Assignment hysterectomy
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Searching Images
hysterectomy types abdominal vaginal laparoscopic uterus anatomy
Hysterectomy — Nursing Assignment
1. Definition
Hysterectomy is the surgical removal of the uterus. It is one of the most commonly performed major gynecological surgeries. Depending on the extent of removal and the surgical route, it may also include removal of the cervix, fallopian tubes, and/or ovaries.
2. Anatomy Relevant to Hysterectomy
The uterus lies in the pelvis between the bladder anteriorly and the rectum posteriorly. Key anatomical structures involved during hysterectomy include:
| Structure | Relevance |
|---|---|
| Round ligaments | First ligaments divided in abdominal hysterectomy |
| Broad ligament (anterior & posterior leaves) | Incised to access uterine vessels |
| Infundibulopelvic ligament | Contains ovarian vessels; divided if oophorectomy is performed |
| Uterine artery | Ligated at level of internal cervical os |
| Cardinal ligaments | Support the cervix laterally; clamped and divided |
| Uterosacral ligaments | Provide apical support; incorporated into vaginal cuff closure |
| Ureter | Runs within the broad ligament ~2 cm lateral to the cervix — at high risk of injury |
| Bladder | Lies anterior to lower uterine segment; must be dissected off the cervix |
— Gray's Anatomy for Students; Sabiston Textbook of Surgery, 21st ed.
3. Indications
| Indication | Notes |
|---|---|
| Uterine leiomyomas (fibroids) | Most common indication (~195,000/year in the US); only for symptomatic patients who do not desire future fertility |
| Abnormal uterine bleeding (AUB) | After medical therapy fails; endometrial sampling required before surgery |
| Endometriosis / Adenomyosis | Especially useful when childbearing is complete; pelvic pain relief in ~77% |
| Pelvic organ prolapse | ~74,000/year; increasingly replaced by uterus-sparing hysteropexy |
| Gynecologic cancers | Endometrial, cervical, ovarian (~53,000/year); may require radical hysterectomy |
| Benign ovarian neoplasms | ~70,000/year |
| Chronic pelvic pain | Only when other correctable pathology has been excluded and ≥6 months of pain persists |
Key principle: Hysterectomy for leiomyomas should only be performed in symptomatic patients who have completed childbearing. — Berek & Novak's Gynecology, 16th ed.
4. Types of Hysterectomy
A. By Extent of Tissue Removed
| Type | What is Removed |
|---|---|
| Total hysterectomy | Uterine body + cervix (most common) |
| Subtotal / Supracervical hysterectomy | Uterine body only; cervix preserved |
| Radical hysterectomy (Wertheim's) | Uterus + cervix + upper vagina + parametrium + pelvic lymph nodes; for malignancy |
| Hysterectomy + BSO (bilateral salpingo-oophorectomy) | Uterus + both fallopian tubes + both ovaries |
| Hysterectomy + opportunistic salpingectomy | Uterus + fallopian tubes only; ovaries preserved to reduce cardiovascular risk |
Salpingo-oophorectomy in premenopausal women at average risk for ovarian malignancy is associated with increased long-term mortality from cardiovascular disease; ovarian conservation should be strongly considered. — Berek & Novak's Gynecology
B. By Surgical Approach
| Route | Description | Advantages |
|---|---|---|
| Total Abdominal Hysterectomy (TAH) | Open laparotomy via low transverse (Pfannenstiel) or vertical midline incision | Best access for large uteri, malignancy, adhesions |
| Vaginal Hysterectomy (VH) | Uterus removed through the vagina | No abdominal incision; shorter hospital stay; preferred route if feasible |
