Orris i need to learn about placenta it's development and parts like chorionic fundosum etc everything with reference pictures teach me
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have everything I need. Let me compile a comprehensive, well-structured lesson on placenta development with all the images.
The Placenta - Complete Guide with Illustrations
Sources: The Developing Human: Clinically Oriented Embryology (Moore & Persaud) + Histology: A Text and Atlas (Ross & Pawlina)
1. What is the Placenta?
The placenta is a fetomaternal organ - meaning it is built from BOTH fetal and maternal tissues working together. It is a disc-shaped structure that serves as the lifeline between mother and fetus, performing the functions of the lungs, intestines, kidneys, and liver all at once.
Two components:
- Fetal part - derived from the chorionic sac (outermost fetal membrane)
- Maternal part - derived from the decidua (endometrium of the pregnant uterus)
At term, the placenta:
- Covers 15-30% of the decidua
- Weighs ~1/6 of the fetus
- Uses 40-60% of oxygen and glucose reaching the uterus for its own metabolism
2. The Decidua (Maternal Side)
The decidua is the endometrium of the uterus during pregnancy. It is divided into three named regions based on their position relative to the implanted embryo:
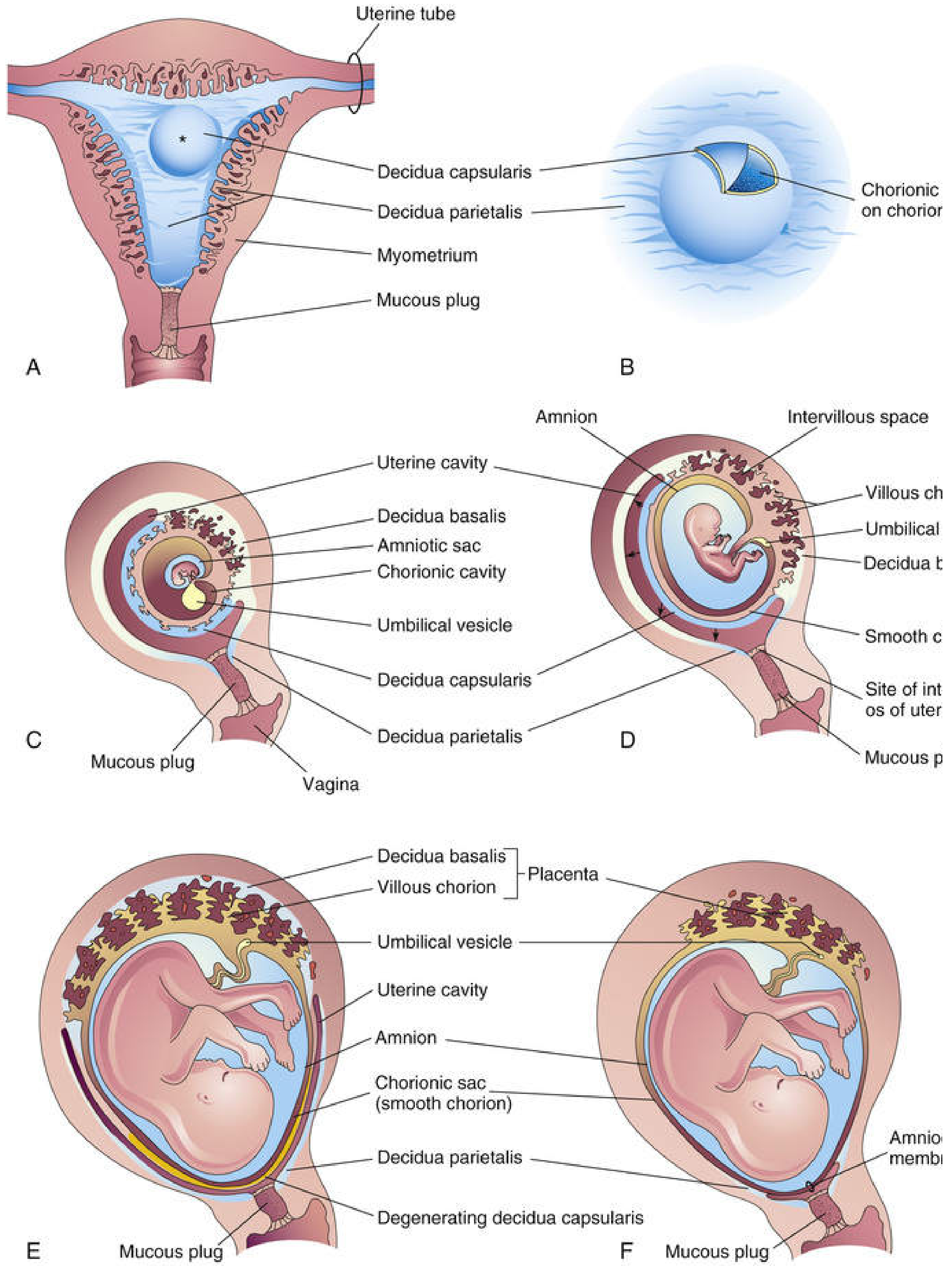
Fig. 7.1 - Development of the placenta and fetal membranes (Moore & Persaud). The diagrams A-F show the changing relations of the fetal membranes to the decidua from weeks 4 to 22.
