Venous blood gases topic in detail
"venous blood gas" AND arterial correlation
"venous blood gas" AND "arterial blood gas" clinical utility
Venous Blood Gases (VBG): A Detailed Overview
1. What Is a Venous Blood Gas?
- Tintinalli's Emergency Medicine, p. 304
- Murray & Nadel's Textbook of Respiratory Medicine, p. 2280
2. Sampling Sites
| Site | Source | Clinical Use |
|---|---|---|
| Peripheral vein | Arm/hand vein | Most common; easy access; widely used in ED |
| Central vein (SVC/right atrium) | Central venous catheter | Better for systemic assessment; ScvO2 monitoring |
| Pulmonary artery (mixed venous) | Pulmonary artery catheter (PAC) | Gold standard for true mixed venous; reflects global O2 balance |
- The pulmonary artery is the ideal sampling site because blood from all body sites is equally represented, but it is rarely practical.
- Blood from the superior vena cava (SVC) disproportionately represents cerebral and upper body blood flow.
- Peripheral venous samples are widely used in emergency medicine and correlate closely enough to be clinically useful.
3. Normal VBG Values vs. ABG Values
| Parameter | Arterial (ABG) | Venous (VBG) | Difference |
|---|---|---|---|
| pH | 7.35 - 7.45 | ~7.32 - 7.42 | ~0.03-0.05 lower |
| PCO2 | 35 - 45 mmHg | ~40 - 50 mmHg | ~3-8 mmHg higher |
| PO2 | 80 - 100 mmHg | ~35 - 45 mmHg | Much lower (not usable for oxygenation) |
| HCO3- | 22 - 26 mEq/L | ~2-3 mEq/L higher | ~5% higher than arterial |
| O2 saturation (SvO2) | 95-100% | ~60-80% | Reflects tissue O2 extraction |
- Venous pH averages approximately 0.03 lower than arterial pH (central VBG) - Goldman-Cecil quotes this as ~0.03; Tintinalli cites up to ±0.05.
- Venous PCO2 averages 3-8 mmHg higher than arterial PCO2.
- Venous HCO3- runs approximately 2-3 mmol/L higher because it includes CO2 from cellular metabolic activity not yet excreted by the lung, plus carbonic acid, dissolved CO2, carbonate, and carbamates.
4. What VBG Can and Cannot Tell You
Can Use VBG For:
- pH assessment: Venous pH correlates closely with arterial pH (±0.03-0.05 units). In most clinical scenarios, this difference is not clinically significant. Central VBGs are considered more accurate than peripheral VBGs.
- Hypercapnia screening: A normal PvCO2 effectively excludes hypercapnic respiratory failure. If venous PCO2 is normal, arterial PCO2 is almost certainly normal.
- Acid-base disorders: VBG has excellent agreement with ABG for detecting acid-base disorders, including in patients with shock (ICU studies confirm this).
- Serum lactate: Normal and markedly elevated venous lactate values correlate with arterial lactate. (Caution: mildly elevated venous lactate may not reliably correlate - confirm with arterial if clinically important.)
- Bicarbonate estimation: Venous total CO2/HCO3- provides a useful surrogate for arterial HCO3-.
Cannot Use VBG For:
- Oxygenation assessment: Venous PO2 values do NOT correlate with arterial oxygen content and cannot be used to assess hypoxemia. An ABG (or SpO2) is required.
- Reliable hypercarbia quantification when severe: In states of low cardiac output, high CO2 production, or inhibition of red cell carbonic anhydrase, the arteriovenous PCO2 difference can increase up to 10-fold - making VBG unreliable.
- Hypotensive patients: VBGs are considered unacceptably inaccurate in hypotensive patients with severe hypercapnia.
5. Mixed Venous Oxygen Saturation (SvO2)
- Normal SvO2: ~65-75%
- Low SvO2 (<65%): Suggests global oxygen delivery is deficient relative to consumption - seen in low cardiac output, severe anemia, high metabolic states
- High SvO2 (>75-80%): Seen in septic shock (distributive) with impaired tissue O2 extraction, or in high-flow states
CO = VO2 / (CaO2 - CvO2)
Central Venous O2 Saturation (ScvO2) vs. Mixed Venous (SvO2)
| ScvO2 (SVC/right atrium) | SvO2 (pulmonary artery) | |
|---|---|---|
| Access | Central venous catheter | Pulmonary artery catheter |
| Represents | Upper body + cerebral | Entire body |
| Normal value | ~70-80% | ~65-75% |
| Reliability | Variable; not a reliable surrogate | Gold standard |
6. Arteriovenous Differences - Why They Exist
- pH: ~0.03-0.05 units (vein is more acidic)
- PCO2: ~3-8 mmHg higher venously
- PO2: ~50-60 mmHg lower venously
- HCO3-: ~2-3 mEq/L higher venously
7. Pre-Analytical Errors Affecting VBG Accuracy
- Air exposure: Decreases PCO2, raises pH, and gradually decreases CO2 content
- Saline/fluid dilution (e.g., sampling from a flush line): Causes both PCO2 and HCO3- to fall equally
- Temperature not corrected: Hypothermia causes spuriously higher PCO2, lower pH, and higher PO2; the opposite occurs with hyperthermia
- Delayed analysis: Continued cellular metabolism in the sample affects values
8. Clinical Applications
Emergency Medicine
- Respiratory failure screening: A normal venous PCO2 excludes hypercapnic failure. If hypercapnia or hypoxia is severe, confirm with ABG.
- DKA monitoring: VBG correlates well with ABG for pH and HCO3- monitoring in diabetic ketoacidosis - avoiding repeated arterial punctures.
- Toxicology: VBG used alongside electrolytes in phenol exposure, symptomatic toxic ingestions.
- Pediatric assessment: VBG commonly used alongside glucose, ammonia, and metabolic panel in metabolic emergencies.
Critical Care / ICU
- Acid-base monitoring: Central VBGs have excellent agreement with ABGs for acid-base assessment, including in patients in shock.
- Sepsis: ScvO2 monitoring (though no longer a guideline recommendation as of 2016).
- Hemorrhagic shock: VBG alongside TEG and type-and-screen is prioritized in severe hemorrhagic shock.
- COPD exacerbation: VBG is recommended as initial blood gas; if severe hypercapnia or hypoxia present, follow with ABG.
Surgery / Anesthesia
- Continuous SvO2 monitoring via PAC in high-risk surgical patients; provides real-time assessment of global perfusion adequacy.
9. VBG vs. ABG - When to Choose Which
| Clinical Question | Use |
|---|---|
| Is oxygenation adequate? | ABG (or SpO2) - VBG cannot assess this |
| Is the patient hypercapnic? | VBG first; normal excludes hypercapnia. Confirm ABG if elevated or severe |
| What is the acid-base status? | VBG is acceptable (pH ±0.03-0.05) |
| Is bicarbonate normal? | VBG (HCO3- runs ~2-3 mEq/L higher than arterial) |
| Is lactate elevated? | VBG acceptable for screening; mildly elevated should be confirmed |
| Is global O2 delivery adequate? | Mixed SvO2 from PAC (or ScvO2 as trend) |
| Hypotensive / severely hypercapnic patient | ABG preferred; VBG unreliable |
10. Key Formulas Relevant to VBG Interpretation
PaCO2 = (1.5 × [HCO3-] + 8) ± 2
CO = VO2 / (CaO2 - CvO2)
VD/VT = (PaCO2 - PeCO2) / PaCO2
Summary Table
| Feature | VBG | ABG |
|---|---|---|
| Invasiveness | Low (venipuncture) | Higher (arterial puncture) |
| Pain | Minimal | Moderate |
| pH accuracy | Good (±0.03-0.05) | Reference standard |
| PCO2 | Elevated ~3-8 mmHg vs. arterial | Reference |
| PO2 / Oxygenation | Not useful | Required |
| HCO3- | ~2-3 mEq/L higher | Reference |
| Lactate | Acceptable (screen); confirm if mildly elevated | More accurate |
| Use in shock/hypotension | Unreliable | Preferred |
| SvO2 (mixed venous) | Via PAC only | N/A |
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, pp. 304-310
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 2270-2282
- Goldman-Cecil Medicine International Edition, p. 754
- Fishman's Pulmonary Diseases and Disorders, p. 2060
- Miller's Anesthesia 10e, pp. 833-835
- Rosen's Emergency Medicine: Concepts and Clinical Practice, pp. 2550-2551
Can you make this into a pdf
ls -la /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace
mkdir -p /home/daytona/workspace/vbg-pdf && python3 -c "from reportlab.lib.pagesizes import A4; print('reportlab ok')" && python3 -c "from weasyprint import HTML; print('weasyprint ok')" 2>&1 || true
~/vbg-pdf/generate_vbg_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import cm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak
)
from reportlab.platypus.flowables import KeepTogether
OUTPUT = "/home/daytona/workspace/vbg-pdf/Venous_Blood_Gases.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=2*cm, rightMargin=2*cm,
topMargin=2.2*cm, bottomMargin=2.2*cm,
title="Venous Blood Gases",
author="Orris Medical Reference"
)
W = A4[0] - 4*cm # usable width
# ── Colour palette ──────────────────────────────────────────────────────────
NAVY = colors.HexColor("#1a3a5c")
TEAL = colors.HexColor("#0d6e8a")
LIGHT = colors.HexColor("#e8f4f8")
ACCENT = colors.HexColor("#f0a500")
WHITE = colors.white
LGREY = colors.HexColor("#f5f5f5")
DGREY = colors.HexColor("#333333")
MGREY = colors.HexColor("#666666")
RED = colors.HexColor("#c0392b")
GREEN = colors.HexColor("#1a7a4a")
# ── Styles ───────────────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
title_style = ParagraphStyle("Title", fontName="Helvetica-Bold",
fontSize=22, textColor=WHITE, alignment=TA_CENTER, leading=28)
subtitle_style = ParagraphStyle("Subtitle", fontName="Helvetica",
fontSize=11, textColor=colors.HexColor("#cce8f0"),
alignment=TA_CENTER, leading=16)
h1 = ParagraphStyle("H1", fontName="Helvetica-Bold",
fontSize=14, textColor=WHITE, leading=18,
backColor=NAVY, leftPadding=8, rightPadding=8,
spaceBefore=14, spaceAfter=4)
h2 = ParagraphStyle("H2", fontName="Helvetica-Bold",
fontSize=12, textColor=TEAL, leading=16,
spaceBefore=10, spaceAfter=3)
body = ParagraphStyle("Body", fontName="Helvetica",
fontSize=9.5, textColor=DGREY, leading=14,
spaceBefore=2, spaceAfter=2, alignment=TA_JUSTIFY)
bullet = ParagraphStyle("Bullet", fontName="Helvetica",
fontSize=9.5, textColor=DGREY, leading=14,
leftIndent=14, bulletIndent=4, spaceBefore=1, spaceAfter=1)
small_italic = ParagraphStyle("SmallItalic", fontName="Helvetica-Oblique",
fontSize=8.5, textColor=MGREY, leading=12,
spaceBefore=2, spaceAfter=4)
note_style = ParagraphStyle("Note", fontName="Helvetica",
fontSize=8.8, textColor=DGREY, leading=13,
backColor=LIGHT, leftPadding=8, rightPadding=8, borderPadding=6,
spaceBefore=4, spaceAfter=4)
warn_style = ParagraphStyle("Warn", fontName="Helvetica-Bold",
fontSize=9, textColor=RED, leading=13,
leftIndent=10, spaceBefore=2, spaceAfter=2)
source_style = ParagraphStyle("Source", fontName="Helvetica-Oblique",
fontSize=8, textColor=MGREY, leading=11,
spaceBefore=0, spaceAfter=0)
def h1_para(text):
return Paragraph(f" {text}", h1)
def h2_para(text):
return Paragraph(text, h2)
def para(text):
return Paragraph(text, body)
def bul(text):
return Paragraph(f"\u2022 {text}", bullet)
def src(text):
return Paragraph(f"<i>- {text}</i>", source_style)
# ── Helper: coloured table ───────────────────────────────────────────────────
def make_table(headers, rows, col_widths=None, header_bg=NAVY, alt=True):
data = [[Paragraph(f"<b>{h}</b>", ParagraphStyle("TH",
fontName="Helvetica-Bold", fontSize=9, textColor=WHITE,
leading=12, alignment=TA_CENTER))
for h in headers]]
for i, row in enumerate(rows):
data.append([Paragraph(str(cell), ParagraphStyle("TD",
fontName="Helvetica", fontSize=8.8,
textColor=DGREY, leading=12, alignment=TA_CENTER))
for cell in row])
style = [
("BACKGROUND", (0,0), (-1,0), header_bg),
("ROWBACKGROUNDS", (0,1), (-1,-1),
[LGREY, WHITE] if alt else [WHITE]),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#cccccc")),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
("LINEBELOW", (0,0), (-1,0), 1, ACCENT),
]
t = Table(data, colWidths=col_widths, repeatRows=1)
t.setStyle(TableStyle(style))
return t
# ── Build story ──────────────────────────────────────────────────────────────
story = []
# ── Cover banner ─────────────────────────────────────────────────────────────
banner_data = [[
Paragraph("Venous Blood Gases", title_style),
""
],[
Paragraph("A Comprehensive Clinical Reference", subtitle_style),
""
],[
Paragraph("Based on: Tintinalli's EM · Murray & Nadel's · Goldman-Cecil · Fishman's · Miller's Anesthesia · Rosen's EM", subtitle_style),
""
]]
banner = Table(banner_data, colWidths=[W, 0])
banner.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("TOPPADDING", (0,0), (-1,-1), 10),
("BOTTOMPADDING", (0,0), (-1,-1), 10),
("LEFTPADDING", (0,0), (-1,-1), 12),
("RIGHTPADDING", (0,0), (-1,-1), 12),
]))
story.append(banner)
story.append(Spacer(1, 0.5*cm))
# ── 1. Definition ─────────────────────────────────────────────────────────────
story.append(h1_para("1. What Is a Venous Blood Gas (VBG)?"))
story.append(Spacer(1, 0.15*cm))
story.append(para(
"A <b>venous blood gas (VBG)</b> is an analysis of blood taken from a venous source "
"to measure pH, PCO\u2082, PO\u2082, bicarbonate (HCO\u2083\u207b), and oxygen saturation. "
"It is less invasive and less painful than an arterial blood gas (ABG), making it widely "
"used in emergency medicine and critical care. Partially or centrally obtained venous "
"samples are both in routine clinical use."
))
story.append(src("Tintinalli's Emergency Medicine, p. 304 | Murray & Nadel's Textbook of Respiratory Medicine, p. 2280"))
story.append(Spacer(1, 0.2*cm))
# ── 2. Sampling Sites ────────────────────────────────────────────────────────
story.append(h1_para("2. Sampling Sites"))
story.append(Spacer(1, 0.15*cm))
story.append(make_table(
["Site", "Source", "Clinical Use"],
[
["Peripheral vein", "Arm / hand vein", "Most common; easy access; widely used in ED"],
["Central vein (SVC / right atrium)", "Central venous catheter",
"Better systemic assessment; ScvO\u2082 monitoring"],
["Pulmonary artery (mixed venous)", "Pulmonary artery catheter (PAC)",
"Gold standard for true mixed venous; reflects global O\u2082 balance"],
],
col_widths=[W*0.28, W*0.28, W*0.44]
))
story.append(Spacer(1, 0.2*cm))
story.append(bul(
"The <b>pulmonary artery</b> is the ideal site because blood from all body sites is equally "
"represented, but placement is rarely practical."
))
story.append(bul(
"Blood from the <b>SVC</b> disproportionately represents cerebral and upper body flow."
))
story.append(bul(
"<b>Peripheral venous</b> samples are widely used and correlate closely enough to be "
"clinically useful; significantly abnormal values should be confirmed with an ABG."
))
story.append(src("Tintinalli's Emergency Medicine, p. 304"))
story.append(Spacer(1, 0.2*cm))
# ── 3. Normal Values ─────────────────────────────────────────────────────────
story.append(h1_para("3. Normal VBG Values vs. ABG Values"))
story.append(Spacer(1, 0.15*cm))
story.append(make_table(
["Parameter", "Arterial (ABG)", "Venous (VBG)", "Typical Difference"],
[
["pH", "7.35 - 7.45", "~7.32 - 7.42", "~0.03 - 0.05 lower"],
["PCO\u2082 (mmHg)", "35 - 45", "~40 - 50", "~3 - 8 mmHg higher"],
["PO\u2082 (mmHg)", "80 - 100", "~35 - 45", "Much lower (not for oxygenation)"],
["HCO\u2083\u207b (mEq/L)", "22 - 26", "~24 - 29", "~2 - 3 mEq/L higher"],
["O\u2082 Saturation", "95 - 100%", "~60 - 80% (SvO\u2082)", "Reflects tissue O\u2082 extraction"],
],
col_widths=[W*0.22, W*0.22, W*0.22, W*0.34]
))
story.append(Spacer(1, 0.2*cm))
story.append(bul(
"Venous <b>HCO\u2083\u207b</b> runs ~2-3 mmol/L higher because venous blood includes CO\u2082 "
"from cellular metabolism not yet excreted by the lungs, plus carbonic acid, dissolved CO\u2082, "
"carbonate, and carbamates."
