Explain in detail pacemakers and pacing and different pacemaker rhythms from Braunwald and other standard cardiology reference books and latest guidelines
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cardiac pacing" AND "pacemaker" AND "guidelines"
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I have extensive material from Braunwald's Heart Disease and Fuster/Hurst's The Heart. Now let me synthesize a comprehensive, detailed answer.
Pacemakers and Cardiac Pacing: A Comprehensive Reference
Sources: Braunwald's Heart Disease (11th Ed), Fuster and Hurst's The Heart (15th Ed), AHA/ACC Guidelines
1. Basic Principles of Cardiac Pacing
A permanent pacemaker system consists of two components:
- Pulse generator - contains the battery, sensing amplifiers, and output circuits
- Leads - deliver the electrical impulse to the myocardium and transmit sensed signals back
Lead Design (Braunwald, Ch. 69)
Fixation types:
- Passive fixation - tined leads that lodge in trabecular myocardium (most common for RV)
- Active fixation - retractable/extendable helical screw, allows placement at any site; tip electrode covered with mannitol that dissolves in bloodstream
Electrode configuration:
- Bipolar leads - both electrodes on the lead (tip cathode, ring anode ~1-2 cm proximal); less susceptible to oversensing from myopotentials or EMI
- Unipolar leads - only distal electrode on lead; pulse generator housing serves as anode; larger "antenna" makes them more susceptible to interference; larger pacing spike on ECG
Lead insulation: Polyurethane or silicone; coaxial design (inner and outer coil) or coradial design (coils individually insulated side by side)
2. The NASPE/BPEG Generic (NBG) Pacemaker Code
The current naming convention for pacemaker modes was established by the 2001 NASPE/BPEG consensus:
| Position | I | II | III | IV | V |
|---|---|---|---|---|---|
| Parameter | Chamber(s) Paced | Chamber(s) Sensed | Response to Sensing | Rate Modulation | Multisite Pacing |
| Codes | O, A, V, D | O, A, V, D | O, T, I, D | O, R | O, A, V, D |
- O = None; A = Atrium; V = Ventricle; D = Dual (both)
- Response: T = Triggered; I = Inhibited; D = Dual (triggered + inhibited)
- R (Position IV) = Rate modulation present
3. Common Pacing Modes (Braunwald, Ch. 69)
Single-Chamber Modes
VOO (Fixed-Rate Ventricular Asynchronous)
- Paces only the ventricle, senses nothing, fires asynchronously
- One timing clock: the ventricular escape interval (e.g., 1000 ms = 60 bpm)
- Delivers a pacing pulse regardless of intrinsic rhythm - can cause R-on-T and VF
- Clinical use: Applying a magnet over most pacemakers converts VVI → VOO, useful in the OR to prevent inappropriate inhibition from EMI
VVI (Ventricular Demand/Inhibited)
- Paces V, senses V, inhibited by sensed events
- The sensed ventricular event resets the escape interval
- Adds a ventricular refractory period (VRP) - sensed events during this are ignored (prevents T-wave oversensing, double-counting)
- Main drawback: No AV synchrony - predisposes to pacemaker syndrome
AAI (Atrial Inhibited)
- Paces A, senses A, inhibited by sensed events
- Maintains AV synchrony via native conduction
- Use: Sick sinus syndrome with intact AV conduction (AAIR is the rate-responsive form)
- Cannot be used if significant AV conduction disease is present
AOO / VOO - Asynchronous modes (no sensing); primarily triggered by magnet placement
Dual-Chamber Modes
DDD (Dual Sensing/Pacing/Inhibited+Triggered)
The most physiologic and commonly used mode. Key timing cycles:
- Lower Rate Limit (LRL) - minimum pacing rate
- Upper Rate Limit (URL) - maximum tracking rate in DDD