| Laparoscopic Hysterectomy (LH) | Minimally invasive through small ports; specimen removed vaginally | Less postoperative pain, faster recovery, shorter stay |
| Robotic-Assisted Laparoscopic Hysterectomy | Laparoscopic with robotic system (da Vinci); less blood loss, fewer conversions | Greater cost; similar outcomes to laparoscopic |
Vaginal hysterectomy is the procedure of choice unless contraindicated. Abdominal hysterectomy should be reserved for cases where vaginal or laparoscopic approaches are not feasible. — Berek & Novak's Gynecology
5. Surgical Steps (Total Abdominal Hysterectomy)
The key steps are illustrated below from Sabiston Textbook of Surgery:
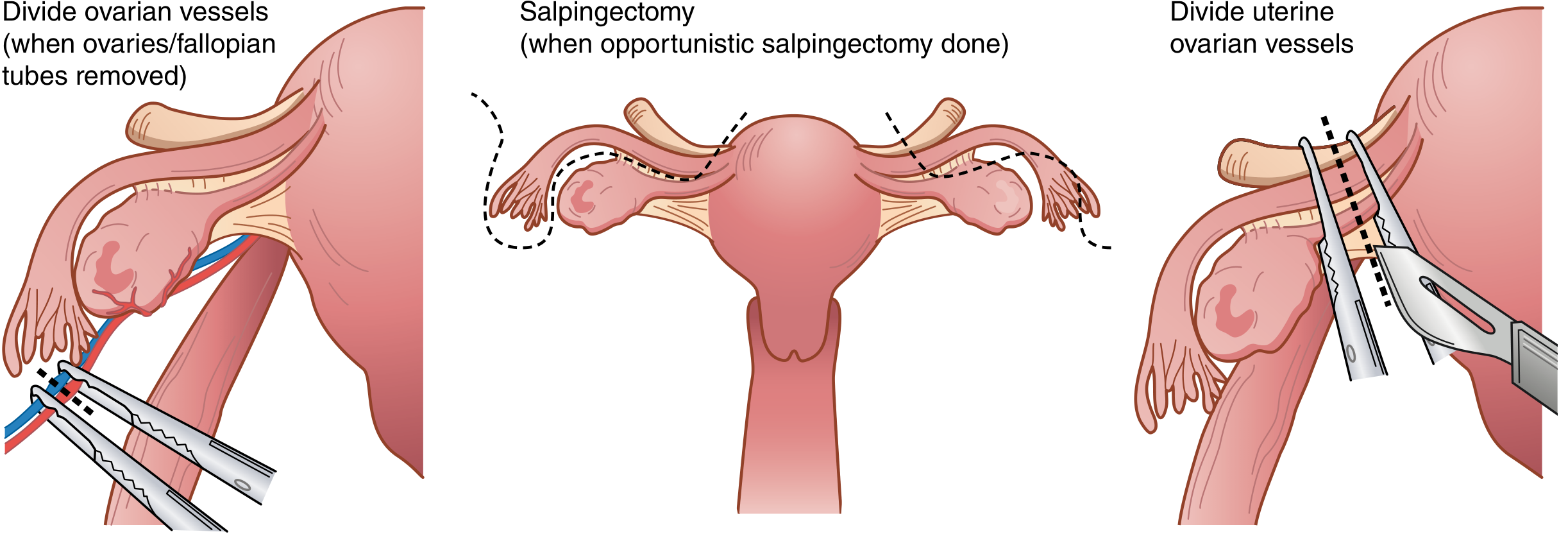
Step-by-step overview:
- Laparotomy — low transverse (Pfannenstiel) or vertical midline incision
- Exploration — identify uterus, tubes, ovaries, and any pathology
- Divide round ligaments — bilaterally with electrocautery or suture ligation
- Incise broad ligament — anterior leaf medially to develop the bladder flap
- Manage adnexa — if BSO: divide infundibulopelvic ligaments after identifying ureters; if ovaries retained: divide utero-ovarian vessels
- Bladder dissection — dissect bladder off the cervix with Metzenbaum scissors
- Ligate uterine vessels — curved clamp placed at level of internal cervical os; pedicle cut and suture-ligated
- Divide cardinal and uterosacral ligaments — serial clamping and ligation bilaterally
- Colpotomy — incise vagina just below the cervix circumferentially
- Remove specimen
- Close vaginal cuff — running, interrupted, or figure-of-eight sutures; uterosacral ligaments incorporated for apical support
6. Preoperative Nursing Care
| Action | Rationale |
|---|---|
| Complete nursing assessment (history, allergies, vital signs) | Baseline data; identify risk factors |
| Confirm informed consent | Legal requirement; PREPARE mnemonic (Procedure, Reason, Expectation, nonsurgical Alternatives, Risks, Expense) |
| Pre-op investigations: CBC, blood group and crossmatch, coagulation, urinalysis, ECG, CXR | Detect anemia, coagulopathy, cardiac risk |
| Bowel preparation (if ordered) | Reduce risk of bowel injury contamination |
| Nil by mouth (NPO) 6–8 hours pre-surgery | Aspiration prevention |
| IV line insertion; urinary catheter insertion (Foley) | IV access for fluids/drugs; intraoperative bladder decompression |
| Skin preparation (abdomen, perineum) | Infection prevention |
| DVT prophylaxis: TED stockings ± LMWH | Hysterectomy patients have elevated VTE risk |
| Pre-operative antibiotics (within 60 min of incision) | Reduce surgical site infection |
| Emotional support and education | Reduce anxiety; explain loss of menstruation and fertility |
7. Intraoperative Nursing Responsibilities
- Correct patient and procedure identification (time-out/WHO checklist)
- Positioning: supine (TAH), lithotomy (VH/LH)
- Assist anaesthesia team — monitoring airway, IV access
- Maintain sterile field; handle instruments and swabs per hospital protocol
- Accurate swab, instrument, and needle count before and after surgery
- Document procedure, specimens sent (uterus to histopathology), intraoperative blood loss
- Ensure specimens are correctly labelled and sent to pathology
8. Postoperative Complications & Nursing Management
A. Hemorrhage
- Recognition: Excessive vaginal bleeding, tachycardia, hypotension, falling hematocrit, flank/abdominal pain, abdominal distention
- Types: Vaginal cuff bleeding (more visible) vs. retroperitoneal hemorrhage (insidious)
