-8 weeks if untreated)
DIAGRAM - CLM (Easy to draw):
╔══════════════════════════════════════════════════════╗
║ CUTANEOUS LARVA MIGRANS - SKIN DIAGRAM ║
║ ║
║ SKIN SURFACE: ║
║ ───────────────────────────────────────────────── ║
║ ~~~~~~~~~~~~~~~~~~~~→ ← Serpiginous track ║
║ ~~~~~~~~~~~~~~~~~~ (red, raised, winding) ║
║ ●~~~~~~~~~~~~~~~~~ ← Larva (at advancing end) ║
║ ───────────────────────────────────────────────── ║
║ EPIDERMIS (larva confined here) ║
║ ───────────────────────────────────────────────── ║
║ DERMIS ║
║ ║
║ Eosinophils around the track ║
╚══════════════════════════════════════════════════════╝
- Clinical diagnosis (characteristic appearance)
- Skin biopsy: Eosinophilic infiltrate; larva may be found (ahead of visible track, 1-2 cm)
- Blood: Peripheral eosinophilia
- No specific serological test
- Ivermectin 200 μg/kg single oral dose (DOC - most effective)
- Albendazole 400mg OD x 3 days (alternative, highly effective)
- Topical Thiabendazole (10-15% cream, applied 3x/day x 5-7 days) - for limited lesions
- Cryotherapy - NOT recommended (larva is ahead of the visible track)
Q16. LAB DIAGNOSIS OF GAS GANGRENE INFECTION
- Gas gangrene (Myonecrosis) - C. perfringens
- Tetanus - C. tetani
- Botulism - C. botulinum
- Food poisoning - C. perfringens Type A
- C. difficile colitis (AAD/PMC) - C. difficile
Morphology of C. perfringens:
╔══════════════════════════════════════════════════════════╗
║ C. PERFRINGENS - MORPHOLOGY ║
║ ║
║ • Gram-positive, large, thick, box-car shaped bacilli ║
║ • Anaerobic (obligate) ║
║ • SPORES: Subterminal, oval (but spores RARELY seen ║
║ in tissue - unlike other Clostridia) ║
║ • CAPSULE: Present (antiphagocytic) ║
║ • Motility: NON-MOTILE (unlike other Clostridia) ║
║ • Toxins: Alpha toxin (phospholipase C) = MOST IMPORTANT║
╚══════════════════════════════════════════════════════════╝
Lab Diagnosis of Gas Gangrene:
╔══════════════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS OF GAS GANGRENE ║
║ ║
║ 1. GRAM STAIN OF WOUND SMEAR (MOST IMPORTANT initial test): ║
║ • Large gram-POSITIVE thick bacilli (box-car shape) ║
║ • ABSENCE of PMNs (toxins destroy neutrophils) ║
║ • ABSENCE of PMNs despite infection = highly characteristic ║
║ • Background: necrotic tissue fragments ║
║ ║
║ 2. CULTURE (ANAEROBIC - essential): ║
║ • Robertson's cooked meat (RCM) medium ║
║ • Thioglycollate broth ║
║ • Blood agar in anaerobic jar (Gas-Pak system) ║
║ ║
║ Blood agar - C. perfringens colonies: ║
║ • Double zone of hemolysis: ║
║ INNER zone: complete (beta-hemolysis) - theta toxin ║
║ OUTER zone: partial (alpha-hemolysis) - alpha toxin ║
║ • "Stormy fermentation" in litmus milk broth: ║
║ Rapid clot formation + gas = "stormy clot" (PATHOGNOMONIC) ║
║ ║
║ 3. NAGLER REACTION: ║
║ • Egg-yolk agar (lecithovitellin agar) ║
║ • Alpha toxin (lecithinase) cleaves lecithin in egg yolk ║
║ → OPAQUE precipitate (pearly layer) around colonies ║
║ → INHIBITED by specific anti-alpha-toxin antiserum ║
║ = NAGLER REACTION POSITIVE ║
