Anti malarial drugs enumerate classify chloroquine and act moa uses adverse effect
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
2nd yr mbbs refer kdt
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
KD Tripathi is not in this library, but I have all the content needed from Lippincott, Katzung, and Goodman & Gilman — which together cover the same syllabus as KDT for 2nd year MBBS. Here is a complete, exam-oriented answer:
Antimalarial Drugs — 2nd Year MBBS (KDT-style)
I. Classification of Antimalarial Drugs
Based on Chemical Class
| Class | Drugs |
|---|---|
| 4-Aminoquinolines | Chloroquine, Amodiaquine, Hydroxychloroquine |
| 8-Aminoquinolines | Primaquine, Tafenoquine |
| Quinoline methanols | Quinine, Quinidine, Mefloquine |
| Bisquinolines | Piperaquine |
| Sesquiterpene lactone endoperoxides | Artemisinin, Artesunate, Artemether, Dihydroartemisinin (ACTs) |
| Folate antagonists | Pyrimethamine, Proguanil, Sulfadoxine-pyrimethamine (Fansidar) |
| Quinone + folate antagonist combo | Atovaquone-proguanil (Malarone) |
| Tetracyclines | Doxycycline, Tetracycline |
| Amyl alcohols | Lumefantrine (used in combo with artemether = Coartem) |
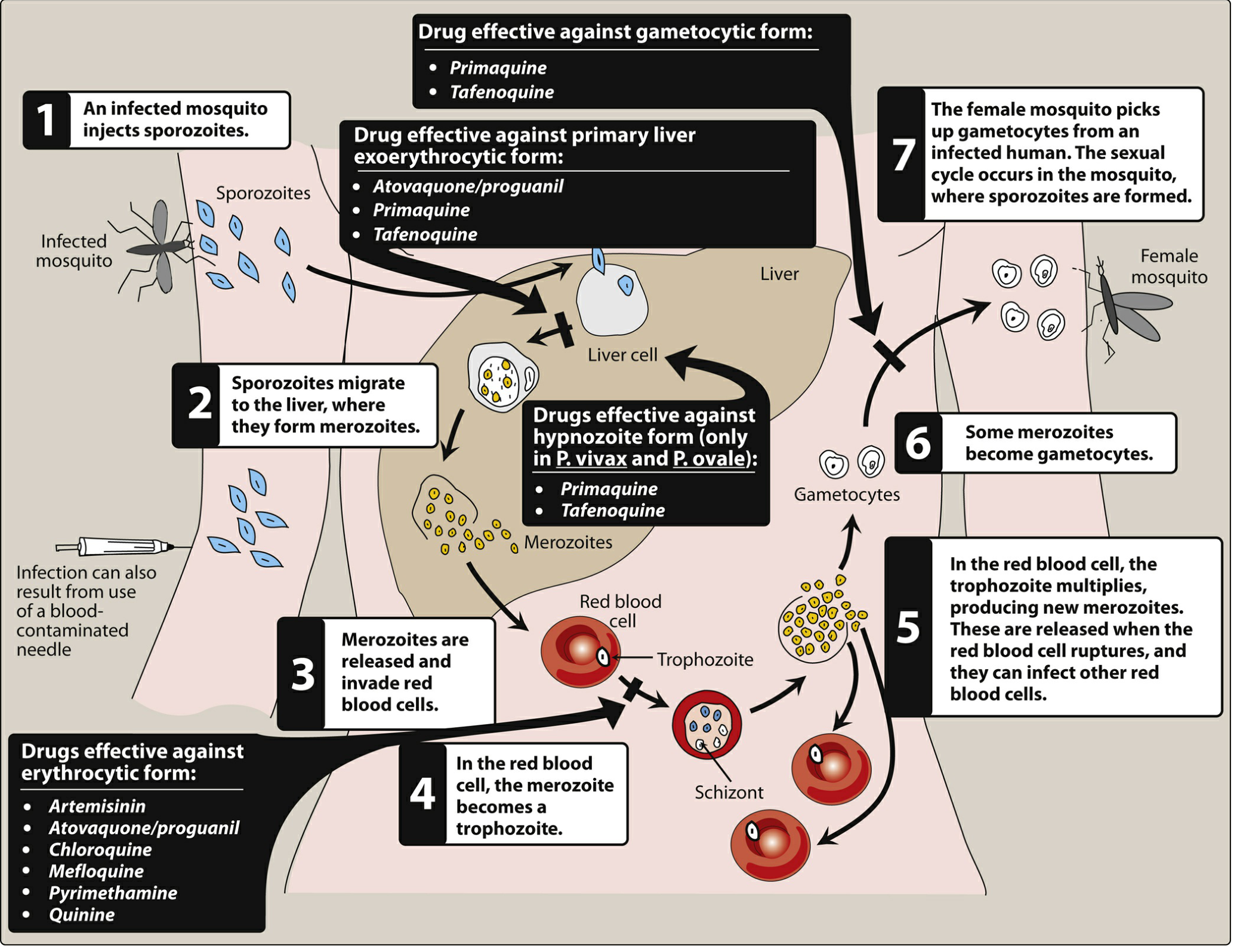
Based on Stage of Action
| Stage | Drugs |
|---|---|
| Primary exoerythrocytic (liver schizonticides) | Primaquine, Tafenoquine, Atovaquone-proguanil |
| Hypnozoiticides (P. vivax / P. ovale relapse prevention) | Primaquine, Tafenoquine |
| Blood schizonticides (erythrocytic stage) | Chloroquine, Quinine, Mefloquine, Artemisinin, Pyrimethamine, Doxycycline |
| Gametocytocidal | Primaquine (all species), Artemisinin (P. falciparum gametocytes) |
| Sporontocidal (blocks development in mosquito) | Primaquine, Proguanil |
II. Chloroquine
Drug Profile
- Class: 4-Aminoquinoline; synthetic drug
- Active against: Erythrocytic asexual stages + some gametocytes (P. vivax, P. malariae, P. ovale); NOT against liver stages or hypnozoites