))
story.append(src("Murray & Nadel's, p. 2280-2282 | Goldman-Cecil Medicine, p. 754"))
story.append(Spacer(1, 0.2*cm))
# ── 4. What VBG Can and Cannot Tell You ──────────────────────────────────────
story.append(h1_para("4. What VBG Can and Cannot Tell You"))
story.append(Spacer(1, 0.15*cm))
story.append(h2_para("CAN Use VBG For:"))
story.append(bul(
"<b>pH assessment:</b> Correlates closely with arterial pH (±0.03-0.05 units). In most "
"clinical scenarios this difference is not clinically significant. Central VBGs are more "
"accurate than peripheral."
))
story.append(bul(
"<b>Hypercapnia screening:</b> A <b>normal PvCO\u2082 effectively excludes hypercapnic "
"respiratory failure.</b> If venous PCO\u2082 is normal, arterial PCO\u2082 is almost "
"certainly normal."
))
story.append(bul(
"<b>Acid-base disorders:</b> Excellent agreement with ABG for detecting acid-base disorders, "
"including in ICU patients in shock."
))
story.append(bul(
"<b>Bicarbonate estimation:</b> Venous total CO\u2082/HCO\u2083\u207b is a useful surrogate "
"for arterial HCO\u2083\u207b."
))
story.append(bul(
"<b>Lactate (screening):</b> Normal and markedly abnormal venous lactate correlates with "
"arterial lactate. Mildly elevated venous lactate may not reliably correlate - confirm with "
"arterial if clinically important."
))
story.append(bul(
"<b>DKA monitoring:</b> VBG correlates well with ABG for pH and HCO\u2083\u207b, avoiding "
"repeated arterial punctures."
))
story.append(Spacer(1, 0.15*cm))
story.append(h2_para("CANNOT Use VBG For:"))
story.append(Paragraph(
"\u26a0\ufe0f <b>Oxygenation assessment:</b> Venous PO\u2082 does NOT correlate with arterial "
"oxygen content and <b>cannot</b> be used to assess hypoxemia. ABG or SpO\u2082 is required.",
ParagraphStyle("WarnBox", fontName="Helvetica-Bold", fontSize=9.5,
textColor=RED, leading=14, leftIndent=14, spaceBefore=3, spaceAfter=3)
))
story.append(Paragraph(
"\u26a0\ufe0f <b>Reliable hypercarbia quantification when severe:</b> In low cardiac output, "
"high CO\u2082 production, or inhibition of red cell carbonic anhydrase, the arteriovenous "
"PCO\u2082 difference can increase up to <b>10-fold</b>, rendering VBG unreliable.",
ParagraphStyle("WarnBox2", fontName="Helvetica-Bold", fontSize=9.5,
textColor=RED, leading=14, leftIndent=14, spaceBefore=3, spaceAfter=3)
))
story.append(Paragraph(
"\u26a0\ufe0f <b>Hypotensive patients with severe hypercapnia:</b> VBGs are considered "
"unacceptably inaccurate. ABG is preferred.",
ParagraphStyle("WarnBox3", fontName="Helvetica-Bold", fontSize=9.5,
textColor=RED, leading=14, leftIndent=14, spaceBefore=3, spaceAfter=3)
))
story.append(src("Goldman-Cecil, p. 754 | Tintinalli's, p. 306 | Murray & Nadel's, p. 2280"))
story.append(Spacer(1, 0.2*cm))
# ── 5. Mixed Venous O2 Saturation ────────────────────────────────────────────
story.append(h1_para("5. Mixed Venous Oxygen Saturation (SvO\u2082)"))
story.append(Spacer(1, 0.15*cm))
story.append(para(
"The <b>mixed venous oxygen saturation (SvO\u2082)</b>, measured from the pulmonary artery "
"via a PAC, is a global indicator of the balance between oxygen delivery (DO\u2082) and "
"oxygen consumption (VO\u2082)."
))
story.append(Spacer(1, 0.1*cm))
story.append(make_table(
["SvO\u2082 Value", "Interpretation"],
[
["Normal: 65 - 75%", "Adequate global O\u2082 delivery/consumption balance"],
["Low: < 65%", "Global O\u2082 delivery deficient - low CO, severe anaemia, high metabolic state"],
["High: > 75 - 80%", "Distributive shock (e.g. sepsis), impaired tissue O\u2082 extraction, or high-flow state"],
],
col_widths=[W*0.30, W*0.70]
))
story.append(Spacer(1, 0.15*cm))
story.append(para(
"<b>Fick's principle</b> allows cardiac output estimation using SvO\u2082:"
))
# Formula box
formula_table = Table(
[[Paragraph("CO = VO\u2082 / (CaO\u2082 \u2212 CvO\u2082)",
ParagraphStyle("Formula", fontName="Helvetica-Bold", fontSize=11,
textColor=NAVY, leading=16, alignment=TA_CENTER))]],
colWidths=[W]
)
formula_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LIGHT),
("BOX", (0,0), (-1,-1), 1, TEAL),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
]))
story.append(formula_table)
story.append(Spacer(1, 0.1*cm))
story.append(bul(
"<b>Important limitation:</b> SvO\u2082 is a <i>global</i> measure. Organ-specific ischemia "
"may be present even with a normal or elevated mixed venous saturation."
))
story.append(src("Miller's Anesthesia 10e, p. 833-835"))
story.append(Spacer(1, 0.2*cm))
# ScvO2 vs SvO2
story.append(h2_para("Central Venous O\u2082 Saturation (ScvO\u2082) vs. Mixed Venous (SvO\u2082)"))
story.append(make_table(
["", "ScvO\u2082 (SVC / right atrium)", "SvO\u2082 (pulmonary artery)"],
[
["Access", "Central venous catheter", "Pulmonary artery catheter (PAC)"],
["Represents", "Upper body + cerebral flow", "Entire body"],
["Normal value", "~70 - 80%", "~65 - 75%"],
["Reliability", "Variable; NOT a reliable SvO\u2082 surrogate", "Gold standard"],
],
col_widths=[W*0.22, W*0.39, W*0.39]
))
story.append(Spacer(1, 0.1*cm))
story.append(bul(
"Monitoring of ScvO\u2082 was previously part of the <b>Surviving Sepsis Campaign</b>, but "
"failure to demonstrate clinical benefit led to its <b>removal from the 2016 guidelines</b>."
))
story.append(src("Tintinalli's, p. 308 | Miller's Anesthesia, p. 835"))
story.append(Spacer(1, 0.2*cm))
# ── 6. A-V Differences ───────────────────────────────────────────────────────
story.append(h1_para("6. Arteriovenous Differences - Why They Exist"))
story.append(Spacer(1, 0.15*cm))
story.append(para(
"Venous blood is lower in O\u2082 and higher in CO\u2082 because tissues extract oxygen and "
"produce CO\u2082. Normal arteriovenous differences:"
))
story.append(Spacer(1, 0.1*cm))
story.append(make_table(
["Parameter", "Arterial", "Venous", "Normal A-V Difference"],
[
["pH", "7.35 - 7.45", "~0.03 - 0.05 lower", "Vein is more acidic"],
["PCO\u2082 (mmHg)", "35 - 45", "~40 - 50", "3 - 8 mmHg higher venously"],
["PO\u2082 (mmHg)", "80 - 100", "~35 - 45", "~50 - 60 mmHg lower venously"],
["HCO\u2083\u207b (mEq/L)", "22 - 26", "~24 - 29", "~2 - 3 mEq/L higher venously"],
],
col_widths=[W*0.22, W*0.22, W*0.22, W*0.34]
))
story.append(Spacer(1, 0.1*cm))
story.append(bul(
"These differences <b>widen significantly in low-flow states</b> (shock, heart failure) "
"because tissues extract proportionally more O\u2082 and dump more CO\u2082."
))
story.append(Spacer(1, 0.2*cm))
# ── 7. Pre-Analytical Errors ─────────────────────────────────────────────────
story.append(h1_para("7. Pre-Analytical Errors Affecting VBG Accuracy"))
story.append(Spacer(1, 0.15*cm))
story.append(make_table(
["Error", "Effect on Values"],
[
["Air exposure", "Decreases PCO\u2082, raises pH, gradually decreases CO\u2082 content"],
["Saline / fluid dilution (from flush line)", "PCO\u2082 and HCO\u2083\u207b both fall equally"],
["Hypothermia (no temperature correction)", "Spuriously higher PCO\u2082, lower pH, higher PO\u2082"],
["Hyperthermia (no temperature correction)", "Opposite of hypothermia effects"],
["Delayed analysis (prolonged sample time)", "Continued cellular metabolism alters values"],
],
col_widths=[W*0.45, W*0.55]
))
story.append(src("Murray & Nadel's, p. 2274-2278"))
story.append(Spacer(1, 0.2*cm))
# ── 8. Clinical Applications ─────────────────────────────────────────────────
story.append(h1_para("8. Clinical Applications"))
story.append(Spacer(1, 0.15*cm))
story.append(h2_para("Emergency Medicine"))
for pt in [
"<b>Respiratory failure screening:</b> A normal venous PCO\u2082 excludes hypercapnic failure. Severe hypercapnia or hypoxia - confirm with ABG.",
"<b>DKA monitoring:</b> VBG correlates well with ABG for pH/HCO\u2083\u207b, avoiding repeated arterial punctures.",
"<b>Toxicology:</b> VBG used alongside electrolytes in phenol exposure, toxic ingestions.",
"<b>Paediatric assessment:</b> VBG used with glucose, ammonia, and metabolic panel in metabolic emergencies.",
]:
story.append(bul(pt))
story.append(Spacer(1, 0.1*cm))
story.append(h2_para("Critical Care / ICU"))
for pt in [
"<b>Acid-base monitoring:</b> Central VBGs have excellent agreement with ABGs for acid-base assessment, including in patients in shock.",
"<b>Sepsis:</b> ScvO\u2082 monitoring (no longer a Surviving Sepsis Campaign recommendation as of 2016).",
"<b>Haemorrhagic shock:</b> VBG alongside TEG and type-and-screen is prioritised in severe haemorrhagic shock.",
"<b>COPD exacerbation:</b> VBG recommended as initial blood gas; follow with ABG if severe hypercapnia or hypoxia.",
]:
story.append(bul(pt))
story.append(Spacer(1, 0.1*cm))
story.append(h2_para("Surgery / Anaesthesia"))
story.append(bul(
"Continuous SvO\u2082 monitoring via PAC in high-risk surgical patients provides real-time "
"assessment of global perfusion adequacy."
))
story.append(src("Tintinalli's, p. 304-310 | Rosen's EM, p. 2550 | Fishman's Pulmonary Diseases, p. 2060-2061"))
story.append(Spacer(1, 0.2*cm))
# ── 9. VBG vs ABG Decision Table ─────────────────────────────────────────────
story.append(h1_para("9. VBG vs. ABG - When to Choose Which"))
story.append(Spacer(1, 0.15*cm))
story.append(make_table(
["Clinical Question", "Recommended Test"],
[
["Is oxygenation adequate?", "ABG or SpO\u2082 - VBG cannot assess this"],
["Is the patient hypercapnic?", "VBG first; normal excludes hypercapnia. Confirm ABG if elevated"],
["What is the acid-base status?", "VBG is acceptable (pH \u00b10.03-0.05)"],
["Is bicarbonate normal?", "VBG (HCO\u2083\u207b ~2-3 mEq/L higher than arterial)"],
["Is lactate elevated?", "VBG for screening; mildly elevated should be confirmed with ABG"],
["Is global O\u2082 delivery adequate?", "Mixed SvO\u2082 from PAC (or ScvO\u2082 as a trend)"],
["Hypotensive / severely hypercapnic patient", "ABG preferred; VBG unreliable in this setting"],
],
col_widths=[W*0.50, W*0.50]
))
story.append(Spacer(1, 0.2*cm))
# ── 10. Key Formulas ─────────────────────────────────────────────────────────
story.append(h1_para("10. Key Formulas"))
story.append(Spacer(1, 0.15*cm))
formulas = [
("Winter's Equation", "Expected PaCO\u2082 in metabolic acidosis",
"PaCO\u2082 = (1.5 \u00d7 [HCO\u2083\u207b] + 8) \u00b1 2",
"PaCO\u2082 above expected = inadequate ventilatory response"),
("Fick Equation", "Cardiac output from mixed venous saturation",
"CO = VO\u2082 / (CaO\u2082 \u2212 CvO\u2082)",
"Requires SvO\u2082 from pulmonary artery"),
("Dead Space Fraction", "Requires ABG; gauges severity of lung disease",
"V\u1d05/V\u1d1b = (PaCO\u2082 \u2212 PeCO\u2082) / PaCO\u2082",
"PeCO\u2082 measured by metabolic monitor or capnography"),
]
for name, desc, formula, note in formulas:
row_data = [[
Paragraph(f"<b>{name}</b>",
ParagraphStyle("FN", fontName="Helvetica-Bold", fontSize=9.5,
textColor=NAVY, leading=13)),
Paragraph(desc,
ParagraphStyle("FD", fontName="Helvetica", fontSize=9,
textColor=MGREY, leading=13)),
Paragraph(formula,
ParagraphStyle("FF", fontName="Helvetica-Bold", fontSize=10,
textColor=TEAL, leading=14, alignment=TA_CENTER)),
Paragraph(f"<i>{note}</i>",
ParagraphStyle("FNote", fontName="Helvetica-Oblique", fontSize=8.5,
textColor=MGREY, leading=12)),
]]
t = Table(row_data, colWidths=[W*0.22, W*0.26, W*0.28, W*0.24])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LGREY),
("BOX", (0,0), (-1,-1), 0.5, colors.HexColor("#cccccc")),
("LINEAFTER", (0,0), (2,0), 0.5, colors.HexColor("#cccccc")),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
]))
story.append(t)
story.append(Spacer(1, 0.1*cm))
story.append(Spacer(1, 0.2*cm))
# ── 11. Summary Table ────────────────────────────────────────────────────────
story.append(h1_para("11. Summary Comparison Table"))
story.append(Spacer(1, 0.15*cm))
story.append(make_table(
["Feature", "VBG", "ABG"],
[
["Invasiveness", "Low (venipuncture)", "Higher (arterial puncture)"],
["Pain", "Minimal", "Moderate"],
["pH accuracy", "Good (\u00b10.03-0.05)", "Reference standard"],
["PCO\u2082", "~3-8 mmHg higher than arterial", "Reference"],
["PO\u2082 / Oxygenation", "\u274c Not useful", "\u2705 Required for O\u2082 assessment"],
["HCO\u2083\u207b", "~2-3 mEq/L higher", "Reference"],
["Lactate", "Acceptable (screen); confirm if mildly elevated", "More accurate"],
["Use in shock / hypotension", "\u26a0 Unreliable", "\u2705 Preferred"],
["Mixed venous O\u2082 (SvO\u2082)", "Via PAC only", "N/A"],
],
col_widths=[W*0.32, W*0.35, W*0.33]
))
story.append(Spacer(1, 0.3*cm))
# ── References ────────────────────────────────────────────────────────────────
story.append(HRFlowable(width=W, thickness=1, color=TEAL))