║ • PATHOGNOMONIC of C. perfringens ║
║ ║
║ 4. X-RAY / IMAGING: ║
║ • Crepitus in tissue (gas) on plain X-ray ║
║ • MRI: Gas in muscle planes, necrosis ║
║ ║
║ 5. TOXIN IDENTIFICATION: ║
║ • ELISA for alpha-toxin ║
║ • Reverse passive haemagglutination (RPHA) ║
║ • Mouse lethality test (historical) ║
║ ║
║ 6. PCR: For toxin genes (cpa for alpha toxin) ║
╚══════════════════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════════════╗
║ NAGLER REACTION (Egg-yolk agar) ║
║ ║
║ LEFT HALF (no antiserum): RIGHT HALF (+ antiserum):║
║ ┌─────────────────┐ ┌─────────────────┐ ║
║ │ Colony │ │ Colony │ ║
║ │ ◐◐◐◐◐◐ │ │ (no opacity) │ ║
║ │ OPAQUE ZONE │ │ INHIBITED │ ║
║ │ (positive) │ │ │ ║
║ └─────────────────┘ └─────────────────┘ ║
╚══════════════════════════════════════════════════════╝
- Surgical debridement (MOST IMPORTANT) - wide excision of all necrotic tissue, amputation if needed
- Penicillin G IV high dose (DOC) + Metronidazole OR Clindamycin
- Hyperbaric Oxygen (HBO): Anaerobic organism inhibited by high O2; adjunct therapy
- Polyvalent antitoxin (limited evidence)
Q17. DIFFERENCE BETWEEN HSV-1 AND HSV-2
╔══════════════════════════════════════════════════════════════════════╗
║ HSV-1 vs HSV-2 - COMPARISON TABLE ║
╠══════════════════════╦═══════════════════════╦════════════════════════╣
║ Feature ║ HSV-1 ║ HSV-2 ║
╠══════════════════════╬═══════════════════════╬════════════════════════╣
║ Common name ║ Oral herpes ║ Genital herpes ║
║ Primary site ║ Oropharynx (lips, ║ Genitalia, buttocks, ║
║ ║ gingiva) ║ thighs ║
║ Transmission ║ Saliva, droplets, ║ Sexual contact, ║
║ ║ direct contact ║ vertical ║
║ Latency site ║ Trigeminal ganglion ║ Sacral dorsal root ║
║ ║ (CN V) ║ ganglia (S2-S5) ║
║ Reactivation trigger ║ UV light, fever, ║ Stress, menstruation, ║
║ ║ stress, fever ║ immunosuppression ║
║ Recurrent lesions ║ Herpes labialis ║ Genital recurrences ║
║ ║ (cold sores) ║ (more frequent) ║
║ Meningitis ║ HSE (Herpes ║ Aseptic meningitis ║
║ ║ Simplex Encephalitis) ║ (Mollaret's meningitis)║
║ ║ - temporal lobe, FATAL║ ║
║ Keratoconjunctivitis ║ YES (common) ║ Rare ║
║ Neonatal herpes ║ Less common ║ More common (birth ║
║ ║ ║ canal exposure) ║
║ Carcinoma assoc. ║ Oral/oropharyngeal ║ Cervical carcinoma ║
║ ║ (co-factor with HPV) ║ (co-factor) ║
║ Lab differentiation ║ Cytopathic effect; ║ PCR (most reliable) ║
║ ║ Type-specific ELISA ║ Type-specific IgG ║
║ Treatment ║ Acyclovir (topical ║ Valacyclovir oral ║
║ ║ or oral) ║ (episodic/suppressive) ║
╚══════════════════════╩═══════════════════════╩════════════════════════╝
- Family: Herpesviridae; Large dsDNA virus; Enveloped
- ICOSAHEDRAL capsid; Tegument layer between capsid and envelope
- Establish latency in sensory ganglia
- Reactivate during immunosuppression
- Cytopathic effect: Intranuclear inclusions (Cowdry type A - eosinophilic)
- Tzanck smear: Multinucleated giant cells (both types)
- Treatment: Acyclovir / Valacyclovir / Famciclovir (all require viral thymidine kinase for activation)