- AV interval - analogous to PR interval; typically programmed ~150-180 ms at rest (hemodynamically optimal ~150 ms)
- Post-Ventricular Atrial Refractory Period (PVARP) - after each V event, atrial channel is refractory to prevent sensing retrograde P-waves
- Total Atrial Refractory Period (TARP) = AV interval + PVARP
Four possible states in DDD:
- P-sensed, V-paced (AS-VP): Sensed native P wave triggers AV interval, then V paced
- P-paced, V-paced (AP-VP): Both chambers paced; rate below LRL
- P-sensed, V-sensed (AS-VS): Intrinsic rhythm above LRL, both sensed, no pacing
- P-paced, V-sensed (AP-VS): Atrium paced, native AV conduction occurs
DDI
- Paces D, senses D, but does not track atrial activity - avoids pacemaker-mediated tachycardia
- Atrial sensing only inhibits atrial output; does not trigger ventricular output
- Useful when intermittent atrial tachyarrhythmias risk rapid ventricular pacing
VDD
- Senses both A and V, paces only V
- Atrial sensing triggers ventricular pacing (tracks P-waves)
- Adequate for AV block with intact sinus function
- Limitation: If sinus rate drops below LRL, the device paces the ventricle only (losing AV synchrony)
- Uses a single lead with floating atrial sensing electrodes
DDD Mode Timing Cycles (Braunwald):
- At rates below LRL: atria paced → V paced after AV interval
- At rates between LRL and URL: sensed P → V paced after AV interval (P-tracking)
- At rates above URL: 2:1 block or Wenckebach upper rate behavior
- Upper Rate Behavior: At atrial rates exceeding URL, the TARP causes 2:1 block. Just below that, Wenckebach-like upper rate behavior occurs as the device delays VP to maintain TARP.
Mode Enhancements
ADI/R (Atrial-based pacing with minimal RV pacing)
Designed to reduce right ventricular pacing burden. The device operates like AAI/R but switches to DDD if a dropped beat is detected - "ADI/R with DDD backup."
Managed ventricular pacing (MVP) / Search AV+:
Algorithms that extend the AV interval or switch to AAI(R) to allow intrinsic AV conduction, minimizing unnecessary RV pacing. The MOST trial showed increased AF and heart failure with higher RV pacing frequency in SSS patients.
4. Rate-Responsive Pacing (Braunwald, Ch. 69)
The addition of R to the mode code (e.g., VVIR, DDDR, AAIR) indicates rate-adaptive pacing. This is critical because the most important mechanism for increasing cardiac output with exercise is heart rate augmentation - stroke volume can only rise modestly.
Sensors Used:
| Sensor | Mechanism | Strengths | Limitations |
|---|---|---|---|
| Accelerometer | Detects body motion/vibration | Simplest, widely used | May increase rate in car passengers; misses isometric exercise |
| Minute ventilation | Chest impedance measures respiratory effort | Good correlation with metabolic demand | May oversense with upper limb movement |
| RV lead impedance | Correlates with contractility | Physiologic | Less validated |
| QT interval | Shortens with catecholamines/exercise | Proportional to rate need | Affected by drugs |
| Central venous temperature, pH, dP/dt | Metabolic demand | Theoretical advantage | Limited clinical use |
Most widely used: Accelerometers, with minute ventilation as second most common (Braunwald).
In rate-responsive modes, the device paces at LRL at rest and increases up to the programmed upper rate limit based on sensor output.
5. His Bundle and Left Bundle Branch Area Pacing (Conduction System Pacing)
This represents the most important evolution in pacing technology in the past decade. Both Braunwald and Fuster/Hurst dedicate significant coverage to this.