story.append(Spacer(1, 0.1*cm))
story.append(Paragraph("<b>References</b>", ParagraphStyle("RefHead",
fontName="Helvetica-Bold", fontSize=10, textColor=NAVY, leading=14)))
story.append(Spacer(1, 0.05*cm))
refs = [
"Tintinalli's Emergency Medicine: A Comprehensive Study Guide, pp. 304-310",
"Murray & Nadel's Textbook of Respiratory Medicine, pp. 2270-2282",
"Goldman-Cecil Medicine International Edition, p. 754",
"Fishman's Pulmonary Diseases and Disorders, p. 2060",
"Miller's Anesthesia 10th Edition, pp. 833-835",
"Rosen's Emergency Medicine: Concepts and Clinical Practice, pp. 2550-2551",
"Harrison's Principles of Internal Medicine 22E (2025)",
]
for r in refs:
story.append(Paragraph(f"\u2022 {r}", ParagraphStyle("Ref",
fontName="Helvetica", fontSize=8.5, textColor=MGREY,
leading=12, leftIndent=12, spaceBefore=1)))
# ── Page numbers via canvas ──────────────────────────────────────────────────
def add_page_number(canvas, doc):
canvas.saveState()
canvas.setFont("Helvetica", 8)
canvas.setFillColor(MGREY)
canvas.drawRightString(A4[0] - 2*cm, 1.2*cm, f"Page {doc.page}")
canvas.drawString(2*cm, 1.2*cm, "Venous Blood Gases - Orris Medical Reference")
canvas.restoreState()
doc.build(story, onFirstPage=add_page_number, onLaterPages=add_page_number)
print(f"PDF created: {OUTPUT}")
cd /home/daytona/workspace/vbg-pdf && python3 generate_vbg_pdf.py 2>&1
ls -lh /home/daytona/workspace/vbg-pdf/Venous_Blood_Gases.pdf
Venous Blood Gases
PDF Document · PDF
- Definition - What a VBG is
- Sampling Sites - Peripheral, central, and pulmonary artery with a comparison table
- Normal Values - VBG vs. ABG reference table
- What VBG Can/Cannot Tell You - With red-highlighted warnings for oxygenation, severe hypercapnia, and hypotension
- Mixed Venous O2 Saturation - SvO2 interpretation table + Fick equation in a highlighted formula box
- Arteriovenous Differences - Why they exist and when they widen
- Pre-Analytical Errors - Common sampling pitfalls
- Clinical Applications - Emergency medicine, ICU, and anaesthesia
- VBG vs. ABG Decision Table - Quick clinical guide
- Key Formulas - Winter's, Fick, and Dead Space equations
- Summary Comparison Table + full references
The pdf does not work
pandoc --version 2>&1 | head -3; wkhtmltopdf --version 2>&1 | head -3; which libreoffice 2>&1
~/vbg-pdf/vbg.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<title>Venous Blood Gases – Clinical Reference</title>
<style>
@page { size: A4; margin: 2cm 2.2cm 2cm 2.2cm; }
* { box-sizing: border-box; margin: 0; padding: 0; }
body { font-family: Arial, Helvetica, sans-serif; font-size: 10pt; color: #222; line-height: 1.5; }
/* HEADER BANNER */
.banner { background: #1a3a5c; color: white; padding: 18px 22px 14px; margin-bottom: 18px; }
.banner h1 { font-size: 22pt; font-weight: bold; margin-bottom: 4px; }
.banner .sub { font-size: 10pt; color: #cce8f0; }
/* SECTION HEADINGS */
h2 { background: #1a3a5c; color: white; font-size: 12pt; padding: 5px 10px;
margin: 18px 0 6px; }
h3 { color: #0d6e8a; font-size: 11pt; margin: 10px 0 4px; border-bottom: 1px solid #c0dde8; padding-bottom: 2px; }
p { margin-bottom: 6px; text-align: justify; }
ul { margin: 4px 0 6px 20px; }
ul li { margin-bottom: 3px; }
/* TABLES */
table { border-collapse: collapse; width: 100%; margin: 8px 0 10px; font-size: 9pt; }
thead tr { background: #1a3a5c; color: white; }
thead th { padding: 6px 8px; text-align: center; border-bottom: 2px solid #f0a500; }
tbody tr:nth-child(even) { background: #f5f5f5; }
tbody tr:nth-child(odd) { background: #ffffff; }
tbody td { padding: 5px 8px; border: 1px solid #ddd; vertical-align: top; }
/* FORMULA BOX */
.formula { background: #e8f4f8; border: 1.5px solid #0d6e8a; border-radius: 4px;
text-align: center; padding: 10px; margin: 8px 0; font-size: 12pt;
font-weight: bold; color: #1a3a5c; }
/* WARNING BOXES */
.warn { color: #c0392b; font-weight: bold; padding: 2px 0 2px 12px;
border-left: 3px solid #c0392b; margin: 4px 0; }
/* NOTE BOX */
.note { background: #e8f4f8; padding: 8px 12px; margin: 6px 0; font-size: 9pt; }
/* SOURCE CITATIONS */
.src { font-style: italic; color: #777; font-size: 8pt; margin-top: 2px; margin-bottom: 6px; }
/* REFERENCES */
.refs { border-top: 1px solid #0d6e8a; margin-top: 16px; padding-top: 8px; }
.refs h3 { color: #1a3a5c; border-bottom: none; }
.refs li { font-size: 8.5pt; color: #555; }
/* FOOTER NOTE */
.footer { font-size: 8pt; color: #aaa; text-align: center; margin-top: 20px; border-top: 1px solid #eee; padding-top: 6px; }
</style>
</head>
<body>
<!-- BANNER -->
<div class="banner">
<h1>Venous Blood Gases (VBG)</h1>
<div class="sub">A Comprehensive Clinical Reference</div>
<div class="sub" style="margin-top:4px; font-size:9pt;">
Based on: Tintinalli's EM · Murray & Nadel's · Goldman-Cecil · Fishman's · Miller's Anesthesia · Rosen's EM
</div>
</div>
<!-- 1. DEFINITION -->
<h2>1. What Is a Venous Blood Gas (VBG)?</h2>
<p>
A <strong>venous blood gas (VBG)</strong> is an analysis of blood taken from a venous source to measure
pH, PCO<sub>2</sub>, PO<sub>2</sub>, bicarbonate (HCO<sub>3</sub><sup>−</sup>), and oxygen saturation.
It is less invasive and less painful than an arterial blood gas (ABG), making it widely used in
emergency medicine and critical care. Both peripherally and centrally obtained venous samples are in
routine clinical use.
</p>
<p class="src">— Tintinalli's Emergency Medicine, p. 304 | Murray & Nadel's Textbook of Respiratory Medicine, p. 2280</p>
<!-- 2. SAMPLING SITES -->
<h2>2. Sampling Sites</h2>
<table>
<thead><tr><th>Site</th><th>Source</th><th>Clinical Use</th></tr></thead>
<tbody>
<tr>
<td><strong>Peripheral vein</strong></td>
<td>Arm / hand vein</td>
<td>Most common; easy access; widely used in ED</td>
</tr>
<tr>
<td><strong>Central vein (SVC / right atrium)</strong></td>
<td>Central venous catheter</td>
<td>Better systemic assessment; ScvO<sub>2</sub> monitoring</td>
</tr>
<tr>
<td><strong>Pulmonary artery (mixed venous)</strong></td>
<td>Pulmonary artery catheter (PAC)</td>
<td>Gold standard for true mixed venous; reflects global O<sub>2</sub> balance</td>
</tr>
</tbody>
</table>
<ul>
<li>The <strong>pulmonary artery</strong> is the ideal site because blood from all body sites is equally represented, but it is rarely practical to obtain.</li>
<li>Blood from the <strong>SVC</strong> disproportionately represents cerebral and upper body blood flow.</li>
<li><strong>Peripheral venous</strong> samples correlate closely enough to be clinically useful; significantly abnormal values should be confirmed with an ABG.</li>
</ul>
<p class="src">— Tintinalli's Emergency Medicine, p. 304</p>
<!-- 3. NORMAL VALUES -->
<h2>3. Normal VBG Values vs. ABG Values</h2>
<table>
<thead><tr><th>Parameter</th><th>Arterial (ABG)</th><th>Venous (VBG)</th><th>Typical Difference</th></tr></thead>
<tbody>
<tr><td><strong>pH</strong></td><td>7.35 – 7.45</td><td>~7.32 – 7.42</td><td>~0.03 – 0.05 lower</td></tr>
<tr><td><strong>PCO<sub>2</sub> (mmHg)</strong></td><td>35 – 45</td><td>~40 – 50</td><td>~3 – 8 mmHg higher</td></tr>
<tr><td><strong>PO<sub>2</sub> (mmHg)</strong></td><td>80 – 100</td><td>~35 – 45</td><td>Much lower (not usable for oxygenation)</td></tr>
<tr><td><strong>HCO<sub>3</sub><sup>−</sup> (mEq/L)</strong></td><td>22 – 26</td><td>~24 – 29</td><td>~2 – 3 mEq/L higher</td></tr>
<tr><td><strong>O<sub>2</sub> Saturation</strong></td><td>95 – 100%</td><td>~60 – 80% (SvO<sub>2</sub>)</td><td>Reflects tissue O<sub>2</sub> extraction</td></tr>
</tbody>
</table>
<ul>
<li>Venous <strong>HCO<sub>3</sub><sup>−</sup></strong> runs ~2–3 mmol/L higher because venous blood includes CO<sub>2</sub> from cellular metabolism not yet excreted by the lungs, plus carbonic acid, dissolved CO<sub>2</sub>, carbonate, and carbamates.</li>
<li>Venous pH averages ~0.03 lower than arterial (central VBG); peripheral VBG may differ by up to ±0.05.</li>
</ul>
<p class="src">— Murray & Nadel's, p. 2280–2282 | Goldman-Cecil Medicine, p. 754</p>
<!-- 4. CAN / CANNOT -->
<h2>4. What VBG Can and Cannot Tell You</h2>
<h3>✓ CAN Use VBG For:</h3>
<ul>
<li><strong>pH assessment:</strong> Correlates closely with arterial pH (±0.03–0.05 units). In most clinical scenarios this difference is not clinically significant. Central VBGs are more accurate than peripheral.</li>
<li><strong>Hypercapnia screening:</strong> A <strong>normal PvCO<sub>2</sub> effectively excludes hypercapnic respiratory failure.</strong> If venous PCO<sub>2</sub> is normal, arterial PCO<sub>2</sub> is almost certainly normal.</li>
<li><strong>Acid-base disorders:</strong> Excellent agreement with ABG for detecting acid-base disorders, including in ICU patients in shock.</li>
<li><strong>Bicarbonate estimation:</strong> Venous total CO<sub>2</sub>/HCO<sub>3</sub><sup>−</sup> is a useful surrogate for arterial HCO<sub>3</sub><sup>−</sup>.</li>
<li><strong>Lactate (screening):</strong> Normal and markedly abnormal venous lactate correlates with arterial lactate. Mildly elevated venous lactate may not reliably correlate — confirm with arterial if clinically important.</li>
<li><strong>DKA monitoring:</strong> VBG correlates well with ABG for pH and HCO<sub>3</sub><sup>−</sup>, avoiding repeated arterial punctures.</li>
</ul>
<h3>✗ CANNOT Use VBG For:</h3>
<div class="warn">⚠ Oxygenation assessment: Venous PO<sub>2</sub> does NOT correlate with arterial oxygen content and <u>cannot</u> be used to assess hypoxaemia. ABG or SpO<sub>2</sub> is required.</div>
<div class="warn">⚠ Reliable hypercarbia quantification when severe: In low cardiac output, high CO<sub>2</sub> production, or inhibition of red cell carbonic anhydrase, the arteriovenous PCO<sub>2</sub> difference can increase up to <strong>10-fold</strong>, rendering VBG unreliable.</div>
<div class="warn">⚠ Hypotensive patients with severe hypercapnia: VBGs are considered unacceptably inaccurate. ABG is preferred.</div>
<p class="src">— Goldman-Cecil, p. 754 | Tintinalli's, p. 306 | Murray & Nadel's, p. 2280</p>
<!-- 5. MIXED VENOUS -->
<h2>5. Mixed Venous Oxygen Saturation (SvO<sub>2</sub>)</h2>
<p>
The <strong>mixed venous oxygen saturation (SvO<sub>2</sub>)</strong>, measured from the pulmonary artery
via a PAC, is a global indicator of the balance between oxygen delivery (DO<sub>2</sub>) and oxygen
consumption (VO<sub>2</sub>).
</p>
<table>
<thead><tr><th>SvO<sub>2</sub> Value</th><th>Interpretation</th></tr></thead>
<tbody>
<tr><td>Normal: 65 – 75%</td><td>Adequate global O<sub>2</sub> delivery/consumption balance</td></tr>
<tr><td>Low: < 65%</td><td>Global O<sub>2</sub> delivery deficient — low cardiac output, severe anaemia, high metabolic demand</td></tr>
<tr><td>High: > 75 – 80%</td><td>Distributive shock (e.g. sepsis), impaired tissue O<sub>2</sub> extraction, or high-flow states</td></tr>
</tbody>
</table>
<p><strong>Fick's Principle</strong> — cardiac output estimation using SvO<sub>2</sub>:</p>
<div class="formula">CO = VO<sub>2</sub> / (CaO<sub>2</sub> − CvO<sub>2</sub>)</div>
<ul>
<li><strong>Important limitation:</strong> SvO<sub>2</sub> is a <em>global</em> measure. Organ-specific ischaemia may be present even with a normal or elevated mixed venous saturation.</li>
</ul>
<p class="src">— Miller's Anesthesia 10e, p. 833–835</p>
<h3>Central Venous O<sub>2</sub> Saturation (ScvO<sub>2</sub>) vs. Mixed Venous (SvO<sub>2</sub>)</h3>
<table>
<thead><tr><th></th><th>ScvO<sub>2</sub> (SVC / right atrium)</th><th>SvO<sub>2</sub> (pulmonary artery)</th></tr></thead>
<tbody>
<tr><td><strong>Access</strong></td><td>Central venous catheter</td><td>Pulmonary artery catheter (PAC)</td></tr>
<tr><td><strong>Represents</strong></td><td>Upper body + cerebral flow</td><td>Entire body</td></tr>
<tr><td><strong>Normal value</strong></td><td>~70 – 80%</td><td>~65 – 75%</td></tr>
<tr><td><strong>Reliability</strong></td><td>Variable; NOT a reliable SvO<sub>2</sub> surrogate</td><td>Gold standard</td></tr>
</tbody>
</table>
<ul>
<li>Monitoring of ScvO<sub>2</sub> was previously part of the <strong>Surviving Sepsis Campaign</strong>, but failure to demonstrate clinical benefit led to its <strong>removal from the 2016 guidelines</strong>.</li>
</ul>
<p class="src">— Tintinalli's, p. 308 | Miller's Anesthesia, p. 835</p>
<!-- 6. A-V DIFFERENCES -->
<h2>6. Arteriovenous Differences — Why They Exist</h2>
<p>
Venous blood is lower in O<sub>2</sub> and higher in CO<sub>2</sub> because tissues extract oxygen
and produce CO<sub>2</sub>. These differences widen significantly in low-flow states (shock, heart failure).