| Region | Location | Fate |
|---|---|---|
| Decidua basalis | Deep to the conceptus | Forms maternal part of placenta |
| Decidua capsularis | Superficial, overlying the conceptus | Degenerates by weeks 22-24 as blood supply is cut off |
| Decidua parietalis | All remaining endometrium | Fuses with decidua capsularis eventually, obliterating uterine cavity |
Decidual reaction: In response to progesterone, connective tissue cells enlarge and accumulate glycogen/lipid to form decidual cells. Many degenerate near the chorionic sac, providing rich nutrition for the early embryo via the syncytiotrophoblast.
3. Development of the Placenta - Timeline
Early Formation (Weeks 2-3)
The uteroplacental circulation begins around day 9 after fertilization. The syncytiotrophoblast (outer trophoblast layer) erodes maternal capillaries, forming fluid-filled spaces called trophoblastic lacunae. Maternal sinusoids drain into these lacunae, establishing a primitive circulation driven by arteriovenous pressure differences.
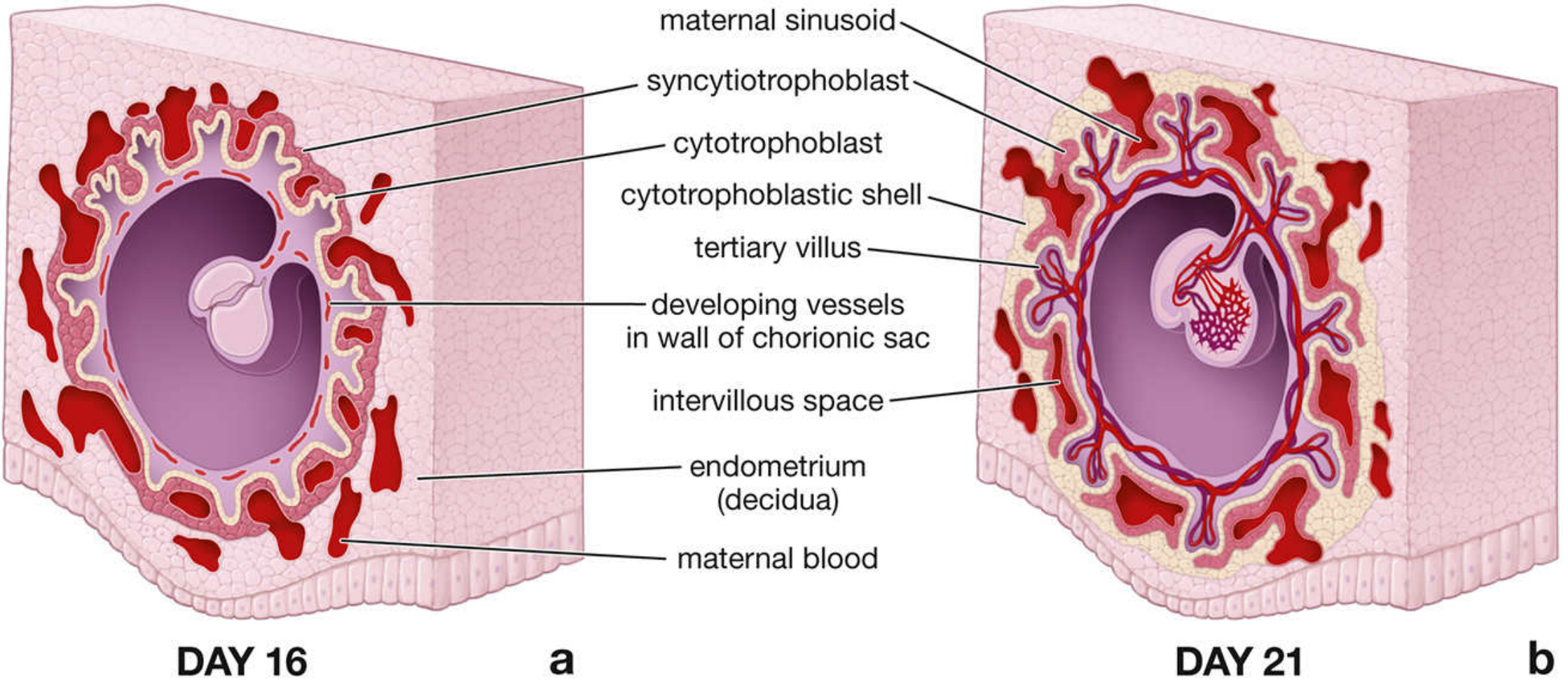
Fig. 23.25 - Early uteroplacental circulation at Day 16 and Day 21 (Histology: Ross & Pawlina). Note the maternal sinusoids draining into the intervillous space, and the developing cytotrophoblastic shell.
Weeks 3-8: Chorionic Villi Formation
Chorionic villi initially cover the entire chorionic sac. They then undergo a critical divergence:
- Villi covering the decidua capsularis get compressed and lose blood supply → they degenerate → form the smooth chorion (chorion laeve) - a bare, avascular area
- Villi covering the decidua basalis rapidly proliferate and branch profusely → form the villous chorion (chorion frondosum) - the bushy, functional area
Note on your question: The term is chorion frondosum (not "fundosum") - from Latin frondosus meaning "leafy/bushy." It is the fetal component of the placenta.
4. The Two Parts of the Placenta
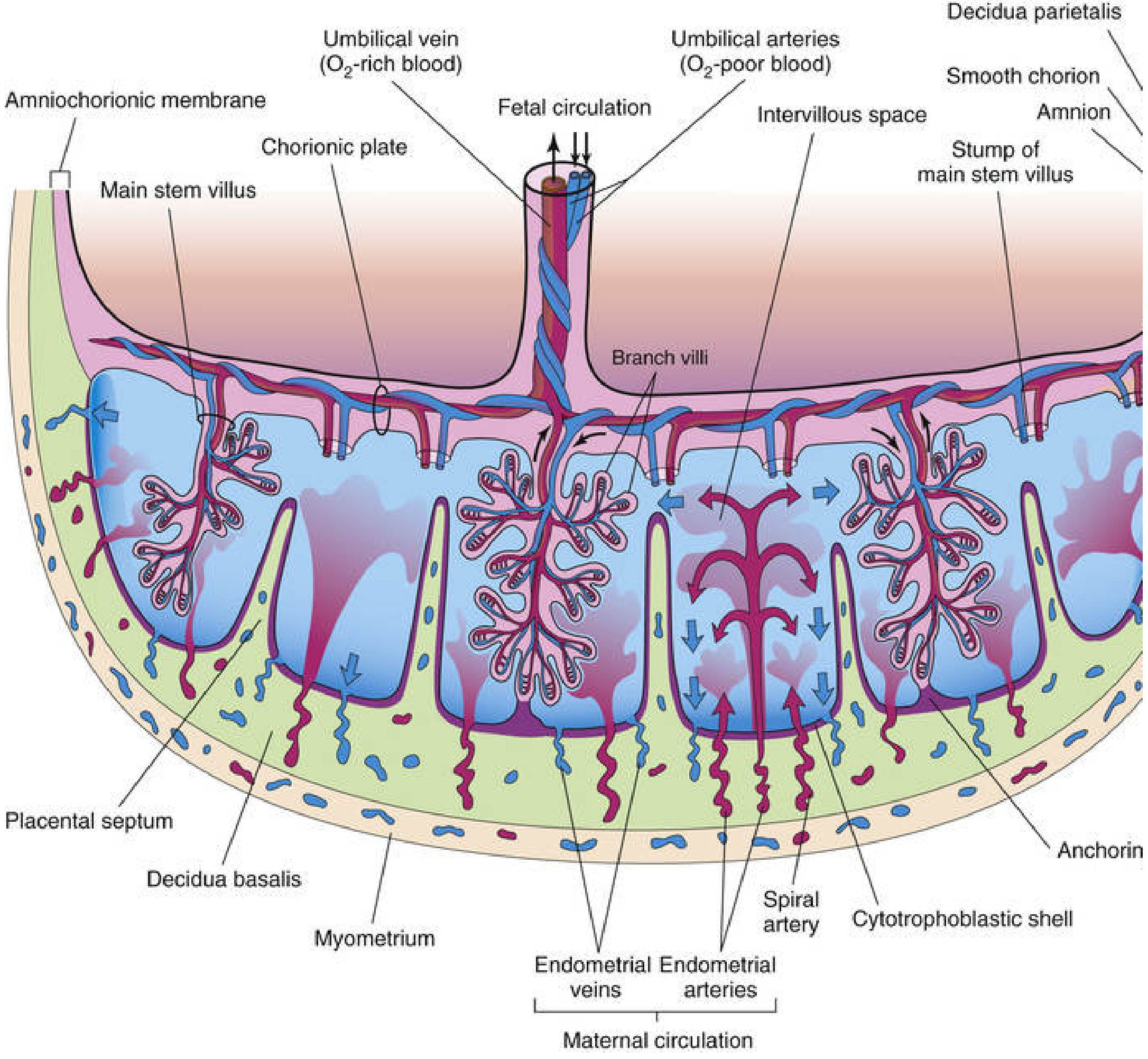
Fig. 7.5 - Transverse section through a full-term placenta (Moore & Persaud). This is one of the most important diagrams to understand the entire placenta at once.