Q18. BRIEF NOTE ON PCP PNEUMONIA IN HIV INDIVIDUALS
- Formerly thought to be protozoan; reclassified as FUNGUS (Ascomycota) based on rRNA and wall biochemistry
- Cannot be cultured in vitro
- AIDS-defining illness when CD4 <200 cells/μL
Morphology:
- Trophozoites: Small, 1-4 μm, pleomorphic
- Cysts (Asci): 5-8 μm, spherical, contain 8 intracystic bodies (ascospores)
- Pneumocysts: Cysts with 8 intracystic bodies
Clinical Features (HIV/AIDS, CD4 typically <200):
╔══════════════════════════════════════════════════════════════╗
║ CLINICAL FEATURES OF PCP IN HIV ║
║ ║
║ INSIDIOUS ONSET (weeks): ║
║ ├── Progressive exertional dyspnoea (most common) ║
║ ├── Dry, non-productive COUGH ║
║ ├── LOW-GRADE FEVER ║
║ ├── Fatigue, weight loss ║
║ └── NORMAL BREATH SOUNDS or fine bibasal crackles ║
║ ║
║ INVESTIGATIONS: ║
║ • SpO2 drops with exercise (HALLMARK) ║
║ • LDH elevated (>500 IU/L = bad prognosis) ║
║ • CXR: Bilateral, diffuse, INTERSTITIAL pattern ║
║ "Ground-glass" or "bat-wing" opacities ║
║ • HRCT: Bilateral ground-glass attenuation ║
║ • PaO2 < 70 mmHg = severe (needs adjunct steroids) ║
╚══════════════════════════════════════════════════════════════╝
Lab Diagnosis:
| Test | Details |
|---|---|
| Giemsa stain (BAL) | Shows cysts + trophozoites (trophozoites stain well) |
| GMS (Gomori Methenamine Silver) | Cysts stain BLACK; best for cyst identification |
| Toluidine Blue O | Cysts stain blue; fast and easy |
| Calcoflour White | Fluorescent; highly sensitive for cyst wall |
| IFA (Immunofluorescence) | Monoclonal antibody; gold standard sensitivity (~95%) |
| PCR (BAL/serum) | Most sensitive; quantitative PCR preferred |
| Beta-D-glucan (serum) | Elevated (>80 pg/mL); sensitive but not specific for PCP |
GMS STAIN DIAGRAM (exam-friendly):
╔══════════════════════════════════════════════════╗
║ PCP CYSTS on GMS stain ║
║ ║
║ Green/brown background ║
║ ◯ ◯ ◯ ← Black cysts (cup-shaped or ║
║ ◯ ◯ ◯ boat-shaped with "dot" = ║
║ ◯ ◯ intracystic body) ║
║ 5-8 μm cysts, 8 intracystic bodies ║
║ Seen in ALVEOLAR EXUDATE (foamy) ║
╚══════════════════════════════════════════════════╝
- TMP-SMX (Co-trimoxazole) = DRUG OF CHOICE
- Mild-moderate: TMP 15-20mg/kg + SMX 75-100mg/kg/day oral x 21 days
- Severe (PaO2 <70mmHg): IV co-trimoxazole + Prednisolone 40mg BD x 5 days (then taper)
- Alternatives: Pentamidine IV, Dapsone + TMP, Clindamycin + Primaquine
- Co-trimoxazole DS 1 tablet OD (also prophylaxis for Toxoplasma)
- Discontinue when CD4 >200 sustained for 3 months on ART
Q19. ENUMERATE DERMATOPHYTE INFECTIONS AND LAB DIAGNOSIS
Dermatophytes (Ringworm fungi):
- Trichophyton - skin, hair, nails (most species)
- Microsporum - skin and hair (NOT nails)
- Epidermophyton - skin and nails (NOT hair)
Classification of Dermatophytoses (TINEA):
╔══════════════════════════════════════════════════════════════════╗
║ DERMATOPHYTE INFECTIONS - CLASSIFICATION ║
║ ║
║ TINEA (Ringworm): ║
║ ┌─────────────────────────────────────────────────────────┐ ║
║ │ DISEASE │ SITE │ COMMON ORGANISM │ ║