</p>
<table>
<thead><tr><th>Parameter</th><th>Arterial</th><th>Venous</th><th>Normal A-V Difference</th></tr></thead>
<tbody>
<tr><td>pH</td><td>7.35 – 7.45</td><td>~0.03–0.05 lower</td><td>Vein is more acidic</td></tr>
<tr><td>PCO<sub>2</sub> (mmHg)</td><td>35 – 45</td><td>~40 – 50</td><td>3 – 8 mmHg higher venously</td></tr>
<tr><td>PO<sub>2</sub> (mmHg)</td><td>80 – 100</td><td>~35 – 45</td><td>~50 – 60 mmHg lower venously</td></tr>
<tr><td>HCO<sub>3</sub><sup>−</sup> (mEq/L)</td><td>22 – 26</td><td>~24 – 29</td><td>~2 – 3 mEq/L higher venously</td></tr>
</tbody>
</table>
<!-- 7. PRE-ANALYTICAL ERRORS -->
<h2>7. Pre-Analytical Errors Affecting VBG Accuracy</h2>
<table>
<thead><tr><th>Error</th><th>Effect on Values</th></tr></thead>
<tbody>
<tr><td><strong>Air exposure</strong></td><td>Decreases PCO<sub>2</sub>, raises pH, gradually decreases CO<sub>2</sub> content</td></tr>
<tr><td><strong>Saline/fluid dilution</strong> (e.g. flush line)</td><td>PCO<sub>2</sub> and HCO<sub>3</sub><sup>−</sup> both fall equally</td></tr>
<tr><td><strong>Hypothermia</strong> (no temperature correction)</td><td>Spuriously higher PCO<sub>2</sub>, lower pH, higher PO<sub>2</sub></td></tr>
<tr><td><strong>Hyperthermia</strong> (no temperature correction)</td><td>Opposite of hypothermia effects</td></tr>
<tr><td><strong>Delayed analysis</strong></td><td>Continued cellular metabolism alters all values</td></tr>
</tbody>
</table>
<p class="src">— Murray & Nadel's, p. 2274–2278</p>
<!-- 8. CLINICAL APPLICATIONS -->
<h2>8. Clinical Applications</h2>
<h3>Emergency Medicine</h3>
<ul>
<li><strong>Respiratory failure screening:</strong> A normal venous PCO<sub>2</sub> excludes hypercapnic failure. If severe hypercapnia or hypoxia, confirm with ABG.</li>
<li><strong>DKA monitoring:</strong> VBG correlates well with ABG for pH/HCO<sub>3</sub><sup>−</sup>, avoiding repeated arterial punctures.</li>
<li><strong>Toxicology:</strong> VBG used alongside electrolytes in phenol exposure and toxic ingestions.</li>
<li><strong>Paediatric assessment:</strong> VBG used with glucose, ammonia, and metabolic panel in metabolic emergencies.</li>
</ul>
<h3>Critical Care / ICU</h3>
<ul>
<li><strong>Acid-base monitoring:</strong> Central VBGs have excellent agreement with ABGs for acid-base assessment, including in patients in shock.</li>
<li><strong>Sepsis:</strong> ScvO<sub>2</sub> monitoring (no longer a Surviving Sepsis Campaign recommendation as of 2016).</li>
<li><strong>Haemorrhagic shock:</strong> VBG alongside TEG and type-and-screen prioritised in severe haemorrhagic shock.</li>
<li><strong>COPD exacerbation:</strong> VBG recommended as initial blood gas; follow with ABG if severe hypercapnia or hypoxia.</li>
</ul>
<h3>Surgery / Anaesthesia</h3>
<ul>
<li>Continuous SvO<sub>2</sub> monitoring via PAC in high-risk surgical patients provides real-time assessment of global perfusion adequacy.</li>
</ul>
<p class="src">— Tintinalli's, p. 304–310 | Rosen's EM, p. 2550 | Fishman's Pulmonary Diseases, p. 2060–2061</p>
<!-- 9. DECISION TABLE -->
<h2>9. VBG vs. ABG — When to Choose Which</h2>
<table>
<thead><tr><th>Clinical Question</th><th>Recommended Test</th></tr></thead>
<tbody>
<tr><td>Is oxygenation adequate?</td><td>ABG or SpO<sub>2</sub> — VBG cannot assess this</td></tr>
<tr><td>Is the patient hypercapnic?</td><td>VBG first; normal excludes hypercapnia. Confirm ABG if elevated or severe</td></tr>
<tr><td>What is the acid-base status?</td><td>VBG is acceptable (pH ±0.03–0.05)</td></tr>
<tr><td>Is bicarbonate normal?</td><td>VBG (HCO<sub>3</sub><sup>−</sup> ~2–3 mEq/L higher than arterial)</td></tr>
<tr><td>Is lactate elevated?</td><td>VBG for screening; mildly elevated should be confirmed with ABG</td></tr>
<tr><td>Is global O<sub>2</sub> delivery adequate?</td><td>Mixed SvO<sub>2</sub> from PAC (or ScvO<sub>2</sub> as a trend)</td></tr>
<tr><td>Hypotensive / severely hypercapnic patient</td><td>ABG preferred; VBG unreliable in this setting</td></tr>
</tbody>
</table>
<!-- 10. FORMULAS -->
<h2>10. Key Formulas</h2>
<h3>Winter's Equation — Expected PaCO<sub>2</sub> in metabolic acidosis</h3>
<div class="formula">PaCO<sub>2</sub> = (1.5 × [HCO<sub>3</sub><sup>−</sup>] + 8) ± 2</div>
<p>A measured PaCO<sub>2</sub> <em>above</em> the expected value indicates an inadequate ventilatory response to the metabolic acidosis.</p>
<h3>Fick Equation — Cardiac output from mixed venous saturation</h3>
<div class="formula">CO = VO<sub>2</sub> / (CaO<sub>2</sub> − CvO<sub>2</sub>)</div>
<p>Requires SvO<sub>2</sub> measured at the pulmonary artery.</p>
<h3>Dead Space Fraction — Requires ABG</h3>
<div class="formula">V<sub>D</sub>/V<sub>T</sub> = (PaCO<sub>2</sub> − P<sub>E</sub>CO<sub>2</sub>) / PaCO<sub>2</sub></div>
<p>P<sub>E</sub>CO<sub>2</sub> is the mean expired partial pressure of CO<sub>2</sub>, measured by metabolic monitor or capnography in mechanically ventilated patients.</p>
<!-- 11. SUMMARY TABLE -->
<h2>11. Summary Comparison Table</h2>
<table>
<thead><tr><th>Feature</th><th>VBG</th><th>ABG</th></tr></thead>
<tbody>
<tr><td>Invasiveness</td><td>Low (venipuncture)</td><td>Higher (arterial puncture)</td></tr>
<tr><td>Pain</td><td>Minimal</td><td>Moderate</td></tr>
<tr><td>pH accuracy</td><td>Good (±0.03–0.05)</td><td>Reference standard</td></tr>
<tr><td>PCO<sub>2</sub></td><td>~3–8 mmHg higher than arterial</td><td>Reference</td></tr>
<tr><td>PO<sub>2</sub> / Oxygenation</td><td>❌ Not useful</td><td>✅ Required for O<sub>2</sub> assessment</td></tr>
<tr><td>HCO<sub>3</sub><sup>−</sup></td><td>~2–3 mEq/L higher</td><td>Reference</td></tr>
<tr><td>Lactate</td><td>Acceptable (screen); confirm if mildly elevated</td><td>More accurate</td></tr>
<tr><td>Use in shock / hypotension</td><td>⚠ Unreliable</td><td>✅ Preferred</td></tr>
<tr><td>Mixed venous O<sub>2</sub> (SvO<sub>2</sub>)</td><td>Via PAC only</td><td>N/A</td></tr>
</tbody>
</table>
<!-- REFERENCES -->
<div class="refs">
<h3>References</h3>
<ul>
<li>Tintinalli's Emergency Medicine: A Comprehensive Study Guide, pp. 304–310</li>
<li>Murray & Nadel's Textbook of Respiratory Medicine, pp. 2270–2282</li>
<li>Goldman-Cecil Medicine International Edition, p. 754</li>
<li>Fishman's Pulmonary Diseases and Disorders, p. 2060</li>
<li>Miller's Anesthesia 10th Edition, pp. 833–835</li>
<li>Rosen's Emergency Medicine: Concepts and Clinical Practice, pp. 2550–2551</li>
<li>Harrison's Principles of Internal Medicine 22E (2025)</li>
</ul>
</div>
<div class="footer">Venous Blood Gases — Orris Medical Reference | June 2026</div>
</body>
</html>
libreoffice --headless --convert-to pdf /home/daytona/workspace/vbg-pdf/vbg.html --outdir /home/daytona/workspace/vbg-pdf/ 2>&1
cp /home/daytona/workspace/vbg-pdf/vbg.html /tmp/vbg.html && libreoffice --headless --convert-to pdf /tmp/vbg.html --outdir /tmp/ 2>&1 && cp /tmp/vbg.pdf /home/daytona/workspace/vbg-pdf/Venous_Blood_Gases.pdf && ls -lh /home/daytona/workspace/vbg-pdf/Venous_Blood_Gases.pdf
Venous Blood Gases
PDF Document · PDF

ECG analysis of this in detail
ECG Analysis Report
Patient Information
| Field | Details |
|---|---|
| Name | Shabeer |
| ID | 53336 |
| Age/Sex | 43 years, Male |
| Date/Time | 23-06-2026, 09:13:14 AM |
| Settings | 0.67-35 Hz filter, AC50, 25 mm/s paper speed, 10 mm/mV gain |
Automated Measurements
| Parameter | Value | Normal Range |
|---|---|---|
| Heart Rate (HR) | 111 bpm | 60-100 bpm |
| PR interval | 134 ms | 120-200 ms |
| QRS duration | 103 ms | <120 ms |
| P axis | 93 ms | -- |
| QRS-T (QTc/QT) | 353/477 ms | QTc <440 ms (men) |
| RVS/SV1 | 0.264/0.621 mV | -- |
Automated Machine Diagnosis
- Sinus Tachycardia
- Larced PtV1 (Large P terminal velocity in V1 - suggesting left atrial enlargement)
- Limited Right Bundle Branch Block (incomplete RBBB)
- T Wave Abnormality (aVL, V1, V2)
- Prolonged QT Interval
Systematic Lead-by-Lead Analysis
Rhythm Analysis
- Rhythm: Regular sinus rhythm
- Rate: ~111 bpm - Sinus tachycardia (rate >100 bpm with visible P waves before every QRS)
- P waves: Present and upright in leads I, II, aVF - confirming sinus origin. P terminal force appears prominent in V1 (large negative terminal component), suggesting left atrial abnormality/enlargement
- PR interval: 134 ms - normal (120-200 ms range)
- P-QRS relationship: 1:1 conduction maintained throughout
QRS Complex
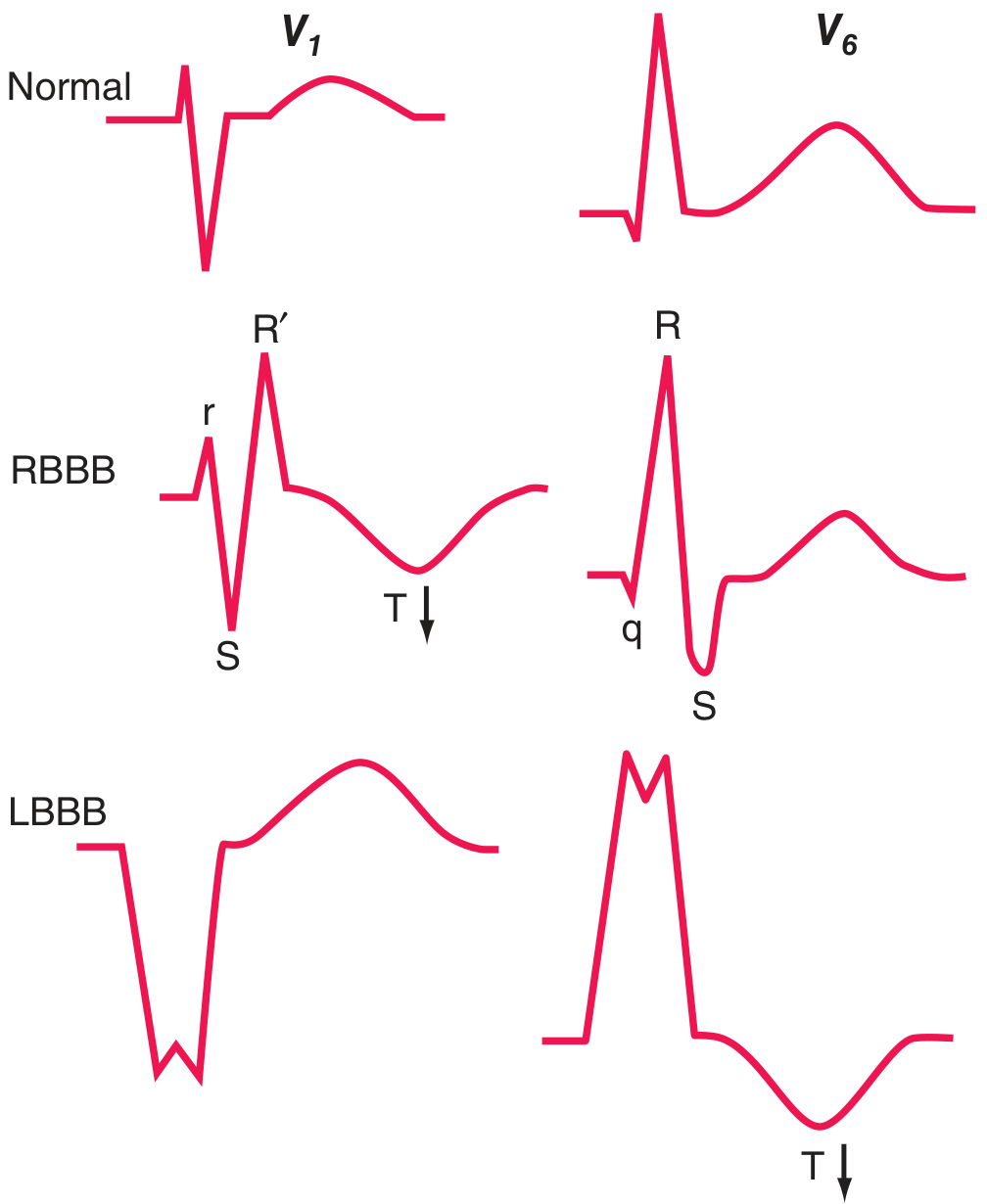
- Duration: 103 ms - this is borderline/mildly prolonged. It is below 120 ms, which places this in the incomplete RBBB category rather than complete RBBB
- Morphology in V1-V2: The characteristic rSR' ("M-shaped") pattern is visible in V1-V2, consistent with delayed right ventricular activation
- Morphology in V5-V6 / Lead I: Wide, slurred S waves are expected (and present) in the lateral leads, confirming the RBBB pattern
- Axis: The overall QRS axis appears to be normal (positive in leads I and II)
- QRS duration 100-119 ms (103 ms here) ✓
- RSR' or rSR' pattern in V1-V2 ✓
- Slurred S wave in leads I and V6 ✓
Incomplete RBBB is often a normal variant, especially in younger individuals and athletes. However, in a 43-year-old male presenting with tachycardia, causes such as right ventricular pressure overload (pulmonary embolism, pulmonary hypertension), atrial septal defect, or ischaemia should be excluded clinically.
Repolarisation / ST-T Changes
- T wave inversions in aVL, V1, V2 - reported by machine and visible on tracing
- In RBBB, secondary T-wave inversions in right precordial leads (V1-V2) are expected and are a normal consequence of the altered depolarisation sequence - these are "discordant" T waves (opposite to the terminal QRS deflection)
- T wave inversion in aVL is a separate finding and can reflect:
- Left ventricular lateral wall ischaemia/strain
- Normal variant in high lateral leads
- Right ventricular strain pattern
QT / QTc Interval
- QT measured: 353 ms
- QTc (corrected): 477 ms
- Normal QTc for men: ≤440 ms; borderline up to 460 ms; >500 ms = high risk
- This patient's QTc of 477 ms is prolonged (above the 440 ms male threshold)
| Category | Examples |
|---|---|
| Electrolyte abnormalities | Hypokalaemia, hypomagnesaemia, hypocalcaemia |
| Medications | Antiarrhythmics (amiodarone, sotalol), antibiotics (azithromycin, fluoroquinolones), antipsychotics, antihistamines |
| Cardiac | Myocarditis, cardiomyopathy, ischaemia |
| Congenital | Long QT syndrome (LQTS type 1, 2, 3) |
| Autonomic | Raised intracranial pressure, hypothyroidism |
Individual Lead Summary
| Lead | Key Finding |
|---|---|
| I | Upright P, normal QRS, slurred S wave (RBBB) |
| II | Upright P wave; sinus tachycardia confirmed |
| III | Small complexes, normal |
| aVR | Inverted P and QRS (normal for aVR) |
| aVL | T wave inversion - lateral/high lateral repolarisation abnormality |
| aVF | Normal, positive QRS |
| V1 | rSR' pattern (RBBB), T wave inversion (secondary/expected), large negative P terminal component (left atrial enlargement) |
| V2 | rSR' with T wave inversion (RBBB secondary change) |
| V3 | Transitional zone |
| V4 | Normal transition |
| V5 | Wide S wave (RBBB), upright T |
| V6 | Slurred S wave (RBBB), upright T |
Summary of Findings
| Finding | Classification | Significance |
|---|---|---|
| Sinus tachycardia (111 bpm) | Abnormal | Requires clinical cause (pain, fever, anxiety, PE, thyrotoxicosis, dehydration, anaemia) |
| Incomplete RBBB (QRS 103 ms) | Abnormal / may be normal variant | Exclude RV pressure overload, ASD, ischaemia |
| T wave inversions (aVL, V1, V2) | V1-V2: secondary to RBBB (expected); aVL: needs correlation | Rule out lateral ischaemia if new |
| Prolonged QTc (477 ms) | Abnormal | Check electrolytes (K+, Mg2+, Ca2+), medications, LQTS; JTc preferred in RBBB |
| Large P terminal force V1 | Suggestive | Left atrial abnormality / enlargement - consider echocardiogram |
RBBB Morphology Reference
Clinical Recommendations
- Check electrolytes - K+, Mg2+, Ca2+ urgently to address the prolonged QTc
- Review medications - identify and stop any QT-prolonging agents
- Treat the tachycardia - identify and treat the underlying cause (fever, pain, hypovolaemia, PE, thyroid disease)
- Echocardiogram - to evaluate for structural heart disease, RV pressure overload, atrial septal defect, or cardiomyopathy given the RBBB
- Troponin / ischaemia workup - if new RBBB with chest pain, rule out ACS or PE
- Compare with prior ECGs - to determine if RBBB is new or chronic
- Cardiology referral - for QTc >470 ms in a male with structural findings warranting further evaluation
⚠️ Disclaimer: This analysis is based on the machine printout and visual tracing. All ECG findings must be clinically correlated by the treating physician. This report does not replace formal cardiologist review.