Fetal Part: Villous Chorion (Chorion Frondosum)
- Made of chorionic villi projecting into the intervillous space
- Attached to the maternal side via the cytotrophoblastic shell
- Connected to the fetus via the umbilical cord
- The fetal surface is covered by the chorionic plate, onto which the umbilical vessels arrive and branch out
Maternal Part: Decidua Basalis
- By the end of the 4th month, almost entirely replaced by fetal cotyledons
- Eroded decidual tissue forms placental septa - wedge-shaped partitions that project inward toward the chorionic plate, dividing the placenta into 15-30 cotyledons
5. Chorionic Villi - Development Stages
The chorionic villi are the functional units of the placenta. They develop in three distinct stages:
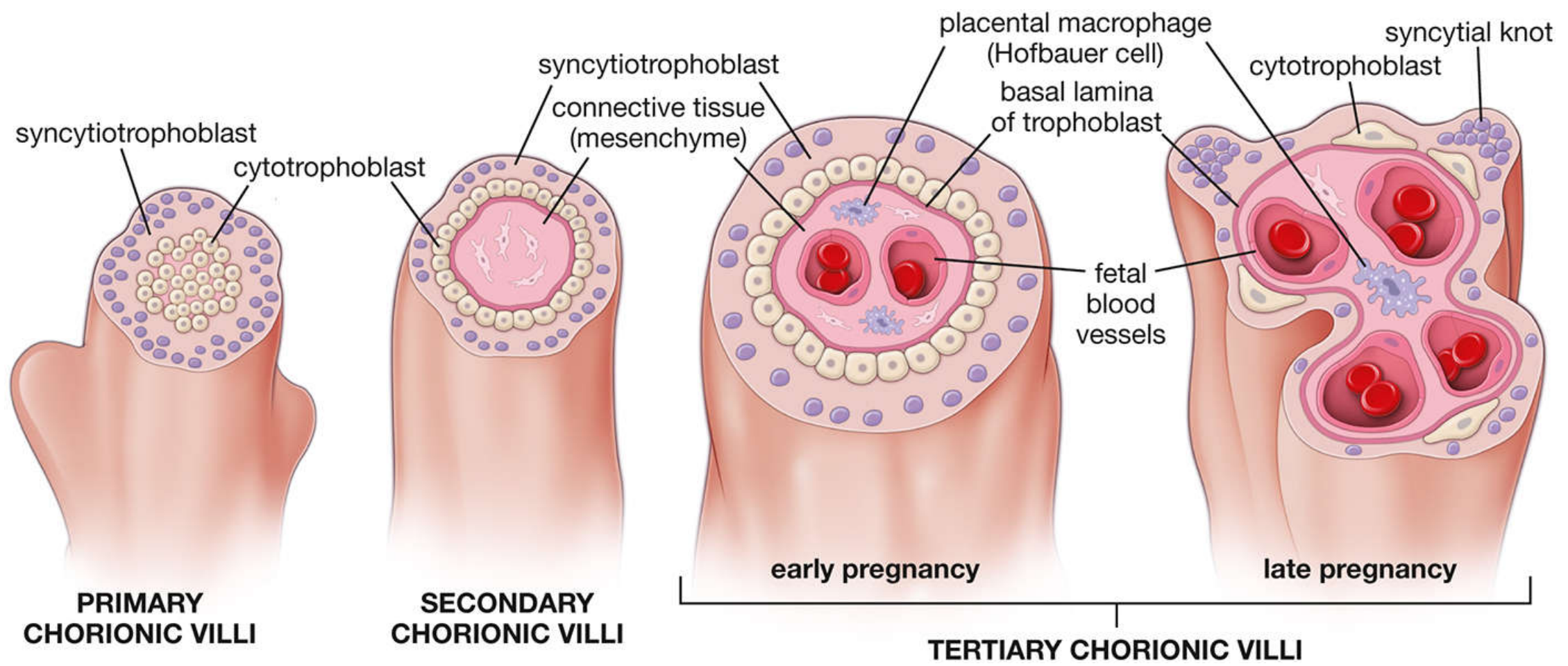
Fig. 23.26 - Developmental stages of chorionic villi (Ross & Pawlina). This single diagram summarizes all three stages beautifully.
Primary Chorionic Villi (Week 2)
- Finger-like extensions of syncytiotrophoblast + cytotrophoblast
- No blood vessels yet
- Appear around day 13
Secondary Chorionic Villi (~Day 16)
- Primary villi become invaded by extraembryonic mesenchyme (loose connective tissue)
- Structure: outer syncytiotrophoblast → inner cytotrophoblast → central mesenchymal core
- Cover the entire surface of the chorionic sac
Tertiary Chorionic Villi (End of Week 3 onward)
- Blood vessels develop within the mesenchymal core
- Hofbauer cells (fetal macrophages) are present in the connective tissue - they are phagocytic and involved in placental development and immunity
- Two subtypes appear:
- Free (floating) villi - remain suspended in the intervillous space, primary site of exchange
- Anchoring (stem) villi - attach firmly to the decidua basalis and form the structural framework
In late pregnancy, villi become smaller, the cytotrophoblast layer becomes discontinuous, and syncytiotrophoblast nuclei cluster into syncytial knots - their number increases with gestational age and is used to evaluate villous maturity.