║ ├─────────────────────────────────────────────────────────┤ ║
║ │ Tinea capitis │ Scalp │ Trichophyton tonsurans│ ║
║ │ (ringworm scalp) │ │ Microsporum canis │ ║
║ ├─────────────────────────────────────────────────────────┤ ║
║ │ Tinea corporis │ Body skin │ T. rubrum, M. canis │ ║
║ │ (ringworm body) │ │ │ ║
║ ├─────────────────────────────────────────────────────────┤ ║
║ │ Tinea cruris │ Groin │ T. rubrum │ ║
║ │ (jock itch) │ (perineum) │ E. floccosum │ ║
║ ├─────────────────────────────────────────────────────────┤ ║
║ │ Tinea pedis │ Feet │ T. rubrum (most │ ║
║ │ (athlete's foot) │ │ common worldwide) │ ║
║ ├─────────────────────────────────────────────────────────┤ ║
║ │ Tinea unguium │ Nails │ T. rubrum │ ║
║ │ (Onychomycosis) │ │ │ ║
║ ├─────────────────────────────────────────────────────────┤ ║
║ │ Tinea barbae │ Beard │ T. violaceum │ ║
║ │ Tinea faciei │ Face │ T. mentagrophytes │ ║
║ └─────────────────────────────────────────────────────────┘ ║
║ ║
║ EPIDEMIOLOGICAL CLASSIFICATION: ║
║ • Zoophilic: From animals (M. canis from cats/dogs) ║
║ • Anthropophilic: Human-to-human (T. rubrum, T. tonsurans) ║
║ • Geophilic: From soil (M. gypseum) ║
╚══════════════════════════════════════════════════════════════════╝
Lab Diagnosis of Dermatophytoses:
- Skin: Scrapings from active edge of lesion (not center which is healed)
- Hair: Infected hair stubs + kerion material (pull with forceps - fluorescent hair under UV)
- Nails: Nail clippings + subungual debris (deep scrapings)
╔══════════════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS OF DERMATOPHYTES ║
║ ║
║ 1. WOOD'S LAMP (UV light, 365 nm): ║
║ • SCREENING for scalp ringworm (Tinea capitis) ║
║ • Microsporum species → BRIGHT GREEN/YELLOW-GREEN ║
║ fluorescence (due to pteridine in hair shaft) ║
║ • Trichophyton → NO fluorescence (exception: T. schoenleinii)║
║ • Quick in-office screening ║
║ ║
║ 2. KOH MOUNT (10-20% KOH - key diagnostic test): ║
║ • Dissolves keratin → reveals fungal elements ║
║ • Skin scraping + 1-2 drops 20% KOH on glass slide ║
║ • Gently heat → wait 15-20 min ║
║ • POSITIVE: Branching, septate hyphae (skin/nails) ║
║ Arthrospores within/around hair shaft (endothrix/ ║
║ ectothrix - Tinea capitis) ║
║ ║
║ HAIR INVASION PATTERNS (Tinea capitis): ║
║ ├── ECTOTHRIX: Arthroconidia on OUTSIDE hair shaft ║
║ │ (Microsporum, T. mentagrophytes) ║
║ └── ENDOTHRIX: Arthroconidia INSIDE hair shaft ║
║ (T. tonsurans, T. violaceum) - "black dot" tinea ║
║ → Hair breaks within follicle → black dot on scalp ║
║ ║
║ 3. CULTURE (SDA): ║
║ • SDA with chloramphenicol + cycloheximide ║
║ (DTM - Dermatophyte Test Medium: colour change red) ║
║ • Incubate at 25-28°C for 1-4 weeks ║
║ • Identify by: Colony morphology + LPCB mount ║
║ ║
║ LPCB MOUNT (Lactophenol Cotton Blue): ║
║ • T. rubrum: Pencil-shaped macroconidia (rare); microconidia ║
║ • T. mentagrophytes: Spiral hyphae, grape-like microconidia ║
║ • Microsporum: Spindle-shaped macroconidia with thick walls ║