Immune thrombocytopenic purpura diagnosis treatment pathology etiology
dengue, shigella lepto brusellosis in detail
Quick Clinical Pearls
- "Breakbone fever" + retro-orbital pain + morbilliform rash + thrombocytopenia after defervescence = classic
- Never give aspirin or NSAIDs
- DHF requires ALL 4 WHO criteria; DSS = DHF + shock
- Lowest infectious dose of any enteric pathogen (~10 organisms)
- Bloody diarrhoea + tenesmus + pus cells in stool = bacillary dysentery
- Unlike EHEC, antibiotics ARE indicated and reduce disease duration
- Avoid antidiarrhoeals
- Conjunctival suffusion (not exudate - redness without discharge) is the pathognomonic bedside sign
- Think lepto in any febrile patient who swam in floodwater or had rodent/animal exposure
- MAT (Microscopic Agglutination Test) is the gold standard serology
- Jarisch-Herxheimer reaction possible with first antibiotic dose
- Undulant fever + profuse night sweats + musculoskeletal pain in someone who ate unpasteurised cheese or works with livestock
- Always combination therapy (never monotherapy) - 6 weeks minimum
- Spondylodiscitis in lower lumbar spine - differentiate from TB (which has more vertebral destruction and psoas abscess)
- Blood culture requires extended incubation up to 6 weeks
Liver cirrhosis diagnosis, treatment, pathophysiology, etiology
Liver Cirrhosis: Etiology, Pathophysiology, Diagnosis & Treatment
Gross Pathology

Definition
- Not all chronic liver disease terminates in cirrhosis
- Not all cirrhosis leads to end-stage liver disease (e.g. cured Hep C may have adequate function despite cirrhosis)
- Regression of established cirrhosis is possible following disease remission or cure
1. Etiology
Main Causes (>95% of cases)
| Cause | Key Features |
|---|---|
| Alcoholic liver disease (ALD) | Dose and duration dependent; steatohepatitis → fibrosis → cirrhosis |
| Non-alcoholic fatty liver disease (NAFLD) / MASH | Metabolic syndrome; increasingly the most common cause globally |
| Chronic hepatitis B (HBV) | Direct cytopathic + immune-mediated injury; can lead to cirrhosis even without inflammation |
| Chronic hepatitis C (HCV) | Immune-mediated; decades of smouldering fibrosis |
Other Causes (≤2% individually)
- Primary biliary cholangitis (PBC)
- Primary sclerosing cholangitis (PSC)
- Autoimmune hepatitis (AIH)
- Biliary atresia / intrahepatic/extrahepatic biliary obstruction
- Hereditary haemochromatosis (iron overload)
- Wilson disease (copper accumulation)
- α1-antitrypsin deficiency
- Glycogen storage diseases, porphyria, abetalipoproteinaemia
- Budd-Chiari syndrome (hepatic vein thrombosis)
- Veno-occlusive disease
- Right-sided heart failure (cardiac cirrhosis)
- Drugs/toxins (methotrexate, amiodarone, vitamin A)
- Intestinal bypass
- Indian childhood cirrhosis
- Cryptogenic cirrhosis - no clear cause identified
2. Pathophysiology
Step 1 - Hepatocellular Injury
- Hepatocyte necrosis/apoptosis
- Release of reactive oxygen species (ROS), cytokines (TGF-β1, TNF-α, IL-1, IL-6, PDGF)
- Kupffer cell (resident macrophage) and inflammatory cell activation
Step 2 - Hepatic Stellate Cell (HSC) Activation - The Central Event
- Hepatic stellate cells (Ito cells / perisinusoidal cells) normally reside in the space of Disse between hepatocytes and sinusoidal endothelial cells
- In their quiescent state, HSCs are the main storage site for retinoids (vitamin A)
- In response to injury, HSCs become activated (transdifferentiate into myofibroblasts):
- Lose vitamin A droplets
- Proliferate
- Develop prominent rough endoplasmic reticulum
- Secrete extracellular matrix (collagen types I and III, proteoglycans, glycoproteins)
- Become contractile (can constrict sinusoids → increased vascular resistance)
Step 3 - Sinusoidal Remodelling ("Capillarisation")
- Defenestration of sinusoidal endothelial cells ("capillarisation of sinusoids")
- Decreased molecular exchange between plasma and hepatocytes
- Sinusoidal narrowing → increased resistance to portal flow
Step 4 - Nodule Formation & Fibrosis
- Fibrous bands link portal tracts to each other and to central veins
- Surviving hepatocytes undergo regenerative proliferation → nodule formation
- Nodules surrounded by fibrosis = cirrhosis
| Nodule Type | Size | Associated Cause |
|---|---|---|
| Micronodular | <3 mm | Alcoholic cirrhosis, haemochromatosis, biliary cirrhosis |
| Macronodular | >3 mm | Viral hepatitis, autoimmune |
| Mixed | Both | Any advanced cirrhosis |
Step 5 - Portal Hypertension Development
- Fixed component - fibrosis + regenerative nodule compression of sinusoids (not amenable to drugs)
- Functional component - active vasoconstriction due to:
- Deficiency of intrahepatic NO (nitric oxide)
- Excess vasoconstrictors (endothelin, angiotensin II)
- Splanchnic vasodilation driven by excess extrahepatic NO production
- Collateral vessels reverse flow (e.g. coronary vein) → portosystemic shunts
- Shunts are insufficient to decompress portal system
- Intrahepatic: NO deficiency → vasoconstriction → increased resistance
- Extrahepatic: NO overproduction → vasodilation → increased portal flow
Splanchnic vasodilation → decreased effective arterial blood volume → RAAS + SNS activation → sodium/water retention → expanded plasma volume → hyperdynamic state (↑CO, ↓SVR, ↓MAP)
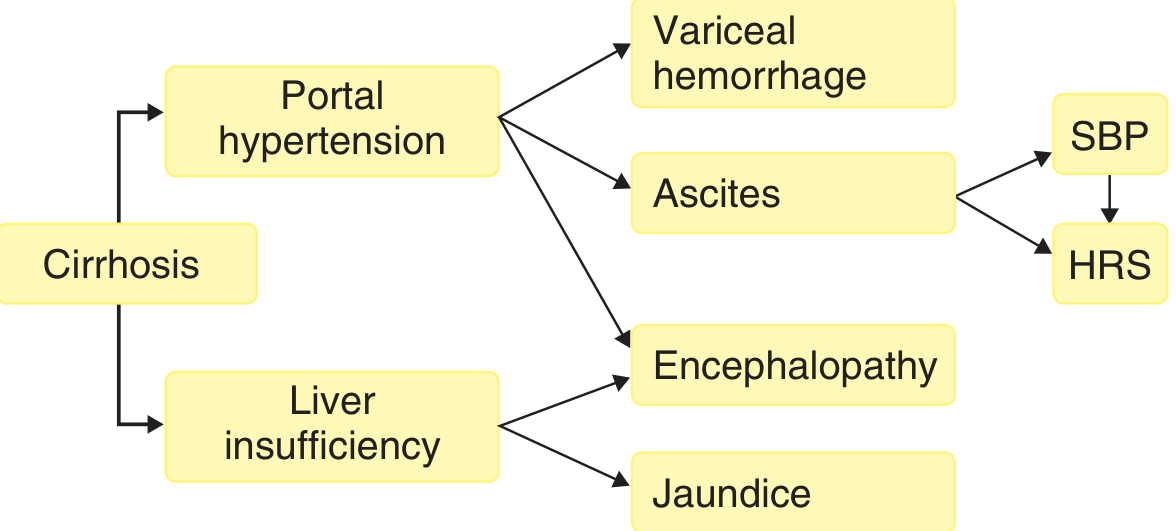
Complications Flowchart
3. Clinical Features
Compensated vs. Decompensated Cirrhosis
| Stage | Features | Median Survival |
|---|---|---|
| Compensated | May be asymptomatic; incidental findings | >12 years |
| Decompensated | Ascites, variceal haemorrhage, encephalopathy, jaundice | ~2 years |
Symptoms & Signs
- Anorexia, weight loss, weakness, fatigue, muscle wasting
- Fever (low-grade)
| Sign | Cause |
|---|---|
| Spider naevi | Dilated cutaneous arterioles (oestrogen ↑) |
| Palmar erythema | Increased oestrogen |
| Caput medusae | Dilated periumbilical collaterals |
| Leukonychia (white nails) | Hypoalbuminaemia |
| Terry's nails | Cirrhosis-specific white nails |
| Dupuytren's contracture | Alcoholic cirrhosis |
| Parotid enlargement | Alcohol |
| Gynaecomastia / testicular atrophy | Feminisation from ↑ oestrogens |
- Hepatomegaly (early) or small shrunken liver (late)
- Splenomegaly (portal hypertension)
- Ascites (shifting dullness, fluid thrill)
- Caput medusae
- Thrombocytopenia (hypersplenism + decreased thrombopoietin)
- Anaemia (multi-factorial: haemolysis, bleeding, folate deficiency)
- Coagulopathy (decreased synthesis of clotting factors II, V, VII, IX, X, XI)
4. Complications in Detail
A. Ascites
- Requires portal pressure (HVPG) threshold of ≥12 mmHg
- Pathogenesis: sinusoidal hypertension + sodium retention (via RAAS/SNS activation from vasodilation)
- Serum-Ascites Albumin Gradient (SAAG): SAAG = serum albumin − ascites albumin
- SAAG ≥1.1 g/dL = portal hypertension (cirrhosis, Budd-Chiari, right heart failure)
- SAAG <1.1 g/dL = non-portal cause (peritoneal carcinomatosis, TB peritonitis)
B. Spontaneous Bacterial Peritonitis (SBP)
- Infection of ascitic fluid without perforation of a viscus or intra-abdominal focus
- Mechanism: bacterial translocation from intestinal lumen through mesenteric lymph nodes + impaired immune defenses + portosystemic shunting bypasses Kupffer cells
- Diagnosis: Ascitic fluid PMN count ≥250 cells/mm³
- Commonest organisms: E. coli, Klebsiella, Streptococcus pneumoniae
- Treatment: Cefotaxime 2g IV q8h × 5 days + IV albumin (1.5 g/kg at diagnosis, 1 g/kg at 72h) - albumin prevents HRS
- Prophylaxis: Norfloxacin 400 mg/day (or ciprofloxacin) in high-risk patients
C. Variceal Haemorrhage
- Varices form when HVPG exceeds 10-12 mmHg; rupture when variceal wall tension reaches a critical point
- Most dreaded complication of portal hypertension
- Mortality per episode: 10-20%
- Acute management:
- Airway protection (intubate if encephalopathic)
- IV terlipressin (or octreotide/somatostatin) - reduce portal pressure
- IV ceftriaxone (antibiotics reduce mortality in variceal bleeding)
- Urgent endoscopy (EVL - endoscopic variceal ligation preferred over sclerotherapy)
- TIPS (transjugular intrahepatic portosystemic shunt) for refractory bleeding
- Primary prophylaxis (before first bleed): Non-selective beta-blockers (propranolol / nadolol / carvedilol) or EVL
- Secondary prophylaxis (after first bleed): Beta-blockers + EVL
D. Hepatic Encephalopathy (HE)
- Caused by portosystemic shunting + liver insufficiency → nitrogenous toxins (ammonia) bypass hepatic detoxification → brain dysfunction
- Precipitants: GI bleeding, infection, sedatives, dehydration, constipation, hyponatraemia, hypokalemia, hepatocellular carcinoma
| Grade | Features |
|---|---|
| 0 (Minimal) | No overt symptoms; neuropsychological testing abnormal |
| 1 | Mild confusion, altered sleep, shortened attention |
| 2 | Lethargy, moderate confusion, asterixis (liver flap) |
| 3 | Stupor, marked confusion, incomprehensible speech |
| 4 | Coma |
- Lactulose 15-45 mL PO bd-qid (1st line); titrate to 3-5 soft stools/day; can be given as enema (300 mL in 700 mL water) if oral route not tolerated
- Rifaximin 550 mg PO bd (add if no response to lactulose in 24h; also used for secondary prevention)
- Treat precipitants; reduce/stop sedatives; adequate nutrition (do NOT restrict protein excessively)
- Zinc supplementation in zinc-deficient patients
E. Hepatorenal Syndrome (HRS)
- Functional renal failure in advanced cirrhosis - no intrinsic renal pathology initially
- Caused by intense renal vasoconstriction from:
- RAAS and SNS over-activation secondary to splanchnic vasodilation
- Decreased effective arterial volume
- Types:
- HRS-AKI (previously Type 1): Rapid progressive renal failure; creatinine doubles to >2.5 mg/dL in <2 weeks; very poor prognosis
- HRS-CKD (previously Type 2): Moderate, steady renal failure; associated with refractory ascites
- Diagnosis: Exclude other causes; no response to volume expansion with albumin; creatinine >1.5 mg/dL
- Treatment:
- Terlipressin + IV albumin (1st line; FDA-approved)
- Alternative: Noradrenaline + albumin (in ICU setting)
- Alternative: Midodrine + octreotide + albumin (where terlipressin unavailable)
- Definitive: Liver transplantation
- TIPS in selected patients
F. Hepatocellular Carcinoma (HCC)
- Risk is markedly elevated in cirrhosis, especially with HBV, HCV, alcoholic, haemochromatosis
- Surveillance: Liver USS every 6 months ± AFP in all cirrhotic patients
- HCC suspected in a cirrhotic patient who develops sudden decompensation
5. Diagnosis
Clinical Assessment
Laboratory Tests
| Test | Finding in Cirrhosis |
|---|---|
| ALT/AST | May be normal in advanced cirrhosis (burnt-out liver) |
| ALP/GGT | Elevated (cholestatic component) |
| Bilirubin | Elevated (failure of excretion) |
| Albumin | Decreased (synthetic failure) - useful prognostic marker |
| Prothrombin time / INR | Prolonged (decreased clotting factor synthesis) |
| Platelets | Decreased (hypersplenism + decreased thrombopoietin) |
| Sodium | Hyponatraemia (dilutional) |
| Creatinine | Elevated if HRS developing |
| Ammonia | Elevated in HE (not sensitive/specific alone) |
| AFP | Screen for HCC |
- Viral serology: HBsAg, HBcore Ab, anti-HCV, HCV RNA
- Autoimmune: ANA, ASMA, AMA (primary biliary)
- Metabolic: Serum ferritin + transferrin saturation (haemochromatosis), ceruloplasmin (Wilson), α1-AT level
Non-Invasive Fibrosis Markers
- FIB-4 score: Age × AST / (platelet count × √ALT) - widely used
- APRI (AST-to-Platelet Ratio Index)
- FibroTest / FibroSure: Combination of blood tests
- Elastography (transient - FibroScan): Measures liver stiffness; most commonly used; can eliminate need for biopsy when fibrosis staging is the only indication
Imaging
| Modality | Findings in Cirrhosis |
|---|---|
| Ultrasound | Nodular/heterogeneous echogenicity; small liver; splenomegaly; ascites; portal vein dilation; reversed portal flow |
| CT (triple phase) | Nodularity; hypertrophied caudate lobe; splenomegaly; varices; ascites; can detect HCC |
| MRI | Superior soft tissue characterisation; MR elastography for fibrosis staging |
| Upper GI endoscopy | Gold standard for varices; grade and risk-stratify oesophageal varices |
Liver Biopsy
- Gold standard for diagnosis, grading (activity), and staging (fibrosis)
- Required: minimum 1.5-2 cm length with 10 portal tracts for accurate fibrosis assessment
- Histologic findings: regenerative nodules, fibrous bands, disrupted architecture, ductular reactions
- Scoring systems: METAVIR (F0-F4), Histology Activity Index (HAI/Knodell)
- Now less often needed when elastography is available
Prognostic Scoring Systems
| Component | 1 point | 2 points | 3 points |
|---|---|---|---|
| Bilirubin (mg/dL) | ≤2 | 2-3 | ≥3 |
| INR | ≤1.6 | 1.7-2.2 | ≥2.3 |
| Albumin (g/dL) | ≥3.5 | 2.8-3.5 | ≤2.7 |
| Ascites | None | Slight | Moderate |
| Hepatic encephalopathy | None | Grade 1-2 | Grade 3-4 |
| Class | Score | 1-yr Survival | 2-yr Survival |
|---|---|---|---|
| A (Compensated) | 5-6 | 100% | 85% |
| B (Significant dysfunction) | 7-9 | 80% | 60% |
| C (Decompensated) | 10-15 | 45% | 35% |
MELD = 3.78 × ln[bilirubin mg/dL] + 11.2 × ln[INR] + 9.57 × ln[creatinine mg/dL] + 6.43
- Predicts 90-day mortality without transplant
- Used for organ allocation in transplant waiting lists
- MELD-Na incorporates serum sodium (adds prognostic value)
- MELD <16 = lower surgical mortality; MELD ≥16 = significantly increased risk
6. Treatment
A. Treat the Underlying Cause
| Cause | Disease-Modifying Treatment |
|---|---|
| Alcoholic liver disease | Complete alcohol cessation; nutritional support; prednisolone (severe alcoholic hepatitis) |
| HCV | Direct-acting antivirals (DAAs) - >95% cure rate; fibrosis may regress after SVR |
| HBV | Tenofovir or entecavir (suppress viral replication; slow fibrosis) |
| NAFLD/MASH | Weight loss ≥7-10%; bariatric surgery; GLP-1 agonists; resmetirom (first approved drug for MASH) |
| Haemochromatosis | Phlebotomy (reduce iron); chelation |
| Wilson disease | Penicillamine or trientine (copper chelation); zinc |
| Autoimmune hepatitis | Prednisolone ± azathioprine |
| PBC | Ursodeoxycholic acid (UDCA) 13-15 mg/kg/day; obeticholic acid (2nd line) |
| PSC | UDCA (controversial); endoscopic stricture management; transplant |
B. Management of Ascites
- Dietary sodium restriction: 2000 mg (88 mmol) sodium/day
- Diuretics (1st line):
- Spironolactone 100 mg/day (MRA - blocks aldosterone-driven sodium retention)
- Furosemide 40 mg/day
- Ratio maintained at 100 mg:40 mg (spiro:furo) during dose escalation
- Maximum: Spironolactone 400 mg/day + Furosemide 160 mg/day
- Target weight loss: ≤0.5 kg/day (no oedema); ≤1 kg/day (with oedema)
- Avoid ACE inhibitors/ARBs (cause hypotension in cirrhosis)
- Large-volume paracentesis (LVP): For refractory ascites; >5 L → give IV albumin 8 g/L fluid removed (prevents post-paracentesis circulatory dysfunction)
- Transjugular intrahepatic portosystemic shunt (TIPS): For refractory ascites unresponsive to diuretics; creates portosystemic shunt to reduce portal pressure
- Fluid restriction: Only if serum sodium <125 mmol/L
C. Management of Variceal Bleeding
D. Management of Hepatic Encephalopathy
- Identify and treat precipitants (GI bleed, infection, drugs, electrolyte disturbance, constipation)
- Lactulose 15-45 mL bd-qid PO; target 3-5 soft stools/day (1st line)
- Rifaximin 550 mg bd (add to lactulose for acute episodes; use for secondary prevention of recurrence)
- Nutrition: Adequate protein (1.2-1.5 g/kg/day); small frequent meals; late evening snack
- Zinc supplementation for deficient patients
E. Liver Transplantation
- Definitive treatment for end-stage cirrhosis
- Indications: MELD ≥15; decompensated cirrhosis (Child-Pugh B/C); hepatorenal syndrome; refractory variceal bleeding; HCC within Milan criteria
- Contraindications: Active alcohol/substance use, extrahepatic malignancy, severe cardiopulmonary disease, uncontrolled sepsis
- Milan criteria for HCC: Single lesion ≤5 cm OR ≤3 lesions each ≤3 cm, no vascular invasion, no extrahepatic disease
- Post-transplant: Immunosuppression (tacrolimus ± mycophenolate); recurrence risk for HBV/HCV/alcoholic
F. General Supportive Measures
- Hepatitis A and B vaccination (if not immune)
- Avoid hepatotoxic drugs: NSAIDs (worsen renal function), aminoglycosides, opioids (precipitate HE), sedatives/benzodiazepines
- Nutritional support: Malnutrition worsens prognosis; protein intake should NOT be restricted
- HCC surveillance: Liver USS every 6 months
- Anaemia: Identify and treat cause; avoid iron supplementation unless clear deficiency
Summary: Compensated vs. Decompensated Cirrhosis
| Feature | Compensated | Decompensated |
|---|---|---|
| Definition | No major complications | Ascites, variceal haemorrhage, HE, or jaundice |
| Portal pressure (HVPG) | <12 mmHg or threshold | ≥12 mmHg |
| Median survival | >12 years | ~2 years |
| Mechanism | Fibrosis + early portal HTN | Portal HTN + hyperdynamic state + liver failure |
| Priority | Treat underlying cause | Manage complications + transplant evaluation |
Basics of pharmacology and drug names
Basics of Pharmacology and Drug Names
What Is Pharmacology?
