Give me 10 marks lAq on meconium aspiration syndrome make this exam ready and simple
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is your complete, exam-ready 10-mark LAQ on Meconium Aspiration Syndrome:
MECONIUM ASPIRATION SYNDROME (MAS)
10-Mark Long Answer Question
DEFINITION
Meconium Aspiration Syndrome (MAS) is a clinical diagnosis defined as respiratory distress in a neonate born through meconium-stained amniotic fluid (MSAF), with a characteristic chest X-ray appearance, where symptoms cannot be explained by another cause. Confirmation requires the presence of meconium below the level of the vocal cords.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1789
INCIDENCE / EPIDEMIOLOGY
| Fact | Value |
|---|---|
| MSAF incidence at delivery | 4% - 22% of all deliveries |
| MAS complicating MSAF | ~1% - 2% of MSAF deliveries |
| More common in | Post-term / post-mature infants (>42 weeks) |
| Need for mechanical ventilation | ~30% of affected infants |
- Intrauterine meconium passage is rare before 36 weeks (immature myenteric plexus)
- Occurs more frequently with post-term gestation
PATHOPHYSIOLOGY
MAS is now understood to be multifactorial - not simply due to airway obstruction alone.
Four Key Mechanisms:
1. Airway Obstruction (Ball-Valve Effect)
- Meconium is a thick, viscous substance that migrates to distal airways
- Complete obstruction → segmental atelectasis
- Partial obstruction → "ball-valve" effect → air trapping and hyperinflation
- Alternating areas of atelectasis and overinflation on CXR
2. Chemical Pneumonitis
- Meconium causes direct chemical irritation of lung parenchyma
- Leads to inflammation, edema, and lung injury
3. Surfactant Inactivation
- Meconium inactivates existing surfactant
- Worsens ventilation-perfusion mismatch and respiratory failure
4. Pulmonary Hypertension (PPHN)
-
Alterations in pulmonary vasculature lead to persistently elevated pulmonary vascular resistance
-
Right-to-left shunting across PDA and foramen ovale worsens hypoxemia
-
PPHN is the most serious complication of MAS
-
Grainger & Allison's Diagnostic Radiology, p. 1765; Creasy & Resnik's Maternal-Fetal Medicine, p. 1789
CLINICAL FEATURES
History / Risk Factors:
- Post-term pregnancy (>42 weeks)
- Non-reassuring fetal heart rate tracings
- Fetal distress / perinatal asphyxia
- MSAF noted at delivery
Clinical Presentation (appear within minutes to hours of birth):
- Respiratory distress: tachypnea, grunting, nasal flaring, subcostal retractions
- Barrel-shaped chest (due to hyperinflation)
- Cyanosis
- Low Apgar scores
- Greenish/yellow staining of skin, nails, umbilical cord (from meconium)
- Diminished or asymmetric breath sounds
Severe Disease hallmarks:
- Need for positive-pressure ventilation
- Presence of pulmonary hypertension
INVESTIGATIONS
1. Chest X-Ray (CXR) - Key Investigation
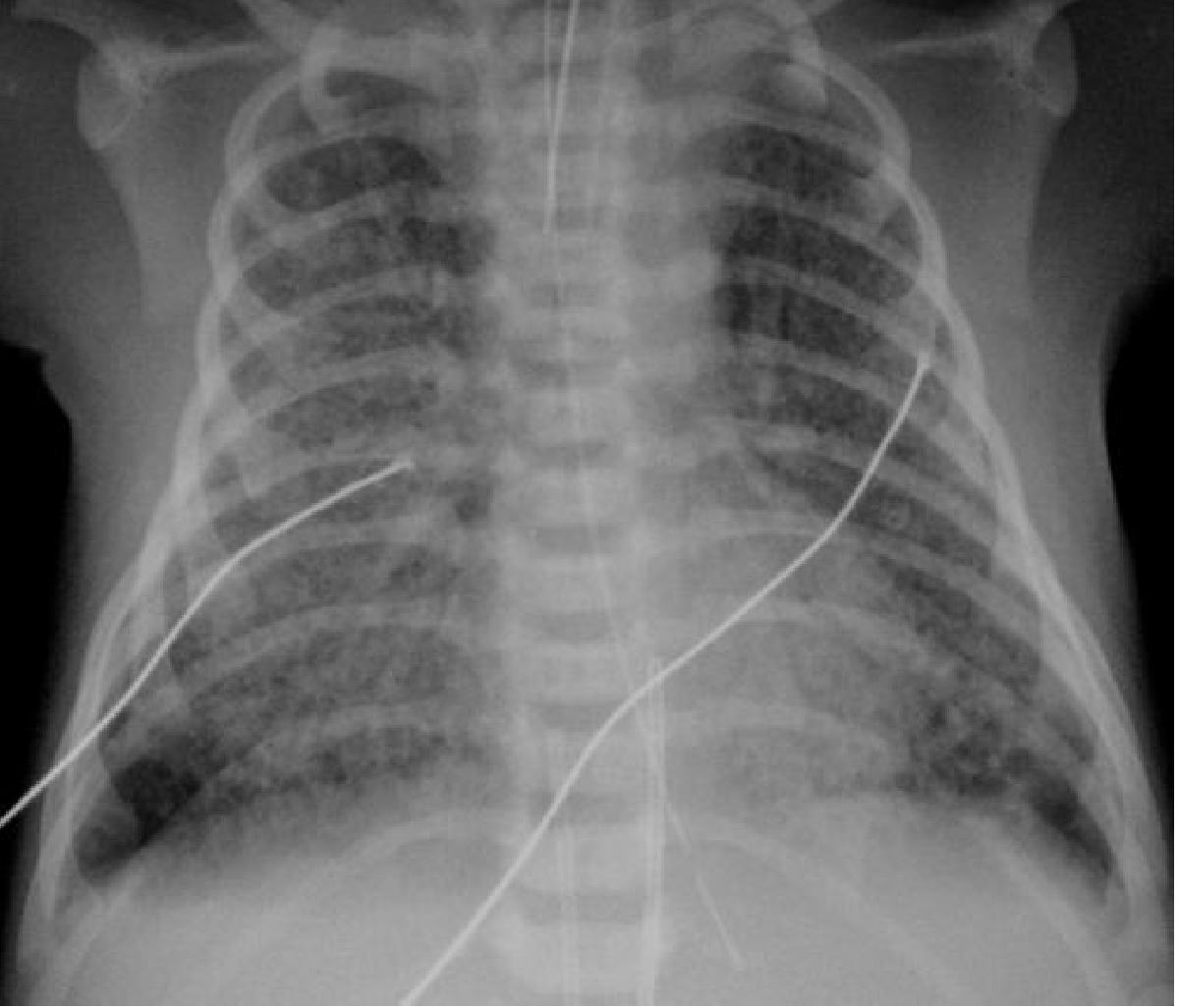
CXR findings in MAS: Bilateral hyperinflation with asymmetrical coarse patchy opacification and small pleural effusion - Grainger & Allison's Diagnostic Radiology
Classic CXR findings:
- Bilateral hyperinflation (flattened diaphragms)
- Coarse, irregular patchy opacities (asymmetrical)
- Areas of atelectasis alternating with overinflation
- Small pleural effusions (may be present)
- Pneumothorax (common complication - air leak)
2. Blood Gas (ABG): Hypoxemia, hypercapnia, metabolic/respiratory acidosis
3. Echocardiography: To assess for PPHN, right heart strain, shunting
4. Blood counts / cultures: To exclude sepsis (neonatal pneumonia can mimic MAS)
COMPLICATIONS
| Complication | Notes |
|---|---|