║ • Epidermophyton: Beaver-tail shaped macroconidia (no micro) ║
║ ║
║ 4. FLUORESCENCE MICROSCOPY (Calcoflour white + KOH): ║
║ Most sensitive for detecting hyphae in specimens ║
╚══════════════════════════════════════════════════════════════════╝
- Topical: Clotrimazole, Miconazole, Terbinafine, Ketoconazole cream
- Systemic (scalp/nail/extensive): Griseofulvin (Tinea capitis, especially Microsporum - binds keratin); Terbinafine (Tinea unguium/nails - DOC); Itraconazole
Q20. NEUROCYSTICERCOSIS - PATHOGENESIS, DIAGNOSIS, CLINICAL FEATURES, CNS DIAGNOSTIC TOOLS
- Ingestion of T. solium EGGS (not cysticerci) via contaminated food/water
- Autoinfection: Reverse peristalsis/vomiting brings gravid proglottids to stomach
Pathogenesis:
╔══════════════════════════════════════════════════════════════════╗
║ PATHOGENESIS OF NEUROCYSTICERCOSIS ║
║ ║
║ T. solium EGGS ingested ║
║ ↓ Gastric acid → oncospheres released ║
║ ONCOSPHERES penetrate gut wall ║
║ ↓ Blood + lymphatics ║
║ Reach BRAIN (most common site of extraintestinal cysticercosis) ║
║ ↓ ║
║ CYSTICERCUS CELLULOSAE develops in brain parenchyma ║
║ (also subarachnoid space, ventricles, spinal cord) ║
║ ↓ ║
║ STAGES: ║
║ 1. Vesicular: Live cyst, minimal inflammation; ASYMPTOMATIC ║
║ 2. Colloidal vesicular: Cyst begins to degenerate; WBC attracted║
║ Inflammation, edema → SEIZURES, HEADACHE ║
║ 3. Granular nodular: Calcifying; fibrosis ║
║ 4. Calcified nodular: Dead calcified cyst; may still cause ║
║ seizures (calcification triggers inflammation) ║
╚══════════════════════════════════════════════════════════════════╝
Clinical Features:
| Feature | Details |
|---|---|
| Seizures | MOST COMMON (70-90%) - focal or generalized |
| Headache | Second most common; raised ICP |
| Focal neurological deficits | Hemiparesis, aphasia, cranial nerve palsies |
| Hydrocephalus | Intraventricular or subarachnoid cysts → CSF obstruction |
| Meningitis | Subarachnoid cysticercosis → CSF eosinophilia |
| Spinal cord | Weakness, paraparesis (rare) |
Diagnosis - CNS Diagnostic Tools:
CT SCAN:
• Hypodense cysts with eccentric scolex ("hole with dot" sign)
• Multiple ring-enhancing lesions (dying cysts)
• Calcified lesions (dead cysts)
• Hydrocephalus
• Perilesional edema
MRI (BEST for NCC):
• T1: Cyst isointense/hypointense to CSF; scolex (dot) = hyperintense
• T2: Fluid-filled cysts hyperintense (like CSF)
• FLAIR: Perilesional edema = hyperintense
• DWI: Abscesses (r/o) - NCC cysts do NOT restrict diffusion
• Detects: Live cysts, scolex, calcified cysts, intraventricular cysts
- Eosinophilic pleocytosis (pathognomonic when present)
- Elevated protein
- Low glucose
- CSF ELISA: Anti-cysticercal IgG antibodies
- CSF PCR: Highly specific
- EITB (Enzyme-Linked Immunoelectrotransfer Blot) - gold standard serological test; sensitivity 94-98% in multiple cysts
- ELISA: IgG anti-cysticercal antibodies
- Note: Single calcified lesion may be seronegative
- Cysticercus structure: Bladder (fluid-filled) + invaginated scolex (with 4 suckers + rostellum with hooks)