Mechanism of Action
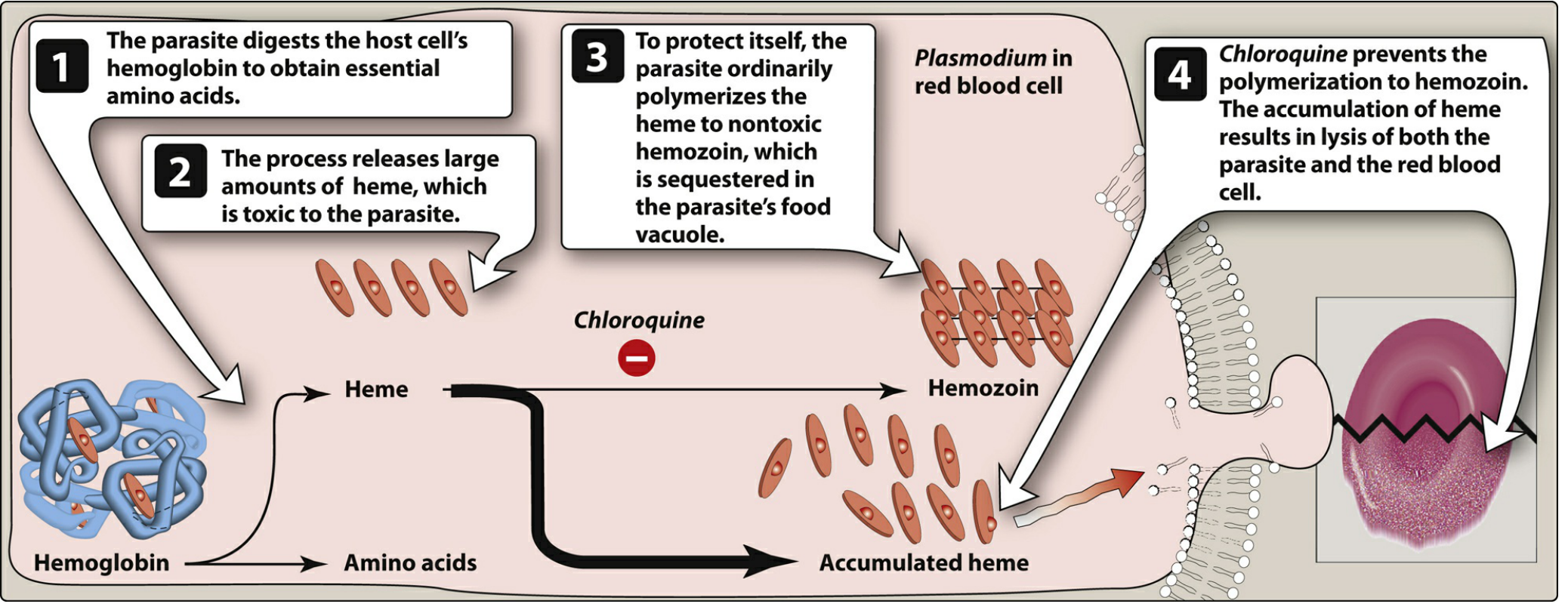
- Chloroquine is a diprotic weak base — it crosses erythrocytic and plasmodial membranes and concentrates in the acidic food vacuole of the parasite (ion trapping)
- The parasite digests host cell hemoglobin to obtain amino acids, releasing large amounts of free heme — which is toxic to the parasite
- Normally the parasite polymerizes heme into non-toxic hemozoin (malaria pigment) and sequesters it
- Chloroquine binds to free heme and inhibits its polymerization to hemozoin
- → Accumulation of toxic heme causes oxidative damage to phospholipid membranes → lysis of both parasite and RBC
In short: Inhibits heme polymerization → toxic heme accumulation → parasite death
- Also raises intra-vacuolar pH (alkalinization), further disrupting parasite digestion of Hb
- Resistance: P. falciparum develops a PfCRT (chloroquine resistance transporter) mutation → pumps chloroquine out of the food vacuole
Uses of Chloroquine
| Indication | Detail |
|---|---|
| Treatment of malaria | Drug of choice for chloroquine-sensitive P. vivax, P. malariae, P. ovale; limited use for P. falciparum (widespread resistance) |
| Chemoprophylaxis | For travel to areas with chloroquine-sensitive malaria (Central America west of Panama Canal, Hispaniola, parts of Middle East) |
| Extraintestinal amebiasis | Amebic liver abscess (used with metronidazole) |
| Rheumatoid arthritis / SLE | Immunomodulatory — suppresses T-lymphocyte responses, inhibits leukocyte chemotaxis (used as disease-modifying agent) |
| Discoid lupus / Porphyria cutanea tarda | (Hydroxychloroquine preferred) |
Adverse Effects of Chloroquine
| System | Effect |
|---|---|
| GI | Nausea, vomiting, abdominal discomfort (minimized by taking after meals) |
| CNS | Headache, dizziness, blurred vision |
