TB melenjites
Reading File
Finding Sources
Searching PubMed
"tuberculous meningitis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Here is a detailed review of tuberculous meningitis (TB meningitis):
Tuberculous Meningitis (TB Meningitis)
Definition
Tuberculous (TB) meningitis is the most severe form of extrapulmonary tuberculosis, caused by Mycobacterium tuberculosis infecting the meninges and subarachnoid space. It is technically a meningoencephalitis because the process frequently penetrates the pia and ependymia to invade underlying brain parenchyma.
Epidemiology
- More common in children historically, but now more frequent in adults (at least in the US)
- Strong association with HIV - incidence is ~500 times higher in AIDS patients than in the general population
- High prevalence in sub-Saharan Africa, parts of Asia, India, and former Soviet Union (25x the US rate), largely due to HIV co-infection
- Also seen in alcoholics, recent immigrants from high-burden countries, and the immunocompromised
Pathogenesis
TB meningitis does NOT arise from direct hematogenous seeding of the meninges. The two-stage process is:
- First stage: Hematogenous dissemination deposits miliary tubercle bacilli in the brain parenchyma and subpial regions, forming millet seed-sized caseating granulomas (Rich foci)
- Second stage: One or more granulomas rupture, discharging bacilli and mycobacterial antigens into the subarachnoid space (SAS), triggering an intense inflammatory response
The resulting exudate is thick and gelatinous, concentrating at the basal cisterns (obliterating the pontine and interpeduncular cisterns), wrapping around cranial nerves, and surrounding major blood vessels.
Causative organisms: Primarily M. tuberculosis; rarely M. bovis, M. avium, M. kansasii, or M. fortuitum (the last after neurosurgical procedures). Atypical mycobacteria are increasingly implicated in HIV patients.
Pathology
- Gross: Small white discrete tubercles over the base of the brain. Thick basal exudate. Convexities relatively spared (partly because hydrocephalus obliterates the cerebral subarachnoid space)
- Microscopic: Meningeal tubercles with central caseation, surrounded by epithelioid cells, giant cells, lymphocytes, plasma cells, and connective tissue. Exudate: fibrin, lymphocytes, plasma cells, and mononuclear cells
- Sequelae:
- Cranial nerve involvement (cranial nerves pass through the exudate-filled cisterns)
- Arteritis and cerebral infarction (vasculitis)
- Obstructive or communicating hydrocephalus (blockage of basal cisterns or aqueduct)
- Spinal radiculopathy (exudate extends to the spinal cord)
Clinical Features
Onset: Subacute/insidious over 1-2 weeks (contrast with acute bacterial meningitis). This delay is a key distinguishing feature.
| Feature | Detail |
|---|---|
| Fever | Low-grade, present in most |
| Headache | >50% of cases |
| Stiff neck / meningism | ~75% of cases; may be absent in infants |
| Altered sensorium | Lethargy, confusion, malaise |
| Cranial nerve palsies | ~20% (ocular > facial > auditory); due to basal exudate |
| Papilledema | Raised ICP from hydrocephalus |
| Focal deficits | From hemorrhagic infarction (arteritis) |
| Seizures | Especially in young children |
| Hyponatremia | Additional feature (SIADH) |
| Hypothermia | Occasionally noted |
In infants and young children: apathy, hyperirritability, vomiting, and seizures predominate; neck stiffness may be absent.
In ~two-thirds of patients, there is active TB elsewhere (usually lungs, occasionally bone, kidney, bowel, or ear).