- Diagnosis confirmatory
- Albendazole 15mg/kg/day x 8-28 days (DOC - kills live cysts)
- Praziquantel (alternative)
- Dexamethasone/Prednisolone - add to reduce perilesional edema during therapy
- Anticonvulsants (AED) - Phenytoin, Carbamazepine (for seizures)
- Calcified cysts: No antiparasitic needed; manage seizures only
- Intraventricular cysts: Endoscopic removal
- Hydrocephalus: VP shunt
Q21. LAB DIAGNOSIS OF BACTERIAL UTI
Microscopy:
╔══════════════════════════════════════════════════════════════════╗
║ LAB DIAGNOSIS - BACTERIAL UTI ║
║ ║
║ SPECIMEN: MSU (Midstream clean catch urine) ║
║ ║
║ STEP 1: URINALYSIS (Dipstick) ║
║ ├── Nitrite: Positive → gram -ve bacteria (reduce nitrate) ║
║ ├── Leukocyte esterase: Positive → pyuria (WBCs present) ║
║ ├── Blood: May be positive (haemorrhagic cystitis) ║
║ └── Protein: Mild elevation ║
║ ║
║ STEP 2: MICROSCOPY (Uncentrifuged urine) ║
║ ├── WBCs: >10 cells/mm³ = pyuria ║
║ ├── RBCs: >5 cells/mm³ = haematuria ║
║ ├── Bacteria: Presence of ANY bacteria ║
║ ├── Casts: WBC casts → pyelonephritis/renal infection ║
║ └── Epithelial cells: >5 squamous cells → contaminated sample ║
║ ║
║ STEP 3: GRAM STAIN (uncentrifuged urine) ║
║ ├── 1+ bacterium/oil immersion field = 10⁵ CFU/mL ║
║ ├── Gram -ve rods (E. coli, Klebsiella, Pseudomonas) ║
║ ├── Gram +ve cocci clusters (Staph) ║
║ └── Gram +ve cocci in chains (Enterococcus) ║
║ ║
║ STEP 4: CULTURE (KEY STEP) ║
║ Media: CLED agar (Cystine Lactose Electrolyte Deficient) ║
║ MacConkey agar ║
║ Blood agar ║
║ Method: CALIBRATED LOOP (0.001 mL or 0.01 mL) ║
║ ║
║ SIGNIFICANT BACTERIURIA THRESHOLD: ║
║ • MSU (symptomatic female): ≥10³ CFU/mL ║
║ • MSU (symptomatic male): ≥10³ CFU/mL ║
║ • Asymptomatic bacteriuria (screening): ≥10⁵ CFU/mL in 2 MSUs ║
║ • Catheter specimen: ≥10³ CFU/mL ║
║ • Suprapubic aspiration: ANY growth significant ║
║ ║
║ STEP 5: IDENTIFICATION + SENSITIVITY ║
║ ├── Biochemical tests (IMVIC for E. coli) ║
║ ├── Oxidase test (Pseudomonas = positive) ║
║ ├── API 20E / MALDI-TOF (rapid ID) ║
║ └── AST: Kirby-Bauer disk diffusion / MIC (VITEK) ║
╚══════════════════════════════════════════════════════════════════╝
- E. coli: Yellow, opaque (lactose fermenter)
- Klebsiella: Mucoid, yellow (lactose fermenter)
- Pseudomonas: Blue-green, non-lactose fermenter
- Proteus: Translucent, non-lactose fermenter
Q22. WELL-LABELLED DIAGRAM OF RABIES VIRUS AND PEP
Rabies Virus Diagram:
╔══════════════════════════════════════════════════════════════════╗
║ RABIES VIRUS - WELL LABELLED DIAGRAM ║
║ ║
║ ←────── 180 nm ──────→ ║
║ ┌──────────────────────┐ ║
║ │ ↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑ │ ← Glycoprotein (G) spikes ║
║ FLAT │ ████████████████████ │ ← LIPID ENVELOPE ║
║ END │ ─────────────────── │ ← MATRIX (M) protein ║
║ ←──→ │ ╔═══╗ ╔═══╗ ╔═══╗ │ ║
║ │ ║RNA║═║ N ║═║L/P║ │ ← RNP (ssRNA + N + L + P) ║
║ │ ╚═══╝ ╚═══╝ ╚═══╝ │ ║
║ │ ─────────────────── │ ← MATRIX (M) protein ║
║ │ ████████████████████ │ ← LIPID ENVELOPE ║