His Bundle Pacing (HBP) (Braunwald, Ch. 69; Fuster, Ch. 38)
- First reported in a small cohort in 2000; field expanded rapidly after 2014
- Selective HBP: Only His bundle captured - narrow QRS, 35 ms isoelectric interval between pacing spike and QRS (= HV interval)
- Non-selective HBP: His bundle + local ventricular myocardium captured - slight delta-like morphology
- Advantages: Maintains synchronous ventricular activation via native Purkinje system; corrects LBBB morphology in ~70% of patients; no ventricular dyssynchrony
- Limitations: Higher/unstable thresholds; technically challenging; potential for far-field sensing
Left Bundle Branch Area Pacing (LBBAP) (Braunwald, Ch. 69; Fuster, Ch. 38)
- Lead screwed deep into the interventricular septum to capture the left bundle branch or its fascicles
- Selective LBBAP: Only LBB captured - produces narrow QRS
- Non-selective LBBAP: LBB + local septal myocardium - RBBB morphology with LBB capture characteristics
- ECG hallmark: R-wave in V1 plus narrow QRS, or short latency and characteristic V1 morphology
- Advantages over HBP: Lower and more stable thresholds; easier implant; can "rescue" failed HBP
- The 2026 meta-analysis (PMID 41957548) confirms LBBAP superior to RV pacing in conduction disorders
Biventricular Pacing (Cardiac Resynchronization Therapy - CRT)
- Simultaneous or near-simultaneous pacing of RV + LV via coronary sinus branch lead
- Corrects interventricular and intraventricular dyssynchrony caused by LBBB
- Indication (Class I): LVEF ≤35%, LBBB morphology, QRS ≥150 ms, NYHA II-IV on GDMT
- Upgrade from RV pacing to CRT is now preferred over continued RV pacing in those who develop pacing-induced cardiomyopathy (meta-analysis PMID 36352513)
- Biventricular vs. Conduction System Pacing: CSP (HBP/LBBAP) is increasingly considered equivalent or superior to biventricular pacing; meta-analysis (PMID 40644356) shows CSP ≥ BiV pacing after AV node ablation
6. Hemodynamic Aspects of Pacing (Braunwald, Ch. 69)
- Severe bradycardia with junctional/ventricular escape: ventricular pacing at normal rates increases cardiac output by 25-30%
- Restoring AV synchrony augments cardiac output by an additional 20%
- Chronotropic response (rate responsiveness) is dominant over AV synchrony in improving exercise capacity
- Optimal AV interval: ~150 ms at rest, somewhat less with exertion
Pacemaker Syndrome
- Occurs in 3-30% of patients with ongoing sinus activity subjected to VVI pacing
- Mechanism: atrial contractions against closed AV valves → retrograde VA conduction → cannon A waves → fall in BP, rise in pulmonary venous pressure
- Manifestations: fatigue, dyspnea, dizziness, neck pulsations (cannon waves), chest pain, hypotension, syncope
- Treatment: upgrade to dual-chamber pacing; dual-chamber pacing reduces stroke, AF occurrence, and improves quality of life vs. VVI
Right Ventricular Pacing-Induced Cardiomyopathy (Fuster, Ch. 38)
- Approximately 12-22% of patients with significant RV pacing develop cardiomyopathy
- Mechanism: RV apical pacing mimics LBBB - intraventricular dyssynchrony, regional wall strain abnormalities, LV remodeling
- Risk increases with QRS prolongation and worse baseline LV function
- DAVID trial: dual-chamber pacing with high RV pacing rate increased composite HF/death by 1.6× vs. backup VVI
- MOST trial: increased RV pacing frequency in SSS associated with increased AF and HF
- Strategy: minimize RV pacing via MVP/ADI algorithms OR use conduction system pacing
7. Abnormal Pacemaker Rhythms / Pacemaker Malfunction
A. Failure to Pace (No Output)
- Causes: Battery depletion, lead fracture, connector block disconnect, oversensing (inappropriate inhibition)
- ECG: No pacing spike when expected; rate falls below LRL
B. Failure to Capture