| Skin | Pruritus (very common in Africans — a major compliance issue); skin rash; discoloration of nail beds and mucous membranes on chronic use |
| Eyes | Retinopathy — irreversible retinal damage on prolonged/high-dose use; corneal deposits; routine ophthalmologic exam required during long-term therapy |
| CVS | QT prolongation — risk of arrhythmia; avoid co-administration with other QT-prolonging drugs |
| Haematological | Haemolysis in G6PD-deficient patients (less than primaquine) |
Contraindications:
- Psoriasis (may precipitate acute attack)
- Porphyria (may precipitate acute attack)
- Severe hepatic/neurological disease — use cautiously
- Pregnancy: crosses placenta — generally avoided at high doses; low-dose prophylaxis considered acceptable
III. Artemisinin-Based Combination Therapy (ACT)
Background
Derived from sweet wormwood (Artemisia annua) — used in Chinese medicine for centuries. Nobel Prize 2015 awarded to Tu Youyou for its discovery.
Key derivatives in clinical use:
| Drug | Route |
|---|---|
| Artesunate | IV/IM/oral/rectal |
| Artemether | Oral/IM |
| Dihydroartemisinin (DHA) | Oral |
Mechanism of Action of Artemisinin
- Artemisinins contain a unique sesquiterpene lactone endoperoxide bridge
- Inside the parasite's food vacuole, free heme (from Hb digestion) activates artemisinin by cleaving this endoperoxide bridge
- This generates reactive free radicals (carbon-centered and oxygen-centered)
- Free radicals promiscuously alkylate and oxidize multiple parasite proteins — including transport proteins, enzymes, and structural proteins
- → Rapid parasite death (4-log₁₀ reduction in parasite burden per 48-hour erythrocytic cycle)
- Also reduces gametocyte carriage — reduces onward transmission
In short: Heme-activated endoperoxide → free radicals → alkylation of parasite proteins → rapid parasite death
Why Combination Therapy (ACT)?