6. Histology of the Placenta
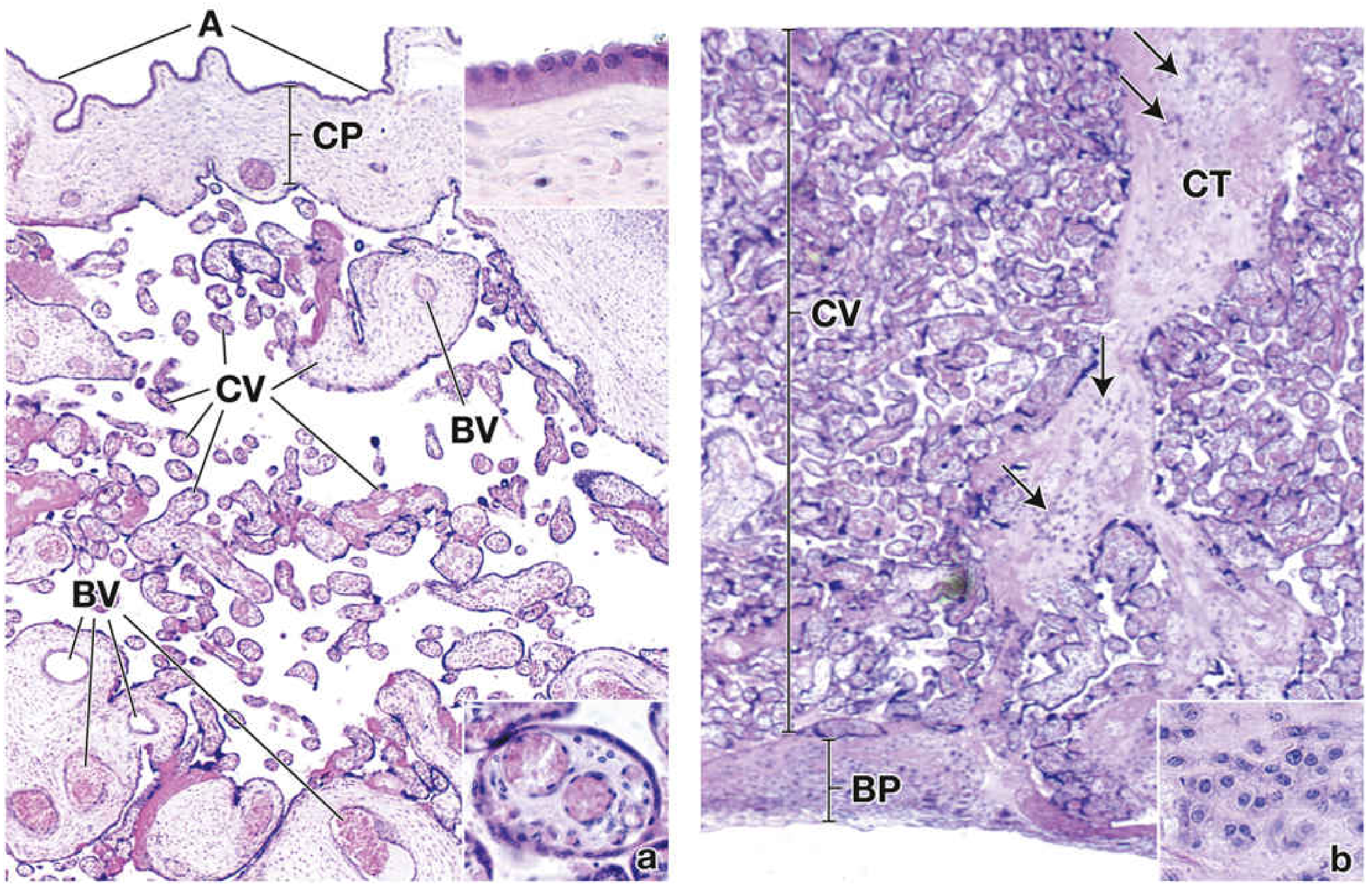
Fig. 23.27 - H&E histology of the placenta (Ross & Pawlina). Left (a): fetal side with chorionic plate and villi. Right (b): maternal side showing basal plate and decidual cells (arrows).