CSF Findings (Classic Pattern)
| Parameter | Finding |
|---|---|
| Opening pressure | Elevated |
| Appearance | Clear / xanthochromic; may form a "cobweb" clot or pellicle |
| WBC | Lymphocytic pleocytosis, 10-500 cells/µL |
| Protein | Elevated, 1-5 g/L |
| Glucose | Decreased, 1.1-2.2 mmol/L (20-40 mg/dL); CSF:serum glucose ratio <0.5 |
Diagnosis
| Test | Yield |
|---|---|
| AFB smear (CSF) | Very low: 10-40% (last tube collected is best; examine clot/pellicle if present) |
| AFB culture | Gold standard; positive in ~50%; takes 4-8 weeks |
| Multiplex PCR (Xpert MTB/RIF Ultra) | More sensitive than single-primer PCR; sensitivity not fully defined for CSF |
| ADA (adenosine deaminase) | Significantly elevated in TB meningitis vs. other meningitides |
| Dot-ELISA (TB antigen/antibody) | Positive in ~86% of suspected TB meningitis cases |
| CSF lysozyme | Elevated in TB vs. bacterial and other meningitis types |
- Large-volume CSF and multiple LPs improve sensitivity of smear and culture
- CT head may be normal in 30% of mild CNS disease; gadolinium MRI is superior (shows basal enhancement, tuberculomas, hydrocephalus)
Complications
- Hydrocephalus (up to 25% require ventriculoperitoneal shunt)
- Cerebral infarction (vasculitis)
- Cranial nerve palsies
- Spinal cord involvement (myeloradiculitis)
- Tuberculoma formation
- Long-term neurologic disability (common)
Treatment
Anti-TB Drugs
Intensive phase (first 2 months): 4-drug regimen:
| Drug | Adult Dose | Key Toxicity |
|---|---|---|
| Isoniazid (INH) | 5 mg/kg/day (max 300 mg) | Neuropathy, hepatitis |
| Rifampin (RMP) | 10 mg/kg/day (adults); 15 mg/kg (children); max 600 mg | Hepatitis, drug interactions |
| Pyrazinamide (PZA) | 20-35 mg/kg/day (weight-based) | Rash, GI, hepatitis |
| Ethambutol (EMB) | 15-25 mg/kg/day (weight-based) | Optic neuropathy (visual acuity + color vision monitoring required) |
- Pyridoxine 50 mg/day added to prevent INH-induced neuropathy
- Total duration: 9-12 months (continuation phase uses INH + RMP)
- For multidrug-resistant TB: add ethionamide (ETA) as fifth drug; patients from certain regions have high rates of INH/EMB resistance
- Alternative regimen: INH + PZA + high-dose RMP + moxifloxacin
- INH and RMP can be given IV/parenterally; others are oral only
Corticosteroids (Adjunct)
- IV dexamethasone recommended alongside anti-TB drugs
- Reduces secondary complications and mortality (from 41% to 32% in a landmark Vietnamese RCT - Thwaites et al.)
- Dose: 0.4 mg/kg/day IV for 1 week, then tapering over 3-6 weeks
- Emergency dose: 0.15 mg/kg IV dexamethasone (per Rosen's EM)
Neurosurgical Indications
- Hydrocephalus: ventriculoperitoneal shunting or drainage
- Tuberculoma with mass effect not responding to drugs: surgical excision
- Pott's disease with cord compression: surgical decompression after initial chemotherapy
Related CNS TB Entities
- Tuberculous serous meningitis: Self-limited; meningeal reaction to an adjacent TB focus without frank meningitis; normal glucose, modest pleocytosis
- Tuberculoma: Space-occupying granulomatous masses (2-12 mm), may cause focal deficits or obstructive hydrocephalus; constitute 5-30% of intracranial mass lesions in developing countries
- Myeloradiculitis: Spinal cord involvement by TB exudate or Pott's disease (vertebral osteomyelitis causing kyphotic deformity and cord compression)
Prognosis
- Overall mortality: ~10% in general population
- HIV-infected patients: ~21% mortality (delayed diagnosis + drug resistance)
- Severe disability or death in roughly half of advanced cases
- Most drug resistance in developed countries results from intermittent/incomplete therapy - directly observed therapy (DOT) is recommended for at least 2 months
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed., Ch. 31
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Rosen's Emergency Medicine, 10th Ed.
- Tintinalli's Emergency Medicine, 9th Ed.
- Henry's Clinical Diagnosis and Management by Laboratory Methods
Prem villas pawa4 14 yrs male residency of anyopholl mumbai had went to hospital in vashi for fever vomiting and headache where he was admitted for 10 days but after that he was shifted to kem fmeningitsr futher investigation were he was diagnosed with TB meningitis was admitted for 14 days thn was discharged and suggested to visit opds soo on had visited opd on 13 after that he was suggested to admit and futher investigation were carried out give present medical history
Based on the clinical timeline you've described, here is a structured Present Medical History (PMH) for this patient in standard medical documentation format:
Present Medical History
Patient: Prem Villas Pawa
Age: 14 years | Sex: Male
Residence: Andheri, Mumbai
Referral: KEM Hospital, Mumbai
Chief Complaints
- Fever - since onset (duration as reported)
- Vomiting
- Headache
History of Present Illness
Master Prem Villas Pawa, a 14-year-old male resident of Andheri, Mumbai, was apparently well until he developed fever, vomiting, and headache, following which he was taken to a hospital in Vashi where he was admitted and managed for 10 days.
As the symptoms persisted and further evaluation was required, he was referred and shifted to KEM Hospital, Mumbai, where a detailed neurological workup was undertaken. On the basis of clinical examination and investigations, he was diagnosed with Tuberculous Meningitis (TB Meningitis).