- Artemisinins alone require >7 days of therapy to fully clear parasites (rapid but short half-life)
- Paired with a slower-acting, slower-eliminated partner drug with a different mechanism:
- Rapid artemisinin component kills most parasites quickly
- Partner drug clears the residual parasites and prevents recrudescence
- 3-day ACT courses are effective vs. 7+ day monotherapy
Major ACT Combinations (WHO Recommended)
| ACT | Constituent Drugs | Use |
|---|---|---|
| Coartem | Artemether + Lumefantrine | First-line uncomplicated P. falciparum |
| Artesunate-Amodiaquine | Artesunate + Amodiaquine | First-line (Africa) |
| Artesunate-Mefloquine | Artesunate + Mefloquine | Southeast Asia |
| DHA-Piperaquine | Dihydroartemisinin + Piperaquine | Asia |
| Pyramax | Artesunate + Pyronaridine | Alternative |
| IV Artesunate | Artesunate alone | Severe/complicated P. falciparum (replaces quinine IV) |
Uses of ACT
| Indication |
|---|
| First-line treatment for uncomplicated P. falciparum malaria in all endemic areas (WHO guideline) |
| Chloroquine-resistant falciparum malaria |
| Severe/complicated falciparum malaria (IV artesunate — superior to IV quinine) |
| Effective against asexual erythrocytic stages of P. vivax too |
Adverse Effects of Artemisinins
| Effect | Detail |
|---|---|
| Generally well tolerated | One of the safest antimalarials |
| Nausea, vomiting, dizziness | Mild, transient |
| Neurotoxicity | In high doses in animal studies; clinical significance at therapeutic doses unclear |
| QT prolongation | Mild; less than quinine |
| Embryotoxic | Teratogenic in animal studies — avoid in 1st trimester; use only if benefit outweighs risk |
| Haemolysis (delayed) | Seen with IV artesunate in hyperparasitaemia — delayed haemolytic anaemia 2–4 weeks post-treatment |
| Resistance (partial) | Pfk13 gene mutation → delayed parasite clearance; clinically significant ACT failure reported in Southeast Asia when partner drug resistance co-exists |
Quick Exam Summary Table
| Feature | Chloroquine | ACT (Artemisinin) |
|---|---|---|
| Class | 4-Aminoquinoline | Sesquiterpene lactone endoperoxide |
| MOA | Inhibits heme polymerization → heme accumulation → lysis | Heme-activated free radicals → alkylation of parasite proteins |
| Stage | Blood schizonticidal, weak gametocytocidal | Blood schizonticidal + gametocytocidal |
| No effect on | Liver stages, hypnozoites | Liver stages, hypnozoites |
| Key use | Sensitive P. vivax/P. malariae/P. ovale; amebic liver abscess; RA/SLE | 1st-line P. falciparum; severe malaria (IV artesunate) |
| Key ADR | Retinopathy, pruritus, QT prolongation | Embryotoxicity (1st trimester), delayed haemolysis (artesunate IV) |
| Resistance | PfCRT mutation (P. falciparum — widespread) | Pfk13 mutation (delayed clearance, SE Asia) |
Sources: Lippincott Illustrated Reviews Pharmacology; Katzung's Basic and Clinical Pharmacology, 16th Ed; Goodman & Gilman's Pharmacological Basis of Therapeutics — content equivalent to KD Tripathi's Essentials of Medical Pharmacology for 2nd MBBS syllabus.