Key histological features:
- Amniotic epithelium (A): simple cuboidal epithelium lining the amnion
- Chorionic plate (CP): connective tissue base from which stem villi emerge
- Chorionic villi (CV): varying sizes - large stem villi contain major vessels, small terminal villi have only capillaries
- Basal plate (BP): maternal side, contains decidual cells (large, pale, glycogen-filled cells)
- Intervillous space: filled with maternal blood - the space between villi
7. Placental Circulation
Fetal (Villous) Circulation
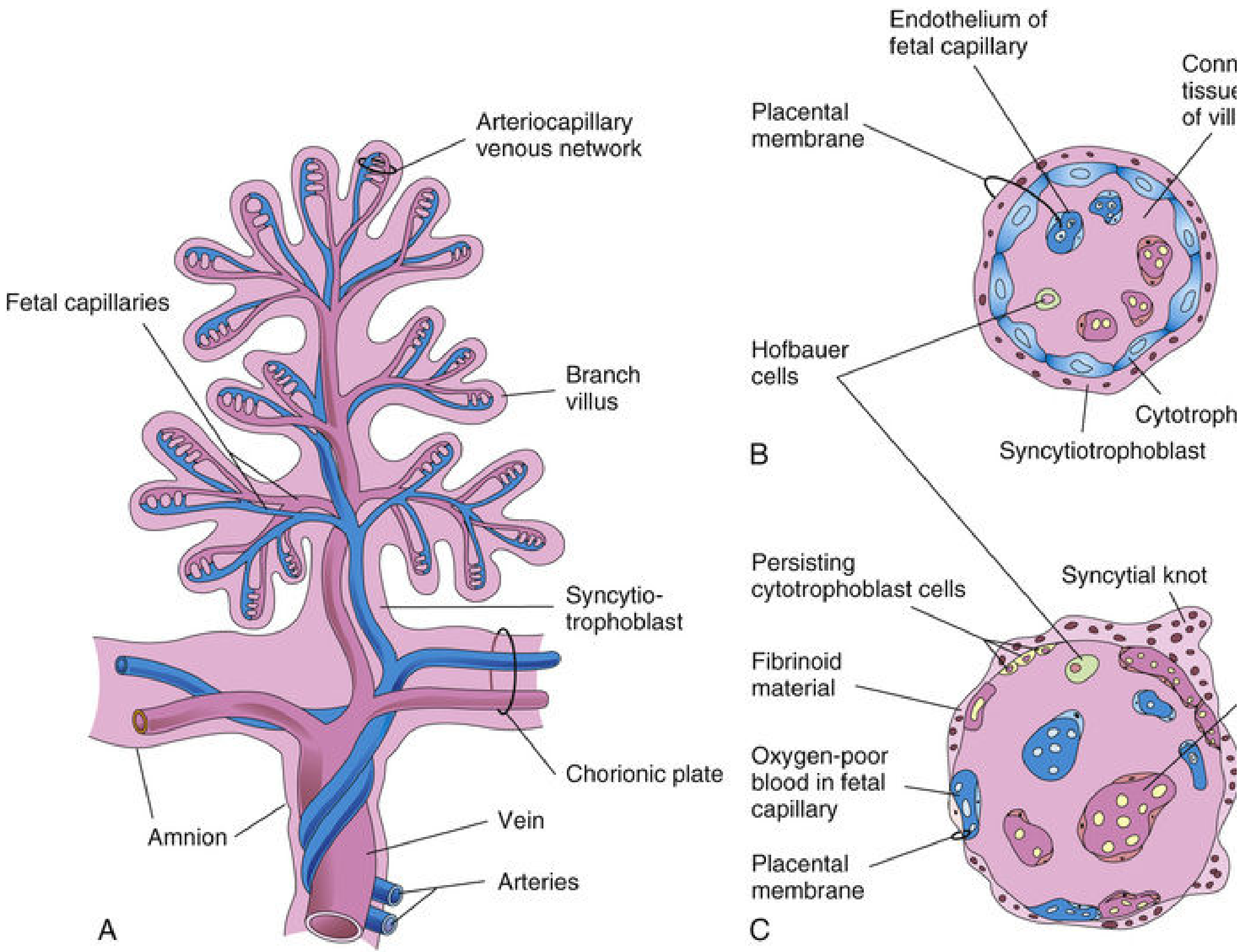
Fig. 7.6 - Fetal villous circulation and placental membrane (Moore & Persaud).
Flow: Umbilical arteries (deoxygenated blood) → chorionic arteries in chorionic plate → radially branch into villi → arteriocapillary-venous network within villi (exchange occurs here) → thin-walled veins → umbilical vein (oxygenated blood back to fetus)
Maternal (Intervillous) Circulation
Flow: 80-100 spiral endometrial arteries in decidua basalis → discharge through gaps in cytotrophoblastic shell → spurt toward chorionic plate → slow flow over branch villi (exchange) → drain via endometrial veins back to maternal circulation
- The intervillous space at term contains ~150 mL of blood, replenished 3-4 times per minute
- Spiral artery flow is pulsatile
- Blood enters at higher pressure, spurts toward chorionic plate, then slows for exchange
Critical principle: Fetal and maternal blood do NOT mix under normal conditions. They are separated by the placental membrane. Exchange occurs by diffusion and active transport.