He was admitted at KEM Hospital for 14 days, during which he received appropriate anti-tubercular and supportive treatment. Following clinical improvement, he was discharged with advice to attend regular Outpatient Department (OPD) follow-ups.
He visited the OPD on the 13th (of the current month), during which his clinical condition was re-evaluated. In view of the findings on review, he was advised re-admission for further investigations and management.
He is currently admitted for the same.
Summary of Timeline
| Event | Detail |
|---|---|
| Initial onset | Fever, vomiting, headache |
| 1st Admission | Vashi Hospital - 10 days |
| Referral | Shifted to KEM Hospital for further investigation |
| Diagnosis | Tuberculous Meningitis |
| 2nd Admission | KEM Hospital - 14 days |
| Discharge | Discharged with OPD follow-up advice |
| OPD Visit | 13th of the month |
| Re-admission | Advised on OPD visit; currently admitted for further investigations |
Relevant Points to Note
- No history of prior TB or anti-tubercular treatment mentioned
- No known contact with TB case documented (to be elicited)
- Immunization history to be confirmed
- BCG vaccination status relevant in this age group
- HIV status to be screened (relevant in TB meningitis workup)
- Nutritional status and socioeconomic background to be assessed
Differential Diagnosis at Presentation (for documentation)
- Tuberculous Meningitis (confirmed)
- Viral Meningitis (ruled out)
- Bacterial Meningitis (ruled out)
- Cryptococcal Meningitis (to confirm exclusion)
Note: The above history has been compiled from the clinical timeline provided. The treating clinician should verify and supplement with direct history elicitation from the patient and/or guardian, including duration of each complaint, associated symptoms (altered sensorium, seizures, neck stiffness, photophobia), past medical/surgical history, family history, drug history, and social history.
analyse_media
analyse_media
Excellent - both documents are fully extracted. Here is the complete structured Present Medical History based on the actual documents:
Present Medical History
(Based on OPD Notes + MRI Report - KEM Hospital, Parel, Mumbai)
Patient Identification
| Parameter | Details |
|---|---|
| Name | Prem Vilas Pawar |
| Age | 13 years 10 months |
| Sex | Male |
| UHID | BMC400202605842487 |
| Contact | 9136760911 |
| Hospital | King Edward Memorial Hospital (KEM), Parel, Mumbai - 400 012 |
| Payer Class | General - Self |
| OPD Visit Date | 13-Apr-2026 |
| Unit | MYN |
Chief Complaints
- Headache - since 1 month
- Vomiting - intermittent, associated with headache
- Diplopia (double vision) - both eyes, since 2 days
History of Present Illness
Master Prem Vilas Pawar, a 13-year-10-month-old male, presented to KEM Hospital OPD on 13th April 2026 with the following complaints:
Headache:
- Present since 1 month
- Predominantly right frontal, parietal, and temporal in location
- Associated with intermittent vomiting
Diplopia:
- Bilateral double vision present since 2 days
- New onset symptom at time of OPD visit
Neurological Review:
- No history of weakness in limbs
- No episodes of lower limb pain
- Power 5/5 in all four limbs
- No neck rigidity noted at the time of examination
Investigations Done Prior to OPD Visit
MRI Brain (External - 8th April 2026):
- Performed outside KEM Hospital on 8th April 2026
- Impression: ? Skull base osteomyelitis with ? Occipital lobe involvement with associated leptomeningeal enhancement
Sputum TB PCR:
- MTB NOT detected
- Note: No active cough reported by patient
Blood Investigations (from OPD notes):
| Investigation | Value | Reference |
|---|---|---|
| OT (AST) | 42 U/L | Normal |
| PT (ALT) | 44 U/L | Normal (upper limit of normal) |
| BUN | 6.5 mg/dL | Normal |
| Creatinine | 0.8 mg/dL | Normal |
| Sodium (Na) | 138 mEq/L | Normal |
| Potassium (K) | 4.4 mEq/L | Normal |
| HIV | Non-Reactive | Negative |
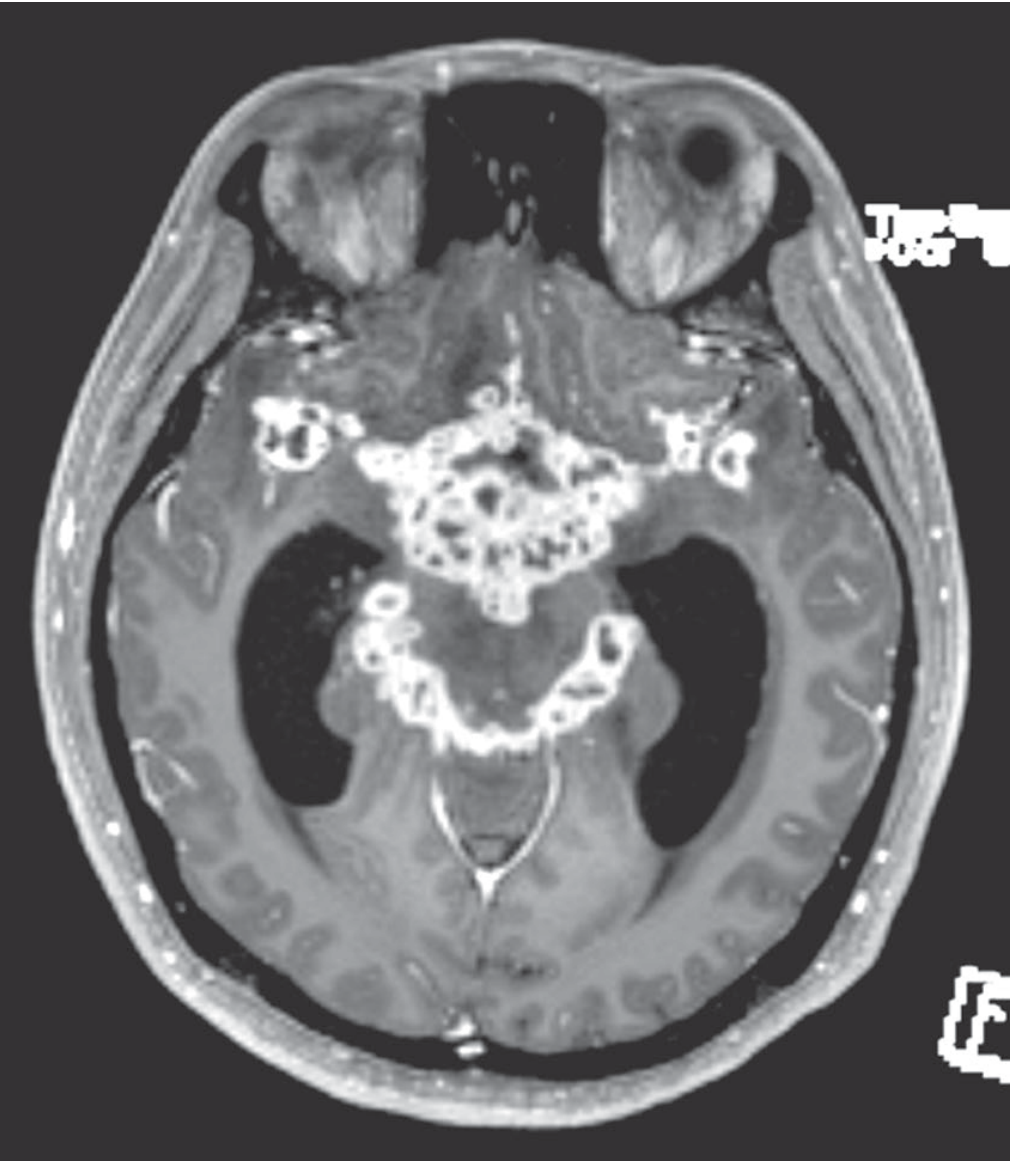
MRI Brain with Contrast - KEM Hospital
(MR No. 63589 | Date: 07/07/2026 | Reported by: JAI JR2 / Sangeetha SR)
History at time of MRI:
Known case of CNS TB, skull base osteomyelitis, on AKT (Anti-Koch's Treatment), currently having occasional headache.