║ │ ↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑↑ │ ← G-protein spikes ║
║ └──────────────────────┘ ║
║ → ROUNDED END ║
║ ║
║ KEY: ║
║ • Shape: BULLET/BACILLIFORM (180×75 nm) ║
║ • Genome: ssRNA, negative sense, non-segmented ║
║ • Nucleocapsid: Helical symmetry ║
║ • G protein: Induces virus-neutralizing antibodies ║
║ Responsible for attachment to nAchR and P75NTR ║
║ • N protein: Forms Negri bodies in infected neurons ║
╚══════════════════════════════════════════════════════════════════╝
PEP (Post-Exposure Prophylaxis) Chart:
╔══════════════════════════════════════════════════════════════════╗
║ RABIES PEP - COMPLETE PROTOCOL ║
║ ║
║ STEP 1: WOUND MANAGEMENT (IMMEDIATE - MOST IMPORTANT) ║
║ ├── Wash wound with soap + water x 15 min ║
║ ├── Apply 70% alcohol/povidone-iodine ║
║ ├── Do NOT suture (if must suture, do it late, loosely) ║
║ └── Tetanus prophylaxis if needed ║
║ ║
║ STEP 2: WHO CATEGORY ASSESSMENT ║
║ ├── Cat I (touch/lick intact skin): Wash only, NO PEP ║
║ ├── Cat II (minor scratch, no bleeding): Vaccine series ║
║ └── Cat III (deep bite/bleed/mucosa): Vaccine + RIG ║
║ ║
║ STEP 3: VACCINE (Essen 5-dose IM schedule): ║
║ Day 0 → Day 3 → Day 7 → Day 14 → Day 28 ║
║ (IM deltoid; cell culture vaccine: PCECV/PVRV/HDCV) ║
║ ║
║ STEP 4: RIG (ONLY Cat III, given on Day 0 ONLY): ║
║ ├── HRIG (Human): 20 IU/kg ║
║ └── ERIG (Equine): 40 IU/kg (after sensitivity testing) ║
║ → Infiltrate maximum at wound site ║
║ → Remaining IM at distant site from vaccine ║
║ ║
║ FOR PREVIOUSLY VACCINATED (PrEP done): ║
║ → 2 doses ONLY: Day 0 + Day 3 (NO RIG needed) ║
║ ║
║ INTRADERMAL (ID) 2-site schedule (economical, India): ║
║ Day 0 (2 sites) → Day 3 (2 sites) → Day 7 (2 sites) → ║
║ Day 28 (1 site) → Day 90 (1 site) ║
╚══════════════════════════════════════════════════════════════════╝
Q23. DEFINE PRECIPITATION AND APPLICATIONS WITH EXAMPLES
- Antigen must be SOLUBLE (not particulate → that's agglutination)
- Optimal proportions (zone of equivalence): Neither antigen nor antibody in excess
- Electrolytes (NaCl, physiological saline) needed
Zone Phenomenon (Lattice theory):
╔══════════════════════════════════════════════════════════════════╗
║ LATTICE THEORY / ZONE PHENOMENON ║
║ ║
║ ANTIBODY ZONE OF ANTIGEN ║
║ EXCESS EQUIVALENCE EXCESS ║
║ ┌─────────┐ ┌─────────────┐ ┌─────────┐ ║
║ │ Small │ │ MAXIMUM │ │ Small │ ║
║ │ lattice │ │ PRECIPITATE │ │ lattice │ ║
║ │ = small │ │ (OPTIMAL) │ │ = small │ ║
║ │precipit.│ │ │ │precipit.│ ║
║ └─────────┘ └─────────────┘ └─────────┘ ║
║ (prozone) (equivalence) (postzone) ║
║ ║
║ PROZONE: Ab excess → small, soluble lattice → NO precipitate ║
║ POSTZONE: Ag excess → small, soluble lattice → NO precipitate ║
║ ZONE OF EQUIVALENCE: MAXIMUM large lattice = MAX precipitate ║
╚══════════════════════════════════════════════════════════════════╝
Types of Precipitation Reactions (with Applications & Examples):
╔══════════════════════════════════════════════════════════════════╗
║ TYPES OF PRECIPITATION REACTIONS ║