| Branch | Definition | Mnemonic |
|---|---|---|
| Pharmacokinetics | What the body does to the drug | PK = body acts on drug |
| Pharmacodynamics | What the drug does to the body | PD = drug acts on body |
PART 1: PHARMACOKINETICS (PK)
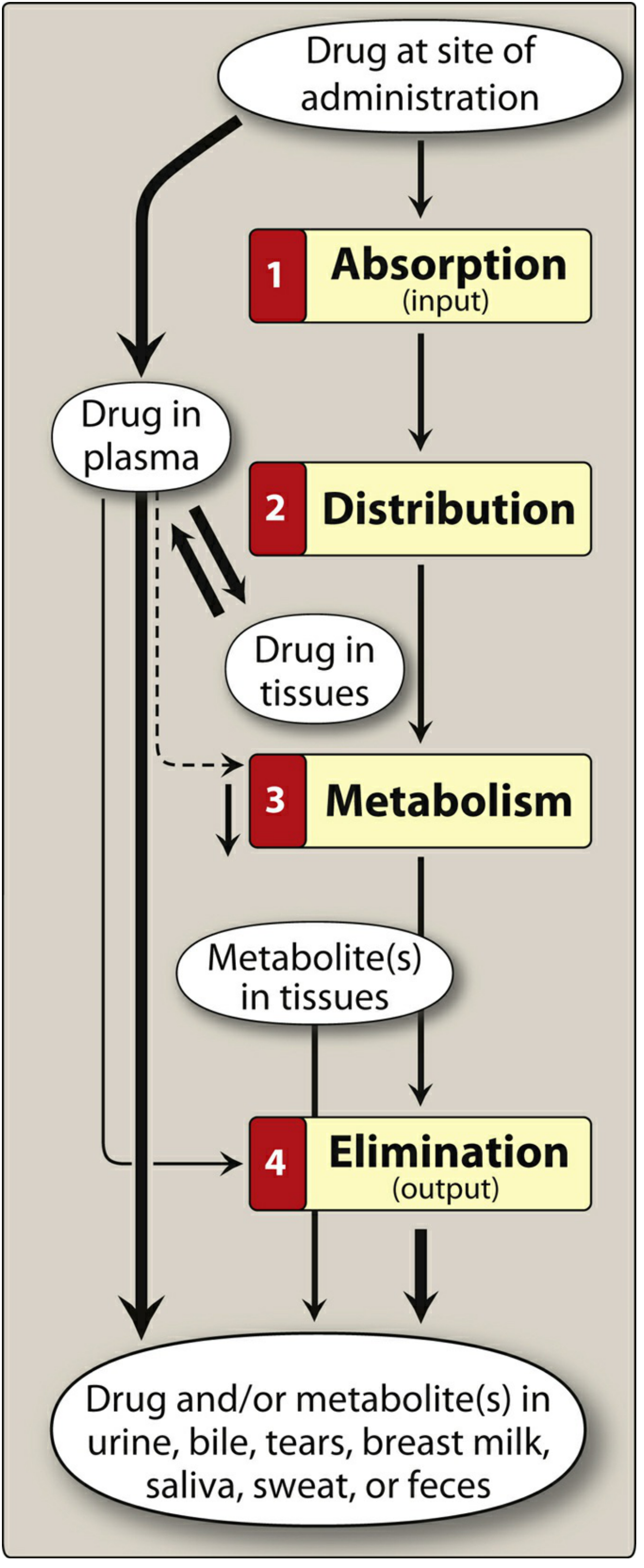
1. Absorption
Routes of Administration
| Route | Key Features | Example Drugs |
|---|---|---|
| Oral (PO) | Most common, convenient, economical; subject to first-pass metabolism; food may affect absorption | Acetaminophen, amoxicillin, metformin |
| Sublingual (SL) | Under tongue; bypasses first-pass effect; rapid systemic absorption | Nitroglycerin (GTN) |
| Buccal | Between gum and cheek | Fentanyl buccal tablets |
| Intravenous (IV) | 100% bioavailability; fastest onset; no absorption step | Penicillin G, morphine, vancomycin |
| Intramuscular (IM) | Intermediate absorption; depot formulations possible | Vaccines, depot antipsychotics |
| Subcutaneous (SC) | Slower than IM; sustained release possible | Insulin, heparin, adalimumab |
| Inhalation | Direct delivery to lungs; rapid onset; minimises systemic side effects | Salbutamol, fluticasone |
| Transdermal | Slow systemic absorption; sustained release; rate depends on skin lipid solubility | Fentanyl patch, nicotine patch, GTN patch |
| Rectal | 50% bypasses portal circulation; useful when oral not possible | Diazepam rectal (seizures), some antiemetics |
| Intrathecal | Direct CNS delivery (bypasses blood-brain barrier) | Spinal anaesthesia, intrathecal methotrexate |
| Topical | Local effect at application site | Hydrocortisone cream, eye drops |
Mechanism of Membrane Crossing
Ionised (charged) drugs cannot cross lipid membranes. Non-ionised (uncharged) drugs cross freely.
- Weak acids (e.g. aspirin, warfarin): non-ionised in acid environments → absorbed better from stomach (low pH)
- Weak bases (e.g. morphine, codeine): non-ionised in alkaline environments → absorbed better from small intestine (higher pH)
First-Pass Effect (Hepatic First-Pass Metabolism)
- Reduces bioavailability of oral drugs (e.g. oral morphine has ~30% bioavailability vs IV)
- Explains why some drugs are given sublingually, IV, or transdermally to bypass this
Bioavailability (F)
F = (AUC oral / AUC IV) × 100%
- IV administration = 100% bioavailability by definition
- Oral bioavailability varies widely: nitroglycerin ~1% (oral) vs. >95% (sublingual)
2. Distribution
Plasma Protein Binding
- Most drugs bind reversibly to plasma proteins (mainly albumin)
- Only free (unbound) drug is pharmacologically active and can cross membranes
- Bound drug acts as a reservoir; as free drug is eliminated, bound drug dissociates
- Drugs with high protein binding have prolonged action but delayed onset
- Drug interactions: Two highly protein-bound drugs compete for albumin → displaces one drug → sudden rise in free drug → toxicity (e.g. warfarin + aspirin)
Lipophilicity
- Lipophilic drugs cross membranes freely → distribute widely into all tissues
- Hydrophilic drugs cannot cross cell membranes → stay in extracellular fluid
Volume of Distribution (Vd)
Vd = Dose / Initial plasma concentration (C₀)
| Vd | Where Drug Distributes | Example |
|---|---|---|
| ~4 L (plasma only) | High molecular weight or highly protein-bound; stays in vascular compartment | Heparin, large antibodies |
| ~14 L (extracellular fluid) | Small, hydrophilic; crosses capillaries but not cells | Aminoglycosides |
| ~42 L (total body water) | Small, lipophilic; distributes into all body water | Ethanol |
| >100 L (extensive tissue) | Highly lipophilic; sequesters in fat/tissues | Chloroquine, amiodarone |
Blood-Brain Barrier (BBB)
- Most hydrophilic drugs cannot cross the BBB
- Lipophilic drugs (e.g. diazepam, thiopental) cross readily
- Inflamed meninges (e.g. meningitis) increase BBB permeability → allows some drugs that normally wouldn't cross (e.g. penicillin) to enter the CNS
Placental and Breast Milk Transfer
- Lipophilic, low-protein-bound drugs cross the placenta
- Many drugs pass into breast milk - clinical significance varies
3. Metabolism (Biotransformation)
- Convert lipophilic drugs → hydrophilic (water-soluble) compounds for renal excretion
- Usually results in inactivation, but sometimes produces active metabolites
Phase I Reactions ("Functionalisation")
Cytochrome P450 (CYP) System - Most Important
- Superfamily of heme-containing enzymes located mainly in liver and GI tract
- Four isozymes responsible for the vast majority of CYP reactions:
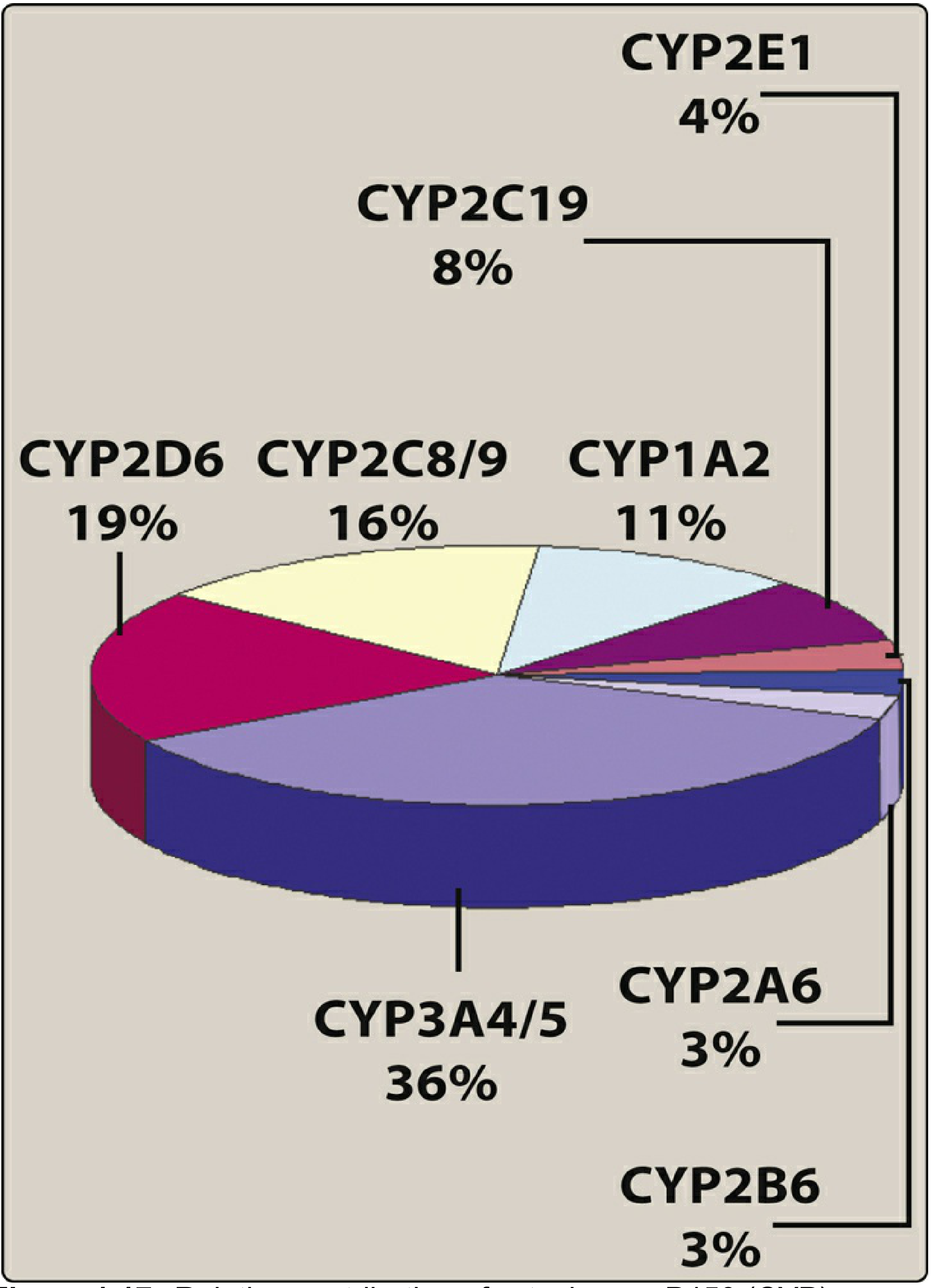
| CYP Isoform | % Drug Metabolism | Key Substrates | Key Inhibitors | Key Inducers |
|---|---|---|---|---|
| CYP3A4/5 | 36% (largest) | Statins, benzodiazepines, cyclosporine, midazolam, many others | Ketoconazole, ritonavir, clarithromycin, grapefruit juice | Rifampicin, carbamazepine, St John's Wort |
| CYP2D6 | 19% | Codeine, β-blockers, antidepressants, antipsychotics | Fluoxetine, paroxetine, haloperidol | (not significantly inducible) |
| CYP2C8/9 | 16% | Warfarin, NSAIDs, sulfonylureas | Fluconazole, amiodarone | Rifampicin |
| CYP1A2 | 11% | Caffeine, theophylline, clozapine | Fluvoxamine, ciprofloxacin | Smoking, omeprazole |
| CYP2C19 | 8% | Omeprazole, clopidogrel (prodrug!), diazepam | Omeprazole, fluoxetine | Rifampicin |
- CYP2D6 has the most important genetic variation
- Poor metabolisers - codeine has no analgesic effect (cannot convert to morphine)
- Ultra-rapid metabolisers - codeine → excessive morphine → respiratory depression
- CYP2C19 poor metabolisers - clopidogrel (a prodrug) is not activated → reduced antiplatelet effect → carry a black box FDA warning
- Key inhibitors: Ketoconazole, ritonavir, clarithromycin (inhibit multiple CYPs)
- Example: Omeprazole inhibits CYP isozymes involved in warfarin metabolism → ↑ warfarin levels → bleeding risk
- Key inducers: Rifampicin, carbamazepine, phenytoin, phenobarbitone, St John's Wort
- Example: Rifampicin induces CYP3A4 → decreases oral contraceptive levels → contraceptive failure
| Prodrug | Active Metabolite |
|---|---|
| Codeine | Morphine (via CYP2D6) |
| Clopidogrel | Active thiol metabolite (via CYP2C19) |
| Enalapril | Enalaprilat |
| Levodopa | Dopamine |
| Prednisone | Prednisolone |
Phase II Reactions (Conjugation)
- Glucuronidation (most common and most important) - via UGT enzymes
- Sulfation
- Acetylation
- Amino acid conjugation (glycine, glutamine)
4. Elimination (Excretion)
Renal Elimination (Most Important)
| Process | Description |
|---|---|
| Glomerular filtration | Free (unbound) drug filters into Bowman's capsule; protein-bound drug stays in blood; GFR ~120 mL/min |
| Active tubular secretion | Carrier-mediated transport of drugs into tubular lumen; can transport protein-bound drug; may saturate |
| Passive tubular reabsorption | Lipophilic, non-ionised drugs reabsorbed back into blood; ionised drugs remain in urine and are excreted |
- Alkaline urine (e.g. bicarbonate) → ionises weak acids → traps them in urine → ↑ excretion of aspirin, phenobarbital
- Acidic urine → ionises weak bases → traps them → ↑ excretion of amphetamines
Other Routes of Elimination
- Bile/faeces: Drugs conjugated with glucuronic acid excreted in bile; may undergo enterohepatic circulation
- Lungs: Volatile anaesthetics, ethanol
- Breast milk, saliva, sweat, tears (minor routes)
Key Pharmacokinetic Parameters
Half-Life (t½)
t½ = 0.693 × Vd / Cl (where Cl = clearance)
- Determines dosing frequency: drugs with short t½ require more frequent dosing
- 5 half-lives to reach steady state (or complete washout)
- 3.3 half-lives to reach 90% of steady state
Steady State (C_ss)
- Reached after 5 × t½ of regular dosing regardless of dose or dosing interval
- A loading dose achieves therapeutic levels rapidly before steady state is reached
- Dosing interval affects fluctuation amplitude, NOT the steady-state concentration
Clearance (Cl)
PART 2: PHARMACODYNAMICS (PD)
Drug-Receptor Interactions
Types of Receptors
| Receptor Type | Location | Signalling | Examples |
|---|---|---|---|
| Ligand-gated ion channels | Cell membrane | Direct ion flow on binding | Nicotinic ACh receptor, GABA-A, glutamate receptors |
| G-protein coupled receptors (GPCRs) | Cell membrane | Activate G-proteins → second messengers (cAMP, IP3, Ca²⁺) | β-adrenergic, muscarinic, opioid, dopamine receptors |
| Enzyme-linked receptors | Cell membrane | Receptor has intrinsic kinase activity | Insulin receptor, growth factor receptors |
| Intracellular receptors | Cytoplasm/nucleus | Drug must be lipophilic to enter cell; activate gene transcription | Glucocorticoid, thyroid hormone, steroid receptors |
Agonists and Antagonists
| Term | Definition | Example |
|---|---|---|
| Agonist | Binds receptor AND activates it (produces response) | Morphine (opioid agonist), salbutamol (β₂ agonist) |
| Full agonist | Produces maximum possible response | Morphine |
| Partial agonist | Binds receptor but produces submaximal response; can block full agonists | Buprenorphine |
| Antagonist | Binds receptor but does NOT activate it; blocks agonist binding | Naloxone (opioid antagonist), atropine (muscarinic antagonist) |
| Competitive antagonist | Competes with agonist for same receptor; can be overcome by ↑ agonist dose | Atropine, metoprolol |
| Non-competitive antagonist | Binds irreversibly or allosteric site; cannot be overcome by ↑ agonist dose | Phenoxybenzamine |
| Inverse agonist | Binds receptor and produces opposite effect to agonist | Some antihistamines |
Dose-Response Relationships
| Parameter | Definition | Clinical relevance |
|---|---|---|
| Potency (ED50) | Dose producing 50% maximum effect | Compares relative drug strength; does NOT imply safety or efficacy |
| Efficacy (Emax) | Maximum effect achievable regardless of dose | Partial agonists have lower efficacy than full agonists |
| EC50 | Concentration producing 50% maximum effect | Lower EC50 = more potent |
Therapeutic Index (TI)