Key MRI Findings:
| Finding | Detail |
|---|---|
| Hydrocephalus | Non-communicating hydrocephalus with periventricular ooze (Evan's index 0.37); lateral + 3rd ventricles dilated; 4th ventricle undilated |
| Basal Exudates | Diffuse thick avid leptomeningeal enhancement filling suprasellar, interpeduncular, prepontine, ambient, and quadrigeminal cisterns; extending into bilateral sylvian fissures; causing mass effect on midbrain and pons (Right > Left) |
| Tuberculomas | Few ring-enhancing conglomerated lesions in the right temporal cortex, ~2.3 x 2.5 x 2.7 cm; T1 hypointense, T2 heterogeneously hyperintense; diffusion restriction present; communicating with basal cisternal exudates |
| Skull Base Osteomyelitis | Abnormal enhancing marrow signal involving left occipital condyle, basilar part of occipital bone, and clivus; T1 hypointense, T2/FLAIR hyperintense; diffusion restriction present |
| Hypoglossal Canal Involvement | Soft tissue partially compromising the left hypoglossal canal; focal extension to lateral margin of foramen magnum |
| Leptomeningitis | Bilateral cerebral and cerebellar hemispheric leptomeningeal enhancement with sulcal FLAIR hyperintensity |
| White Matter Changes | Multiple discrete FLAIR hyperintense foci in subcortical white matter of bilateral frontal and parietal lobes |
| No infarct / No hemorrhage | No acute infarct or intracranial hemorrhage identified |
| No midline shift | Midline maintained |
| Basal ganglia / brainstem | Appear normal |
| Dural venous sinuses | Normal opacification; left sigmoid sinus and left IJV are hypoplastic |
MRI Impression (Official):
In a known case of CNS TB with skull base osteomyelitis:
- Non-communicating hydrocephalus with transependymal CSF ooze
- Right temporal tuberculomas (~2.3 x 2.5 x 2.7 cm) as described
- Diffuse tuberculous meningitis - thick enhancing basal cisternal exudates with diffuse leptomeningeal enhancement and mass effect
- Skull base osteomyelitis involving left occipital condyle, clivus, partially compromising left hypoglossal canal
Current Treatment
- On AKT (Anti-Koch's Treatment) - ongoing
Summary
Master Prem Vilas Pawar is a 13-year-10-month-old male, known case of CNS Tuberculosis with skull base osteomyelitis, currently on anti-tubercular therapy. He presented with a 1-month history of right frontal-parietal-temporal headache, intermittent vomiting, and new onset bilateral diplopia of 2 days duration. Investigations show normal liver and renal function, normal electrolytes, and HIV non-reactive status. MRI brain (07/07/2026) confirms active TB meningitis with basal cisternal exudates, right temporal tuberculomas, non-communicating hydrocephalus, and skull base osteomyelitis involving the left occipital condyle and clivus with partial involvement of the left hypoglossal canal - indicating ongoing CNS TB disease activity despite being on AKT.
Clinical Concern: The presence of hydrocephalus (Evan's index 0.37), mass effect on brainstem, and tuberculoma formation despite being on AKT raises the possibility of paradoxical worsening, inadequate drug penetration, or drug resistance - requiring urgent reassessment of the treatment regimen and neurosurgical evaluation for hydrocephalus management.


1000013531.jpg
1000013533.jpg
Give short point's
Here are the short points from both documents:
Patient
- Name: Prem Vilas Pawar
- Age: 13 yrs 10 months | Sex: Male
- Hospital: KEM Hospital, Parel, Mumbai
- Date: 13-Apr-2026
Chief Complaints
- Headache since 1 month (Rt. frontal + parietal + temporal)
- Vomiting - intermittent
- Diplopia (double vision) both eyes since 2 days
Negative History
- No weakness in limbs
- No limb pain episodes
- No neck rigidity
- No cough
Examination
- Power 5/5 all limbs
Investigations
Outside MRI (8th April):
- ? Skull base osteomyelitis
- ? Occipital lobe involvement
- Associated leptomeningeal enhancement
Sputum PCR: MTB not detected
Blood Reports:
- OT/PT: 42/44 U/L (normal)
- BUN/Creatinine: 6.5/0.8 (normal)
- Na/K: 138/4.4 (normal)
- HIV: Non-Reactive
MRI Brain (KEM - 07/07/2026) Findings
- Hydrocephalus - non-communicating, Evan's index 0.37 with periventricular ooze
- Thick basal cisternal exudates - suprasellar, interpeduncular, prepontine, ambient, quadrigeminal cisterns + bilateral sylvian fissures
- Mass effect on midbrain and pons (Rt > Lt)
- Tuberculoma - right temporal cortex (~2.3 x 2.5 x 2.7 cm), ring enhancing, diffusion restriction
- Skull base osteomyelitis - left occipital condyle + clivus, T2/FLAIR hyperintense
- Left hypoglossal canal - partially compromised by soft tissue
- Diffuse leptomeningeal enhancement - bilateral cerebral + cerebellar hemispheres
- Subcortical white matter FLAIR foci - bilateral frontal + parietal lobes
- No infarct, no hemorrhage, no midline shift
- Left sigmoid sinus + left IJV - hypoplastic
MRI Impression
- Non-communicating hydrocephalus with CSF ooze
- Right temporal tuberculoma
- Tuberculous meningitis - diffuse basal exudates
- Skull base osteomyelitis
Current Status
- Known case of CNS TB + Skull base osteomyelitis
- On AKT (Anti-Koch's Treatment)
- Presenting with occasional headache on follow-up
This is a shared conversation. Sign in to Orris to start your own chat.