- Nursing actions:
- Monitor vital signs every 15–30 min; assess blood loss
- Maintain IV access; administer IV fluids and blood products as ordered
- Input and output monitoring
- Prepare for return to OT if hemorrhage is uncontrolled
- Berek & Novak's Gynecology
B. Urinary Tract Complications
| Complication | Signs | Nursing Action |
|---|---|---|
| Urinary retention | Inability to void after catheter removal | Re-catheterize for 12–24 h; reassess |
| Ureteral injury/obstruction | Flank pain, decreased urine output | Report immediately; CT urogram ordered; prepare for ureteric stenting or repair |
| Vesicovaginal fistula | Watery vaginal discharge 10–14 days post-op | Methylene blue tampon test; report to surgeon; surgical repair planned |
| UTI | Dysuria, fever, cloudy urine | Urine MC&S; antibiotics as ordered |
Urinary retention (post catheter removal) is usually due to pain or anesthesia-related bladder atony and is temporary.
C. Wound Infections
- Occur in ~2% of abdominal hysterectomies; lower with laparoscopic approach
- Monitor wound site for erythema, swelling, purulent discharge, dehiscence
- Maintain aseptic wound care; report signs of infection
- Administer antibiotics as ordered
D. Vaginal Cuff Dehiscence
- Rare but serious complication — separation of vaginal cuff suture line
- Presents with sudden pelvic pain and vaginal discharge/bleeding
- Requires urgent surgical repair
E. Prolapse of Fallopian Tube
- Rare; presents as persistent vaginal discharge/bleeding post-operatively
- Refer to gynecology
F. Deep Vein Thrombosis / Pulmonary Embolism
- Hysterectomy = significant VTE risk (major pelvic surgery)
- Prevention and management: Early ambulation (key!), TED stockings, LMWH (as prescribed), adequate hydration
- Monitor for leg pain, swelling, dyspnea, chest pain
G. Constipation / Ileus
- Post-op opioid use + reduced mobility → bowel slowing
- Stool softeners (docusate sodium), osmotic laxatives (polyethylene glycol), high fiber/fluid intake, early ambulation
9. Postoperative Nursing Care (General)
Immediate Post-op (Recovery Room)
| Assessment | Action |
|---|---|
| Airway, breathing, circulation | ABCDE assessment; oxygen therapy as needed |
| Vital signs | Hourly initially; detect bleeding or sepsis early |
| Pain assessment (numerical scale 0–10) | Administer analgesics per orders; IV acetaminophen, NSAIDs (ketorolac), opioids; aim for opioid-sparing approach |
| Urinary catheter | Ensure patency; monitor hourly urine output (target ≥0.5 mL/kg/h) |
| IV fluids | Maintain adequate hydration |
| Wound check | Observe dressing for bleeding or soakage |
| Nausea/vomiting | Antiemetics as ordered |
Ward (Post-op Days 1–3)
- Ambulation: Encourage as soon as possible (reduces DVT risk, aids recovery)
- Diet: Light diet as tolerated from day of surgery (laparoscopic) or next day (TAH); progress to normal diet
- Catheter removal: Usually day 1 (laparoscopic) or day 2 (TAH); ensure patient voids within 6 hours
- Pain: Transition to oral analgesics (paracetamol, NSAIDs, tramadol)
- Wound care: Daily inspection; Pfannenstiel wound closed with sutures/staples removed at 5–7 days
- Monitor for complications (see Section 8)
- Psychological support: Address grief/adjustment related to loss of reproductive organ, premature menopause if oophorectomy done
10. Discharge Instructions (Patient Education)
Nurses should educate the patient on:
- Rest: Avoid heavy lifting (>5 kg) and strenuous activity for 6 weeks
- Driving: Avoid until off opioids and can perform emergency stop (~2–4 weeks post VH/LH; ~4–6 weeks post TAH)