TI = TD50 / ED50 (or LD50 / ED50 in animal studies)
- Wide TI (safe drugs) = large margin between therapeutic and toxic doses - e.g. penicillins
- Narrow TI (dangerous drugs) = small margin; require therapeutic drug monitoring (TDM)
- Warfarin, digoxin, lithium, phenytoin, theophylline, aminoglycosides, cyclosporine, methotrexate, valproate
PART 3: DRUG NAMES AND NOMENCLATURE
| Name Type | Definition | Example |
|---|---|---|
| Chemical name | Precise chemical structure (IUPAC) | N-acetyl-para-aminophenol |
| Generic name (INN) | International Non-proprietary Name; standardised name | Paracetamol (UK) / Acetaminophen (USA) |
| Brand/Trade name | Manufacturer's proprietary name (capitalised) | Panadol®, Tylenol® |
Drug Stem Nomenclature (INN Suffixes)
Cardiovascular Drugs
| Stem | Drug Class | Examples |
|---|---|---|
| -olol | β-blockers (beta-adrenergic antagonists) | Propranolol, metoprolol, atenolol, carvedilol |
| -dipine | Calcium channel blockers (dihydropyridines) | Amlodipine, nifedipine, felodipine |
| -pril | ACE inhibitors | Enalapril, lisinopril, ramipril, captopril |
| -sartan | Angiotensin II receptor blockers (ARBs) | Losartan, valsartan, irbesartan, candesartan |
| -statin | HMG-CoA reductase inhibitors (statins) | Atorvastatin, rosuvastatin, simvastatin |
| -fibrate | Fibrates (lipid-lowering) | Fenofibrate, gemfibrozil |
| -tidine | H₂ receptor antagonists | Ranitidine, famotidine, cimetidine |
| -floxacin | Fluoroquinolone antibiotics | Ciprofloxacin, levofloxacin, moxifloxacin |
Antimicrobials
| Stem | Drug Class | Examples |
|---|---|---|
| -cillin | Penicillins | Amoxicillin, ampicillin, piperacillin, flucloxacillin |
| -cycline | Tetracyclines | Doxycycline, tetracycline, minocycline |
| -mycin / -micin | Aminoglycosides or macrolides | Gentamicin, tobramycin (amino); Erythromycin, azithromycin, clarithromycin (macrolide) |
| -azole | Antifungals (azoles) or antiprotozoals | Fluconazole, ketoconazole, metronidazole |
| -navir | HIV protease inhibitors | Ritonavir, lopinavir, atazanavir, darunavir |
| -vir | Antivirals | Aciclovir, oseltamivir, sofosbuvir, tenofovir |
| -ovir | Antivirals (herpes/HIV) | Aciclovir, ganciclovir, entecavir |
| -conazole | Antifungals | Fluconazole, itraconazole, voriconazole |
CNS / Neurology
| Stem | Drug Class | Examples |
|---|---|---|
| -pam / -lam | Benzodiazepines | Diazepam, lorazepam, midazolam, alprazolam |
| -pine | Tricyclic antidepressants or antipsychotics | Amitriptyline, clomipramine, clozapine, olanzapine |
| -triptan | Serotonin (5-HT1B/1D) agonists (migraine) | Sumatriptan, rizatriptan, zolmitriptan |
| -prazole | Proton pump inhibitors | Omeprazole, lansoprazole, pantoprazole, esomeprazole |
| -tidine | H₂ blockers | Ranitidine, famotidine |
| cef- / ceph- | Cephalosporins | Cefuroxime, ceftriaxone, cefalexin |
Endocrine / Metabolic
| Stem | Drug Class | Examples |
|---|---|---|
| -glitazone | PPAR-γ agonists (thiazolidinediones) | Pioglitazone, rosiglitazone |
| -formin | Biguanides | Metformin |
| -gliptin | DPP-4 inhibitors | Sitagliptin, saxagliptin, vildagliptin |
| -gliflozin | SGLT-2 inhibitors | Empagliflozin, dapagliflozin, canagliflozin |
| -glutide | GLP-1 receptor agonists | Semaglutide, liraglutide, exenatide |
| -glimide | Sulfonylureas | Glipizide, glibenclamide, gliclazide |
Biologics / Monoclonal Antibodies
[prefix] - [target] - [source] - mab
| Component | Meaning | Examples |
|---|---|---|
| -mab | Monoclonal antibody | Indicates entire class |
| -u- | Human origin | Adalimumab, ustekinumab |
| -xi- | Chimeric (part mouse, part human) | Infliximab, rituximab |
| -zu- | Humanised | Trastuzumab, bevacizumab |
| -o- | Mouse origin (mostly obsolete) | Muronomab |
- -tu- = tumour (antineoplastic) - e.g. pertuzumab
- -li- = immunomodulating - e.g. basiliximab
- -ci- = cardiovascular - e.g. abciximab
- -os- = bone - e.g. denosumab
| Drug | Target | Use |
|---|---|---|
| Adalimumab (Humira) | TNF-α | Rheumatoid arthritis, IBD, psoriasis |
| Infliximab (Remicade) | TNF-α | IBD, rheumatoid arthritis |
| Trastuzumab (Herceptin) | HER2 | HER2+ breast/gastric cancer |
| Rituximab (MabThera) | CD20 | B-cell lymphomas, RA |
| Bevacizumab (Avastin) | VEGF | Colorectal, lung, ovarian cancers |
| Pembrolizumab (Keytruda) | PD-1 | Multiple cancers (checkpoint inhibitor) |
| Nivolumab (Opdivo) | PD-1 | Multiple cancers |
| Omalizumab (Xolair) | IgE | Allergic asthma |
| Denosumab (Prolia) | RANK-L | Osteoporosis, bone metastases |
PART 4: IMPORTANT DRUG INTERACTIONS
Pharmacokinetic Interactions (PK)
| Mechanism | Effect | Example |
|---|---|---|
| CYP3A4 inhibition | ↑ drug levels → toxicity | Ketoconazole + simvastatin → rhabdomyolysis |
| CYP induction | ↓ drug levels → failure | Rifampicin + oral contraceptive pill → pregnancy |
| P-gp inhibition | ↑ drug absorption | Clarithromycin + digoxin → digoxin toxicity |
| Protein binding displacement | ↑ free drug | Aspirin + warfarin → bleeding |
| Renal competition | ↑ drug retention | Probenecid + penicillin → ↑ penicillin levels (used therapeutically) |
Pharmacodynamic Interactions (PD)
| Type | Example |
|---|---|
| Synergism | Two drugs with same effect given together (additive or supra-additive) - e.g. alcohol + benzodiazepines → CNS depression |
| Antagonism | One drug blocks effect of another - e.g. naloxone reverses morphine |
| Potentiation | One drug increases effect of another without having same action alone |
Summary: Key Pharmacology Concepts at a Glance
| Concept | Key Point |
|---|---|
| ADME | Absorption, Distribution, Metabolism, Elimination |
| Bioavailability | IV = 100%; oral reduced by first-pass |
| Vd | Small = stays in plasma; Large = distributes into tissues |
| t½ | 5 half-lives to steady state or washout |
| CYP3A4 | Metabolises 36% of all drugs; major interaction site |
| Prodrugs | Codeine, clopidogrel, enalapril - activated by metabolism |
| Narrow TI | Warfarin, digoxin, lithium, phenytoin - need therapeutic drug monitoring |
| Agonist | Activates receptor |
| Antagonist | Blocks receptor |
| Potency vs. efficacy | Potency = dose needed; Efficacy = maximum effect achievable |
| INN stems | -olol = β-blocker; -pril = ACEi; -sartan = ARB; -statin = statin; -mab = monoclonal antibody |
Diuretics
Diuretics — Complete Reference
Definition
Sites of Action Along the Nephron
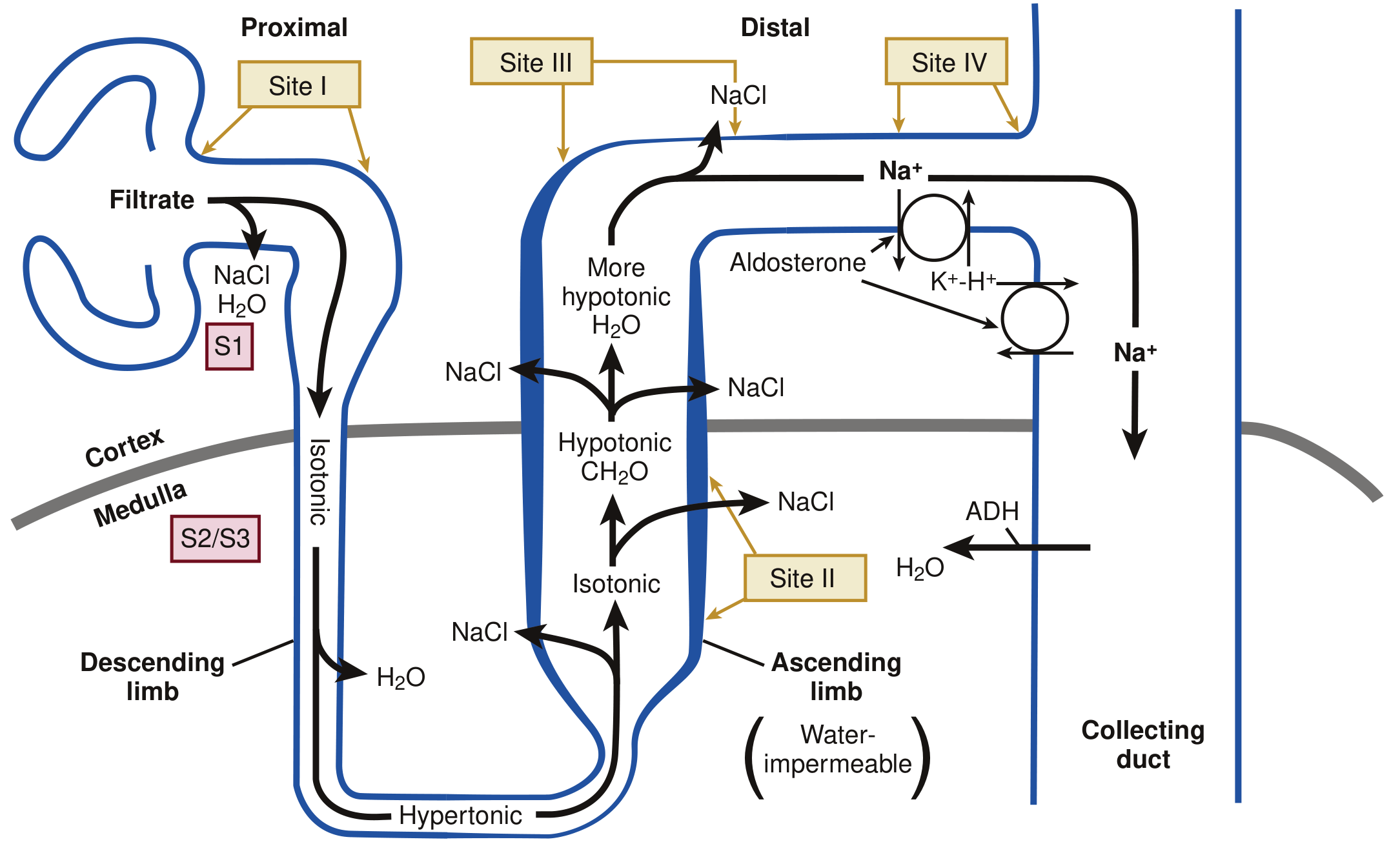
Overview Table
| Class | Site of Action | Transporter Blocked | Na⁺ Excretion | K⁺ Effect | Key Drug |
|---|---|---|---|---|---|
| Osmotic | Proximal tubule + descending loop | None (osmotic) | Moderate | Neutral | Mannitol |
| Carbonic anhydrase inhibitors | Proximal tubule (Site I) | H⁺/HCO₃⁻ (CA enzyme) | Weak | ↓K⁺ (lose K⁺) | Acetazolamide |
| Loop diuretics | Thick ascending limb (Site II) | NKCC2 (Na⁺-K⁺-2Cl⁻) | Strongest: 20-25% | ↓K⁺ (hypokalaemia) | Furosemide |
| Thiazides | Distal convoluted tubule (Site III) | NCC (Na⁺-Cl⁻) | Moderate: 5-10% | ↓K⁺ (hypokalaemia) | Hydrochlorothiazide |
| K⁺-sparing (MRAs) | Collecting duct (Site IV) | Mineralocorticoid receptor | Weak | ↑K⁺ (spare K⁺) | Spironolactone |
| K⁺-sparing (ENaC blockers) | Collecting duct (Site IV) | ENaC (Na⁺ channel) | Weak | ↑K⁺ (spare K⁺) | Amiloride, Triamterene |
| SGLT2 inhibitors | Proximal tubule S1/S2 (Site I) | SGLT2 (Na⁺-glucose) | Mild | Neutral | Empagliflozin |
1. LOOP DIURETICS
Mechanism
- Act on the thick ascending limb of the loop of Henle (TAL)
- Compete with Cl⁻ to bind and inhibit NKCC2 (Na⁺-K⁺-2Cl⁻ co-transporter) on the apical membrane
- Because furosemide, bumetanide, and torsemide are highly protein-bound, filtration is limited → they are actively secreted into the tubular lumen via OAT1/OAT2 (organic anion transporters) in the proximal tubule
- Loss of Na⁺, K⁺, Cl⁻, and water (up to 20-25% of filtered Na⁺ - most potent diuretics)
- Disruption of the countercurrent multiplier → reduced medullary interstitial osmolarity → impairs both concentrating AND diluting ability of kidney
- Increased solute delivery to collecting duct → acts as osmotic agent preventing water reabsorption
- Urine output can reach 25× normal acutely
- Hypercalciuria - Ca²⁺ reabsorption in TAL is passive, driven by the electrochemical gradient from NaCl transport; block NaCl → lose Ca²⁺ too
- Hypomagnesaemia - same mechanism as Ca²⁺ loss
Drugs and Doses
| Drug | Initial Dose | Max Daily Dose | Duration of Action | Notes |
|---|---|---|---|---|
| Furosemide | 20-40 mg OD/BD | 600 mg | 6-8 hours | Most commonly used; IV for acute pulmonary oedema |
| Bumetanide | 0.5-1 mg OD/BD | 10 mg | 4-6 hours | 40x more potent than furosemide mg-for-mg |
| Torsemide | 10-20 mg OD | 200 mg | 12-16 hours | Better oral bioavailability than furosemide (~80% vs ~50%) |
| Ethacrynic acid | 25-50 mg OD/BD | 200 mg | 6 hours | Only loop diuretic NOT sulfonamide-based; use in sulfa allergy |
Indications
- Acute pulmonary oedema (IV furosemide - 1st line)
- Chronic heart failure with fluid overload
- Hypertension (especially in CKD stages 4-5 where thiazides lose efficacy)
- Hypercalcaemia (loop diuretics promote Ca²⁺ excretion)
- Nephrotic syndrome, hepatic cirrhosis with ascites
- Forced diuresis in certain poisonings
Adverse Effects
| Side Effect | Mechanism |
|---|---|
| Hypokalaemia | ↑ Na⁺ delivery to collecting duct → ↑ K⁺ secretion; ↑ aldosterone |
| Hyponatraemia | Excessive free water loss |
| Hypomagnesaemia | Loss in urine (same paracellular mechanism as Ca²⁺) |
| Hypocalcaemia | Hypercalciuria → chronic depletion |
| Metabolic alkalosis | K⁺ loss → H⁺ shifts into cells; contraction alkalosis |
| Ototoxicity | Toxic to cochlear hair cells; dose-dependent; reversible (usually); worse with aminoglycosides |
| Hyperuricaemia | Compete with uric acid for OAT secretion → reduced urate excretion → gout |
| Hypovolaemia / prerenal AKI | Excessive diuresis |
| Hyperglycaemia | (mild, less than thiazides) |