Sedative n hypnotics drugs classify benzodiazepines over barbiturates, adv of benzodiazepines moa therapeutic uses
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent — I have all the content needed. Here is the complete 2nd year MBBS answer:
Sedative-Hypnotic Drugs — 2nd Year MBBS (KDT-style)
I. Definition
- Sedative: A drug that reduces anxiety and produces calming without inducing sleep at therapeutic doses
- Hypnotic: A drug that produces drowsiness and facilitates the onset and maintenance of sleep
- The same drug can act as a sedative at low dose and a hypnotic at higher dose — hence the group is called sedative-hypnotics
II. Classification of Sedative-Hypnotic Drugs
A. Benzodiazepines (BZDs)
Long-acting (t½ >24 h):
- Diazepam, Chlordiazepoxide, Flurazepam, Clonazepam, Clorazepate
Intermediate-acting (t½ 6–24 h):
- Lorazepam, Alprazolam, Oxazepam, Temazepam, Nitrazepam
Short-acting (t½ <6 h):
- Triazolam, Midazolam
B. Barbiturates
Ultra-short-acting: Thiopental (IV anesthesia)
Short-acting: Pentobarbital, Secobarbital
Intermediate-acting: Amobarbital, Butabarbital
Long-acting: Phenobarbital (also anticonvulsant)
C. Non-Benzodiazepine Hypnotics ("Z-drugs") — GABA-A agonists
- Zolpidem, Zaleplon, Eszopiclone (selective α1-subunit agonists)
D. Melatonin Receptor Agonists
- Ramelteon (MT1/MT2 agonist — for insomnia)
E. Orexin Receptor Antagonists
- Suvorexant, Lemborexant
F. Older/Miscellaneous
- Chloral hydrate, Paraldehyde, Meprobamate (largely obsolete)
G. Antihistamines with sedative property
- Promethazine, Diphenhydramine
III. Mechanism of Action of Benzodiazepines
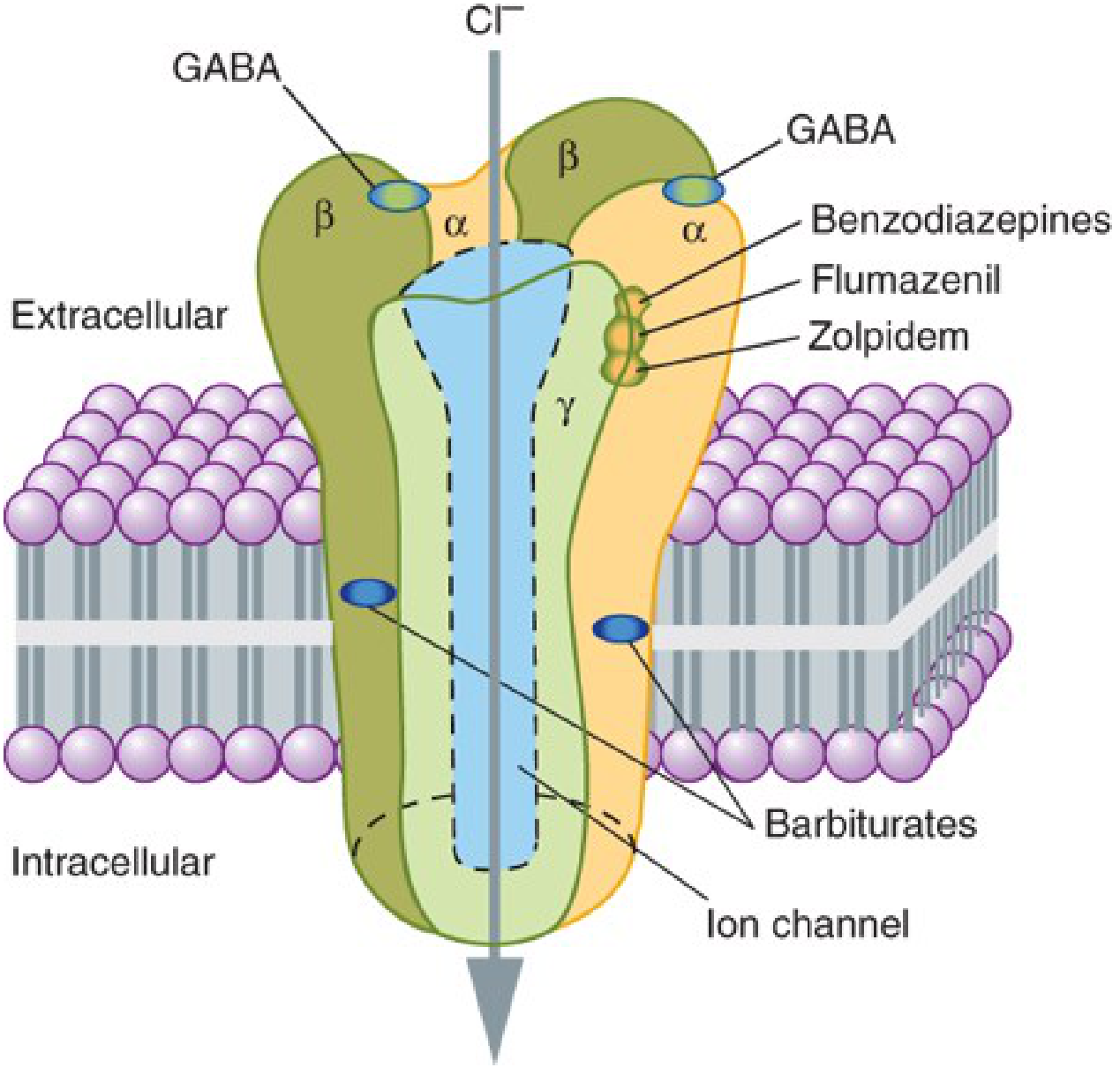
The GABA-A Receptor Complex
The GABA-A receptor is a pentameric ligand-gated chloride ion channel made up of subunits (2α, 2β, 1γ most common). It has distinct binding sites:
- GABA binds at the α–β subunit interface
- Benzodiazepines bind at the α–γ subunit interface (a separate, distinct site)
- Barbiturates bind at yet another distinct site (within the channel pore region)
How BZDs Work — Step by Step
- BZDs bind to the benzodiazepine binding site (BZ site) on the GABA-A receptor — allosteric site, separate from GABA binding site