8. The Placental Membrane (the "Barrier")
The placental membrane separates maternal blood in the intervillous space from fetal blood in the capillaries. It is composed of extrafetal tissues:
Before 20 weeks (4 layers):
- Syncytiotrophoblast (outer)
- Cytotrophoblast
- Connective tissue of villi
- Endothelium of fetal capillaries (inner)
After 20 weeks (3 layers):
Cytotrophoblast becomes attenuated/disappears over large areas, leaving only syncytiotrophoblast + connective tissue + capillary endothelium.
In some areas a vasosyncytial membrane forms where syncytiotrophoblast directly contacts capillary endothelium - this maximizes exchange efficiency near term.
The term "placental barrier" is misleading - most substances (drugs, hormones, toxins) CROSS the membrane. True barriers exist only for very large molecules (e.g., heparin) or certain charged molecules.
Syncytial knots: In the 3rd trimester, syncytiotrophoblast nuclei aggregate into multinucleated protrusions that regularly break off into maternal blood. They lodge in maternal pulmonary capillaries and are rapidly destroyed there.
9. Cotyledons
The placenta is divided into 15-30 cotyledons (convex lobular units) by placental septa. Each cotyledon consists of:
- 2 or more stem villi (main structural units)
- Many branch villi (functional exchange units)
The septa project from the decidua basalis toward the chorionic plate but do NOT reach it, so there is free communication between cotyledons through the intervillous space.
10. Functions of the Placenta
| Function | Details |
|---|---|
| Respiration | O₂ and CO₂ exchange between maternal and fetal blood |
| Nutrition | Glucose, amino acids, fatty acids, vitamins transferred to fetus |
| Excretion | Fetal waste (urea, CO₂, bilirubin) passed to maternal blood |
| Protection | Immune protection; some pathogens and drugs blocked |
| Metabolism | Synthesizes glycogen, cholesterol, fatty acids (especially early pregnancy) |
| Endocrine | Secretes hCG, progesterone, estrogen, hPL (human placental lactogen), relaxin |
Key Hormones
- hCG (human chorionic gonadotropin): secreted by syncytiotrophoblast; maintains corpus luteum in early pregnancy; basis of pregnancy test
- Progesterone: maintains uterine decidua; prevents myometrial contractions
- Estrogens: promote uterine and breast growth
- hPL (human placental lactogen): alters maternal metabolism to ensure fetal nutrition
- Relaxin: loosens ligaments of pelvis for delivery
11. Amniochorionic Membrane
As the amniotic sac expands faster than the chorionic sac, the amnion fuses with the smooth chorion to form the amniochorionic membrane. This then fuses with the decidua parietalis. It is this membrane that ruptures during labor ("waters breaking"). Premature rupture (< 37 weeks) is the most common event leading to premature labor.
Summary Diagram - Key Structures at a Glance
| Structure | What it is |
|---|---|
| Chorion frondosum | Bushy fetal chorion - fetal part of placenta |
| Chorion laeve | Smooth chorion - avascular area away from placenta |
| Decidua basalis | Maternal endometrium forming maternal placenta |
| Decidua capsularis | Endometrium overlying the conceptus (degenerates) |
| Decidua parietalis | Rest of endometrium |
| Chorionic plate | Fetal side of placenta, base for stem villi |
| Basal plate | Maternal side of placenta |
| Intervillous space | Blood-filled space between villi (maternal blood) |
| Cotyledon | Lobule of placenta separated by placental septa |
| Placental septa | Partitions from decidua basalis into intervillous space |
| Cytotrophoblastic shell | Outer anchoring layer of trophoblast cells |
| Spiral arteries | Maternal arteries feeding intervillous space |
| Umbilical arteries (×2) | Carry deoxygenated fetal blood to placenta |
| Umbilical vein (×1) | Carries oxygenated blood from placenta to fetus |
| Hofbauer cells | Fetal macrophages inside villi stroma |
| Syncytial knots | Aggregated nuclei in syncytiotrophoblast, increase with age |
| Vasosyncytial membrane | Thinned exchange area (syncytio + capillary endothelium only) |
References:
- The Developing Human: Clinically Oriented Embryology (Moore, Persaud & Torchia), Chapter 7 - Placenta and Fetal Membranes
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina), Chapter 23 - Female Reproductive System
This is a shared conversation. Sign in to Orris to start your own chat.