║ ║
║ 1. PRECIPITATION IN LIQUIDS: ║
║ a. RING (Interfacial) TEST (Ascoli's test): ║
║ • Antigen layered over antibody in narrow tube ║
║ • Precipitate forms at interface as RING ║
║ • Application: Diagnosis of ANTHRAX ║
║ (Ascoli's thermoprecipitin test for anthrax in hides) ║
║ ║
║ 2. PRECIPITATION IN GEL (Agar/Agarose): ║
║ ║
║ a. DOUBLE IMMUNODIFFUSION (Ouchterlony method): ║
║ • Both Ag and Ab diffuse toward each other in agar ║
║ • Precipitin line forms where they meet ║
║ • Applications: ║
║ ✓ Detect M and H bands in Histoplasmosis ║
║ ✓ Identify fungal species (Aspergillus precipitins) ║
║ ✓ Characterize antigen-antibody identity/cross-react. ║
║ ║
║ b. SINGLE RADIAL IMMUNODIFFUSION (SRID - Mancini): ║
║ • Ab in agar, Ag in well ║
║ • Area of precipitin ring ∝ Ag concentration ║
║ • Application: QUANTIFY immunoglobulins (IgG, IgA, IgM) ║
║ Complement components (C3, C4) ║
║ ║
║ c. IMMUNOELECTROPHORESIS (IEP): ║
║ • Ag separated by electrophoresis first, then ║
║ antibody diffuses from trough ║
║ • Application: Identify myeloma proteins (paraproteins) ║
║ ║
║ d. COUNTER CURRENT IMMUNOELECTROPHORESIS (CCIE): ║
║ • Both Ag and Ab move toward each other under current ║
║ • RAPID and MORE SENSITIVE than Ouchterlony ║
║ • Application: Bacterial antigens in CSF/serum ║
║ (meningococcus, H. influenzae, S. pneumoniae) ║
║ Anti-dsDNA in SLE, CIE in Leptospirosis ║
║ ║
║ 3. IMMUNOTURBIDIMETRY / IMMUNONEPHELOMETRY: ║
║ • Ag-Ab complex = turbidity measured by light scattering ║
║ • Application: Quantify CRP, IgG, IgA, IgM, complement ║
║ in clinical labs (automated analyzers) ║
╚══════════════════════════════════════════════════════════════════╝
Summary Table:
| Test | Principle | Application/Example |
|---|---|---|
| Ring test (Ascoli) | Interfacial precipitin | Anthrax diagnosis in hides |
| Ouchterlony (double diffusion) | Both diffuse in agar | Histoplasma M/H bands; identity/cross-reactivity |
| Mancini (SRID) | Ag diffuses into Ab-agar | Quantify IgG, IgM, IgA, C3, C4 |
| CCIE | Electrophoresis of both | CSF antigens (meningitis), CIE Leptospirosis |
| Immunoelectrophoresis | Electrophoresis + diffusion | Paraprotein detection (multiple myeloma) |
| Immunonephelometry | Light scatter of complexes | CRP, serum proteins (automated lab) |
- False negative result due to ANTIBODY EXCESS in undiluted serum
- Example: VDRL test in secondary syphilis (very high antibody titre → prozone → false negative → dilute serum to get positive result)
- Solution: Test serum at multiple dilutions
References: Apurba Shastri's Textbook of Microbiology (4th Ed); Jawetz Melnick & Adelberg 28th Ed; Murray's Medical Microbiology 9th Ed; WHO Rabies Guidelines; India NIP/NVBDCP schedules; NACO guidelines.
MUHS Exam Tip: For 5-mark SAQs, ideal structure = Definition (1 mark) + Classification or Pathogenesis (2 marks) + Diagram/Table (1 mark) + Lab diagnosis or Treatment (1 mark). For 8-10 mark LAQs, each sub-part gets 2-3 marks. Time: 2 min per mark = 16-20 min for a 10-mark LAQ.