| Persistent Pulmonary Hypertension (PPHN) | Most serious; right-to-left shunting |
| Pneumothorax / Pneumomediastinum | "Air leak" due to ball-valve trapping |
| Chronic lung disease | Long-term morbidity |
| Developmental delay | In severe cases |
| Death | Mortality improved with modern therapies |
MANAGEMENT
A. Preventive Strategies (Antenatal/Intrapartum)
- Induction of labor at 41 weeks to prevent post-term MSAF (evidence-based; reduces MAS and C-section rates)
- Amnioinfusion - diluting thick meconium did NOT reduce MAS in settings with adequate surveillance (not routinely recommended)
- Routine intrapartum oropharyngeal suctioning - no longer recommended (2004 RCT showed no benefit)
B. Delivery Room Management
Current Guidelines (ILCOR/AAP 2015 and updated):
- Routine endotracheal intubation and suctioning is NO LONGER recommended for either vigorous or depressed infants born through MSAF
- Reason: RCTs showed no difference in MAS incidence, mechanical ventilation need, or mortality with tracheal suctioning
- Delay in positive-pressure ventilation causes more harm than benefit
- Skilled personnel should attend delivery; initiate PPV if infant is depressed
Key Exam Point: The practice of routine tracheal suctioning for all MSAF infants was abandoned after landmark trials (Wiswell 2000, followed by ILCOR 2015 update)
C. NICU Management (Supportive & Targeted)
1. Respiratory Support:
- Supplemental oxygen
- CPAP or mechanical ventilation as needed
- High-frequency oscillatory ventilation (HFOV) for refractory cases
- Avoid high peak inspiratory pressures (risk of air leak)
2. Surfactant Therapy:
- Early exogenous surfactant administration is a useful treatment modality
- Counteracts surfactant inactivation by meconium
3. Management of PPHN (Pulmonary Hypertension):
- Inhaled Nitric Oxide (iNO) - selective pulmonary vasodilator; first-line for PPHN in MAS
- Sildenafil - oral/IV pulmonary vasodilator
- Bosentan - endothelin receptor antagonist
- These agents improve oxygenation and allow less injurious ventilator strategies
4. ECMO (Extracorporeal Membrane Oxygenation):
- Used when conventional treatment fails
- VA-ECMO (veno-arterial): bypasses lungs when PVR is very high; catheter via internal jugular vein + common carotid artery
- VV-ECMO (veno-venous): double-lumen catheter via internal jugular vein; for gas exchange alone
- Allows physiological oxygen saturation while lungs recover
5. Antibiotics and Steroids:
- Selectively used; no demonstrated effectiveness in clinical trials
6. General Supportive Care:
- Maintain normothermia, normoglycemia, blood pressure
- Treat underlying asphyxia
PROGNOSIS
- Mortality has significantly improved with iNO, ECMO, and better neonatal care
- Severe disease associated with: chronic lung disease, air leak, developmental delay
- Incidence of MAS has declined in recent years due to better obstetric surveillance and abandonment of routine tracheal suctioning
QUICK SUMMARY TABLE (Exam-Friendly)
| Feature | Key Point |
|---|---|
| Definition | Respiratory distress in MSAF baby + CXR changes |
| Incidence | 1-2% of MSAF deliveries; more in post-term |
| Pathophysiology | Obstruction + pneumonitis + surfactant inactivation + PPHN |
| Key complication | PPHN (most serious) |
| CXR findings | Hyperinflation + coarse patchy opacities + air leaks |
| Delivery room | NO routine tracheal suction (ILCOR 2015) |
| PPHN treatment | Inhaled Nitric Oxide (first-line) |
| Last resort | ECMO |
Sources: Creasy & Resnik's Maternal-Fetal Medicine (9e); Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.