| Sulfonamide allergy | Furosemide, bumetanide, torsemide contain sulfonamide group → use ethacrynic acid if severe sulfa allergy |
2. THIAZIDE DIURETICS
Mechanism
- Act on early distal convoluted tubule (DCT)
- Block NCC (Na⁺-Cl⁻ co-transporter) on the apical membrane
- Maximum fractional Na⁺ excretion = 5-10% (weaker than loop)
- Decrease free water clearance → can contribute to hyponatraemia
- Hypocalciuria (opposite to loop diuretics) - thiazides INCREASE Ca²⁺ reabsorption in DCT by a separate mechanism; useful for kidney stones and osteoporosis
Drugs
| Drug | Notes |
|---|---|
| Hydrochlorothiazide (HCTZ) | Most widely used thiazide |
| Chlorthalidone | Longer-acting; preferred in guidelines for hypertension; more potent CV benefit |
| Indapamide | Thiazide-like; also has direct vasodilatory effect |
| Metolazone | Thiazide-like; also acts on proximal tubule; used in combination with furosemide for diuretic resistance in heart failure; effective even in CKD |
| Bendroflumethiazide | Commonly used in UK for hypertension |
Indications
- Hypertension (1st line or combination; multiple RCTs show reduction in mortality and CV events)
- Heart failure (adjunct to loop diuretics)
- Nephrolithiasis / hypercalciuria (reduce urinary Ca²⁺)
- Osteoporosis (increase Ca²⁺ retention)
- Nephrogenic diabetes insipidus (paradoxical mechanism - volume contraction → ↑ proximal reabsorption → ↓ urine output)
- Oedema (mild to moderate)
Adverse Effects
| Side Effect | Mechanism / Notes |
|---|---|
| Hypokalaemia | ↑ Na⁺ delivery to collecting duct → K⁺ secretion; most common |
| Hyponatraemia | Impairs free water clearance; most dangerous electrolyte effect |
| Hyperglycaemia | ↓ Insulin secretion (K⁺ depletion reduces beta-cell function) |
| Dyslipidaemia | ↑ LDL, triglycerides (dose-dependent) |
| Hyperuricaemia / gout | Compete with uric acid excretion |
| Hypomagnesaemia | Direct Mg²⁺ wasting in DCT |
| Hypercalcaemia | ↑ Ca²⁺ reabsorption → raise serum Ca²⁺ |
| Metabolic alkalosis | K⁺ loss + contraction alkalosis |
| Photosensitivity | Sulfonamide derivative → rash |
| Sexual dysfunction | Less common with newer agents |
"GLUC" goes UP: Glucose, Lipids, Uric acid, Calcium "SNAP" goes DOWN: Sodium, Na (filtered), K (potassium), Mg (magnesium)
3. POTASSIUM-SPARING DIURETICS
Sub-class A: Mineralocorticoid Receptor Antagonists (MRAs)
Mechanism
- Block aldosterone (mineralocorticoid) receptors in the collecting duct principal cells
- Normally aldosterone promotes Na⁺ reabsorption and K⁺/H⁺ secretion
- MRAs block this → ↓ Na⁺ reabsorption + ↑ K⁺ retention
- Natriuresis is mild (only ~2-3% of filtered load) because most Na⁺ has already been reabsorbed upstream
Drugs
| Drug | Generation | Notes |
|---|---|---|
| Spironolactone | 1st (steroidal) | Structural analogue of aldosterone; anti-androgenic side effects |
| Eplerenone | 2nd (steroidal) | More selective; fewer sex hormone side effects than spironolactone |
| Finerenone | 3rd (non-steroidal) | Most selective; less hyperkalaemia; approved for CKD + T2DM |
Indications
- Heart failure (RALES trial: spironolactone 25 mg reduced mortality by 30% in severe HF; EMPHASIS trial: eplerenone in mild HF)
- Hypertension (especially resistant hypertension, 4th-line agent)
- Primary hyperaldosteronism (Conn syndrome) - both diagnostic and therapeutic
- Cirrhosis with ascites (1st-line diuretic due to secondary hyperaldosteronism)
- Combined with loop/thiazide diuretics to prevent hypokalaemia
- Finerenone: CKD with type 2 diabetes (renoprotective and cardioprotective)
Adverse Effects
- Hyperkalaemia (most dangerous; dose-dependent; worse in CKD; avoid with ACEi/ARBs/K⁺ supplements)
- Metabolic acidosis (↓ H⁺ secretion)
- Gynaecomastia (spironolactone only - anti-androgenic effect)
- Menstrual irregularities (spironolactone)
- Impotence / decreased libido (spironolactone)
- Eplerenone avoids most sexual side effects
Sub-class B: ENaC Blockers (Epithelial Na⁺ Channel Blockers)
Mechanism
- Amiloride and triamterene directly block ENaC (epithelial sodium channels) in the luminal membrane of collecting duct principal cells
- Independent of aldosterone → work even in low-aldosterone states
- Block Na⁺ entry → ↓ Na⁺-K⁺-ATPase activity → ↓ K⁺ secretion → potassium-sparing
Drugs and Uses
| Drug | Use | Notes |
|---|---|---|
| Amiloride | Combined with HCTZ (e.g. Co-amilozide); treatment-resistant hypertension | Pure K⁺-sparing effect |
| Triamterene | Combined with HCTZ (Dyazide®, Maxzide®) | Can crystallise in urine → nephrolithiasis |
Adverse Effects (both ENaC blockers)
- Hyperkalaemia (main concern)
- Metabolic acidosis
- Triamterene: renal calculi, folate antagonism
4. CARBONIC ANHYDRASE INHIBITORS
Mechanism
- Acetazolamide inhibits carbonic anhydrase (CA) enzyme, primarily in proximal tubule
- CA normally catalyses: CO₂ + H₂O ⇌ H₂CO₃ ⇌ H⁺ + HCO₃⁻
- Blocking CA → ↓ H⁺ secretion → ↓ Na⁺/H⁺ exchange → NaHCO₃ remains in tubule → osmotic diuresis
- Result: loss of Na⁺ + HCO₃⁻ in urine → metabolic acidosis (bicarbonate wasting)
- Weak diuretic - proximal tubule reabsorbs only bicarbonate-linked Na⁺; compensated by downstream segments
Drug: Acetazolamide
Indications
- Acute mountain sickness (AMS) prophylaxis and treatment - induces metabolic acidosis → respiratory stimulation → ↑ ventilation → ↑ O₂ saturation
- Glaucoma (reduces aqueous humour production by inhibiting CA in ciliary body)
- Idiopathic intracranial hypertension (pseudotumour cerebri)
- Metabolic alkalosis from contraction (short-term use)
- Epilepsy (some types, second-line)
- Altitude acclimatisation
Adverse Effects
- Metabolic (hyperchloraemic) acidosis - bicarbonate wasting; limits long-term use
- Hypokalaemia - ↑ distal Na⁺ delivery
- Drowsiness, paraesthesiae (tingling of face and extremities)
- Tinnitus
- Nephrolithiasis (alkaline urine → Ca²⁺ phosphate stones)
- Contraindicated in sulfa allergy (contains sulfonamide group)
5. OSMOTIC DIURETICS
Mechanism
- Mannitol (prototype) is a non-reabsorbable sugar alcohol
- Freely filtered at glomerulus but NOT reabsorbed
- Acts as an osmotic agent → retains water in the tubular lumen → obligatory water and solute excretion
- Also reduces medullary interstitial osmolarity
Drug: Mannitol
Indications
- Cerebral oedema / raised intracranial pressure (ICP) - draws water from brain parenchyma into the bloodstream (osmotic effect across BBB)
- Acute oliguric kidney injury - flushes tubules, prevents tubular obstruction
- Acute glaucoma - reduces vitreous humour volume
- Haemolytic transfusion reactions - promotes forced diuresis to prevent haemoglobinuria causing AKI
- Used in combination with furosemide in acute decompensated heart failure
Adverse Effects
- Initial intravascular volume expansion before diuresis → can precipitate pulmonary oedema in heart failure
- Hyponatraemia (dilutional) initially
- Hypernatraemia and dehydration after prolonged use
- Rebound intracranial hypertension (if BBB disrupted, mannitol enters brain tissue)
- Contraindicated in pulmonary oedema, severe heart failure, anuria (cannot be excreted)
6. SGLT2 INHIBITORS (New Class - Also Diuretic)
Mechanism
- Block SGLT2 (sodium-glucose co-transporter 2) in proximal tubule S1-S2 segments
- Accounts for 90% of renal glucose reabsorption
- Blocking SGLT2 → glucose + Na⁺ excreted in urine → glycosuria + mild natriuresis
- Volume contraction without sympathetic activation
- Triggers tubuloglomerular feedback → afferent arteriole constriction → reduces glomerular hyperfiltration → renoprotective
Drugs (the "-gliflozins")
| Drug | Key Trial | Key Indication |
|---|---|---|
| Empagliflozin (Jardiance) | EMPA-REG OUTCOME | T2DM, HFrEF, CKD |
| Dapagliflozin (Forxiga) | DAPA-HF, DECLARE-TIMI | T2DM, HFrEF, HFpEF, CKD |
| Canagliflozin (Invokana) | CANVAS, CREDENCE | T2DM, CKD |
Indications
- Type 2 diabetes mellitus (lower HbA1c)
- Heart failure (HFrEF and HFpEF - reduce hospitalisations and mortality)
- Chronic kidney disease (renoprotective regardless of diabetes status)
- Weight loss (caloric loss via glycosuria)
- Cardiovascular risk reduction (MACE reduction)
Adverse Effects
- Genital mycotic infections (glycosuria promotes Candida growth)
- UTIs (more glucose in urine)
- Euglycaemic DKA (rare but serious; glucose may be normal; acidosis from ketogenesis)
- Fournier's gangrene (rare)
- Hypotension / volume depletion
- Amputation risk (canagliflozin - higher risk; mechanism unclear)
- Bone fractures (canagliflozin)
Diuretic Resistance
| Cause | Solution |
|---|---|
| Reduced oral bioavailability | Switch to IV route |
| Hypoalbuminaemia → less drug delivered to tubule | Albumin infusion before furosemide |
| Reduced GFR → less drug secreted | Increase dose |
| RAAS activation by loop diuretic | Add MRA (spironolactone) |
| Distal tubule hypertrophy (adaptation) | Add thiazide (especially metolazone) |
| Poor Na⁺ restriction | Sodium restriction + dietary counselling |
| High albumin binding | Use bolus then continuous IV infusion |
Clinical Comparison Summary
| Feature | Loop | Thiazide | K⁺-sparing (MRA) | CA Inhibitor | Osmotic |
|---|---|---|---|---|---|
| Potency | Highest (20-25%) | Moderate (5-10%) | Weak (2-3%) | Weak | Moderate |
| K⁺ effect | ↓ (lose K⁺) | ↓ (lose K⁺) | ↑ (spare K⁺) | ↓ (lose K⁺) | Neutral |
| Ca²⁺ effect | ↑ excretion (hypercalciuria) | ↓ excretion (hypocalciuria) | Neutral | ↑ excretion | Neutral |
| Acid-base | Metabolic alkalosis | Metabolic alkalosis | Metabolic acidosis | Metabolic acidosis | Neutral |
| Works in CKD? | Yes | No (Clcr <40) | Use caution | Yes | Yes |
| Key interaction | Ototoxicity + aminoglycosides | ↑ digoxin toxicity (via hypokalaemia) | Hyperkalaemia + ACEi/K⁺ supplements | Sulfa allergy | Pulmonary oedema |
Drug Names Quick Reference
- Furosemide + Spironolactone (Lasix + Aldactone) - cirrhosis, HF
- Amiloride + HCTZ (Co-amilozide / Moduretic)
- Triamterene + HCTZ (Dyazide, Maxzide)
parathyroid gland and its disorders in detail trousseau sign calcium levels