- This binding does NOT directly open the Cl⁻ channel — BZDs require GABA to be present
- BZDs increase the affinity of the GABA receptor for GABA (allosteric potentiation)
- This results in an increase in the FREQUENCY of Cl⁻ channel opening (without changing the duration or conductance)
- ↑ Cl⁻ influx → hyperpolarization of the postsynaptic neuron → reduced neuronal excitability → CNS depression
Key point: BZDs are positive allosteric modulators of GABA-A. They cannot open Cl⁻ channels in the absence of GABA — this is why they have a ceiling effect and high safety.
BZDs vs Barbiturates at GABA-A Receptor
| Feature | Benzodiazepines | Barbiturates |
|---|---|---|
| Binding site | α–γ interface (BZ site) | Separate site (β subunit region / channel pore) |
| Effect on Cl⁻ channel | ↑ Frequency of opening | ↑ Duration of opening |
| GABA dependence | Yes — require GABA to act | At high doses — can directly open Cl⁻ channel (GABA-mimetic) |
| Ceiling effect | Yes (safe) | No (lethal at high dose) |
| Additional actions | GABA potentiation only | Also inhibit AMPA/glutamate receptors, Na⁺/K⁺ channels |
IV. Advantages of Benzodiazepines Over Barbiturates
This is a high-yield exam topic. BZDs replaced barbiturates as the drugs of choice largely because of the following advantages:
1. Wide Therapeutic Index / High Safety Margin
- BZDs cannot directly activate Cl⁻ channels — require endogenous GABA → ceiling effect on CNS depression
- Fatal overdose with BZDs alone is extremely rare
- Barbiturates have a narrow therapeutic index — overdose easily causes respiratory depression and death
2. Specific Antidote Available
- Flumazenil (a competitive BZ antagonist at the BZ site) reverses BZD effects
- No antidote available for barbiturate overdose
3. Less Respiratory Depression
- BZDs cause significantly less respiratory depression at therapeutic doses compared to barbiturates
4. Less Cardiovascular Depression
- BZDs have minimal cardiovascular effects at therapeutic doses
5. No Enzyme Induction
- Barbiturates are potent inducers of hepatic CYP450 enzymes → reduce efficacy of many co-administered drugs (warfarin, OCP, phenytoin, corticosteroids, etc.)