- Sexual activity: Avoid penetrative intercourse for 6–8 weeks until cuff heals
- Vaginal discharge: Expect light pink/brown discharge for 4–6 weeks; report heavy/bright red bleeding
- Bowel care: Use stool softeners/fiber; avoid straining
- When to seek urgent help:
- Excessive vaginal bleeding
- Fever (>38.5°C)
- Severe abdominal pain
- Inability to void
- Signs of DVT (leg swelling, pain) or PE (chest pain, dyspnea)
- Follow-up: First outpatient visit at 4–6 weeks post-surgery
- Menstruation: Will permanently cease post-hysterectomy
- Menopause: If ovaries removed, surgical menopause begins immediately — hormone replacement therapy may be discussed
11. Quality of Life Outcomes
- The majority of patients report significant improvement in pelvic pain, urinary symptoms, psychological well-being, and quality of life at 1–2 years post-hysterectomy (Maine Women's Health Study)
- Sexual function is unchanged or improved in the majority of women after hysterectomy
- ~8% of patients report persistent or new symptoms (depression, reduced libido) — nursing support and referral to psychology or sexual health services is important
- Berek & Novak's Gynecology, 16th ed.; Campbell-Walsh-Wein Urology
12. Summary Table
| Aspect | Key Points |
|---|---|
| Definition | Surgical removal of the uterus |
| Most common indication | Leiomyomas / AUB |
| Preferred route | Vaginal hysterectomy (if feasible) |
| Main complications | Hemorrhage, urinary injury, infection, DVT, cuff dehiscence |
| Key nursing priorities | Vital sign monitoring, pain control, early ambulation, urinary monitoring, wound care, patient education |
| Discharge | 1–3 days (LH/VH); 3–5 days (TAH); full recovery 4–6 weeks |
Sources: Berek & Novak's Gynecology, 16th ed.; Sabiston Textbook of Surgery, 21st ed.; Campbell-Walsh-Wein Urology, 12th ed.; Gray's Anatomy for Students, 4th ed.
Assignment hysterectomy
I just completed a full hysterectomy assignment for you above. Here's a quick summary of what's covered:
What's in Your Assignment
- Definition — what hysterectomy is
- Relevant Anatomy — uterus, ligaments, ureter, bladder relationships
- Indications — fibroids, AUB, endometriosis, prolapse, cancer, chronic pelvic pain
- Types — by extent (total, subtotal, radical, ± BSO) and by surgical route (TAH, vaginal, laparoscopic, robotic)
- Surgical Steps — step-by-step TAH technique with diagram
- Preoperative Nursing Care — assessment, consent, investigations, prep, DVT prophylaxis
- Intraoperative Nursing — WHO checklist, positioning, swab counts, specimen handling
- Postoperative Complications & Nursing Management — hemorrhage, urinary complications, wound infection, DVT, cuff dehiscence, ileus
- Post-op Nursing Care — immediate recovery room care + ward management
- Discharge Patient Education — activity restrictions, warning signs, follow-up
- Quality of Life Outcomes — evidence-based patient outcomes
- Summary Table
Scroll up to read the full detailed assignment. If you need me to:
- Format it as a Word document (.docx) for submission
- Add nursing diagnoses (NANDA) and care plans
- Add more on a specific section (e.g., radical hysterectomy for cervical cancer, robotic technique, or hormonal effects of oophorectomy)
Just let me know!
Assignment hysterectomy included definition, indication,types ,causes, surgical steps, complications,pre operative and post operative management, care given within 48 hours, patient education, summary
Reading File
Reading File
Reading File
Reading File
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.