- BZDs do not induce hepatic enzymes → far fewer drug interactions
6. Less Physical Dependence and Tolerance
- Though BZDs do cause dependence, it is significantly less severe and develops more slowly than with barbiturates
- Barbiturates have high abuse and addiction potential with rapid tolerance development
7. No Suppression of REM Sleep (or minimal)
- Barbiturates markedly suppress REM sleep → REM rebound insomnia on discontinuation
- BZDs (especially short-acting) have lesser REM suppression
8. Less Rebound Insomnia
- Abrupt withdrawal from barbiturates causes severe rebound insomnia and potentially life-threatening withdrawal seizures
- BZD withdrawal, while significant, is generally less severe
9. No Cross-Reactions with Excitatory Neurotransmitters
- Barbiturates also inhibit glutamate (AMPA) receptors and affect Na⁺/K⁺ channels — producing non-specific CNS depression
- BZDs act selectively on GABA-A → more predictable, targeted effect
10. No Porphyria Precipitation
- Barbiturates precipitate acute porphyria attacks (enzyme induction)
- BZDs are safe in porphyria
V. Therapeutic Uses of Benzodiazepines
1. Anxiety Disorders (Anxiolytic)
- Short-term management of Generalized Anxiety Disorder (GAD), panic attacks, phobias, acute situational anxiety
- Drugs: Diazepam, Lorazepam, Alprazolam, Clonazepam
- Note: SSRIs/SNRIs are preferred for long-term anxiety; BZDs used for acute/bridging therapy
2. Insomnia (Hypnotic)
- Reduce sleep latency, decrease nocturnal awakenings
- Drugs: Nitrazepam, Flurazepam (long-acting); Temazepam, Lorazepam (intermediate); Triazolam (short-acting)
- Used for short-term insomnia only (tolerance develops within 2–4 weeks)
3. Epilepsy / Seizures (Anticonvulsant)
- Status epilepticus: IV Lorazepam (first choice) or IV Diazepam (first-line emergency treatment)
- Absence seizures / Myoclonic seizures: Clonazepam
- Febrile seizures: IV/rectal Diazepam
- Alcohol withdrawal seizures: Diazepam, Lorazepam, Chlordiazepoxide
4. Alcohol Withdrawal Syndrome
- Chlordiazepoxide and Diazepam — prevent delirium tremens, withdrawal seizures, and manage autonomic symptoms
- Long-acting BZDs preferred (self-tapering due to long t½)
5. Preoperative Medication (Premedication)
- Midazolam IV/IM — short-acting, produces sedation, anxiolysis, and anterograde amnesia
- Diazepam orally before procedures
6. IV Conscious Sedation / Procedural Sedation
- Midazolam — for endoscopy, minor surgical procedures, ICU sedation
7. Muscle Relaxant (Central)
- Diazepam — useful in muscle spasm, spasticity (multiple sclerosis, cerebral palsy), tetanus
- Mechanism: Enhancement of GABA inhibition at spinal cord level (interneurons) and supraspinal centers
8. Induction of Anesthesia
- Midazolam (IV) — produces rapid unconsciousness with amnesia; used for induction in balanced anesthesia
9. Bipolar Disorder / Acute Mania (Adjunct)
- Lorazepam, Clonazepam — used as adjunctive agents for acute agitation in manic episodes
10. Panic Disorder
- Alprazolam, Clonazepam — high potency BZDs; effective for acute panic attacks
VI. Quick Comparison Table — Classification by Duration
| Duration | Drug | t½ | Key Use |
|---|---|---|---|
| Ultra-short | Midazolam | 2–4 h | IV sedation, anesthesia induction |
| Short | Triazolam, Alprazolam | 2–6 h | Insomnia, panic |
| Intermediate | Lorazepam, Oxazepam, Temazepam | 6–24 h | Anxiety, status epilepticus |
| Long | Diazepam, Chlordiazepoxide, Clonazepam, Flurazepam | >24 h | Anxiety, seizures, alcohol withdrawal, muscle spasm |
Lorazepam, Oxazepam, Temazepam undergo direct glucuronide conjugation (no active metabolites) — safe in elderly, liver disease (mnemonic: LOT)
VII. Adverse Effects of Benzodiazepines
| Effect | Detail |
|---|---|
| Sedation/Drowsiness | Daytime sedation, cognitive impairment, "hangover" |
| Anterograde amnesia | Especially midazolam — inability to form new memories |
| Ataxia / Motor incoordination | Risk of falls in elderly |
| Dependence & Withdrawal | Physical and psychological dependence; abrupt cessation → rebound anxiety, insomnia, seizures |
| Respiratory depression | Mild at therapeutic doses; serious with IV use or in combination with opioids/alcohol |
| Paradoxical reactions | Agitation, aggression (more common in elderly, children) |
| Tolerance | Hypnotic effect lost within 2–4 weeks |
Contraindicated in: Myasthenia gravis, severe hepatic disease (except LOT drugs), sleep apnea, first trimester pregnancy (cleft palate risk), glaucoma (some agents)
Sources: Katzung Basic & Clinical Pharmacology 16th Ed; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Kaplan & Sadock's Synopsis of Psychiatry — aligned with KD Tripathi 2nd MBBS syllabus
This is a shared conversation. Sign in to Orris to start your own chat.