- Causes: Lead displacement (most common - early), increased threshold (fibrosis, drugs - Class 1C, amiodarone), perforation, exit block
- ECG: Pacing spike present but NOT followed by a P or QRS complex
- Drugs that raise threshold: Flecainide, chronic amiodarone (especially atrial thresholds)
- Drugs that lower threshold: Glucocorticoids, isoproterenol, epinephrine
C. Oversensing (Inappropriate Inhibition)
- Device senses non-cardiac signals (T waves, myopotentials, EMI, crosstalk) and is inappropriately inhibited
- Crosstalk: Ventricular channel senses atrial pacing spike → inhibits ventricular output (dangerous in pacemaker-dependent patients)
- Myopotential oversensing: More common with unipolar leads
- EMI sources: MRI (requires specific MRI-conditional devices), electrocautery, arc welders, strong magnets
- ECG: Unexplained pauses; pacing spikes absent
D. Undersensing
- Device fails to sense native cardiac activity → paces too frequently or at inappropriate times
- Causes: Lead displacement, low signal amplitude, lead fibrosis, oversized sensing threshold
- ECG: Pacing spikes that fall on or near native beats; escape interval shorter than programmed (Braunwald eFig. 69.9)
E. Pacemaker-Mediated Tachycardia (PMT) (Braunwald; Fuster)
- Occurs in dual-chamber pacemakers
- Mechanism: A PVC or premature beat conducts retrogradely to atrium → retrograde P-wave sensed outside PVARP → triggers ventricular pacing → another retrograde P → endless loop tachycardia
- Rate: = URL (upper rate limit) of the pacemaker - often a sudden jump to 120-150 bpm
- Management: Place magnet (converts to asynchronous, breaks loop); reprogram - lengthen PVARP; reprogram PMT detection algorithm
- Fuster (Ch. 38): PMT can usually be corrected by reprogramming
F. Runaway Pacemaker
- Rare; catastrophic battery depletion or component failure → pacing at very high rates (>200 bpm)
- Management: Magnet placement; device replacement emergency
G. Pacing-Induced Proarrhythmia (Braunwald, Ch. 69)
- RV pacing itself can produce QRS prolongation and trigger arrhythmias
- "Pacing-induced proarrhythmia" - documented but uncommon in isolation
- Torsades de pointes can occur with pause-dependent QT prolongation in bradycardic patients
H. Unexpected Drop in Pacing Rate
- Rate hysteresis: Intentional design - LRL is lower than escape interval; device waits longer before initiating pacing (promotes intrinsic rhythm)
- Battery depletion (ERT/EOL indicators): Rate drop to magnet/backup rate indicates battery near end of life
- Mode switch: Device may switch from DDDR to VVIR during AF → apparent rate change
8. Special Pacing Rhythms on ECG
| Rhythm/Pattern | Description |
|---|---|
| Atrial pacing | Pacing spike before P wave; P morphology different from sinus if from right atrium |
| Ventricular pacing | Wide QRS (LBBB morphology with RV apex pacing); pacing spike immediately before wide QRS |
| AV sequential pacing | Two spikes - one before P, one before wide QRS; fully paced rhythm |
| P-synchronous ventricular pacing | Native P wave tracked by device → ventricular spike + wide QRS after AV delay |
| VVI paced rhythm | Wide QRS complexes at set rate when native rate falls below LRL; no atrial spikes |
| His bundle paced | Pacing spike + narrow QRS (if selective); isoelectric interval between spike and QRS = HV interval |
| LBBAP | Pacing spike + narrow QRS; RBBB-like in V1 with short latency; deep S in V6 |
| Biventricular paced | Pacing spike + fusion of RV and LV activation; QRS narrower than LBBB, RBBB or intermediate morphology |
| Pacemaker Wenckebach | Progressive lengthening of AV interval (VAV interval) until a P-wave falls in PVARP → dropped VP; analogous to Wenckebach |
| 2:1 pacemaker block | Every other P-wave falls in TARP → only every other P tracked → ventricular rate = ½ atrial rate |
| PMT | Sudden tachycardia at URL; P-wave after QRS (retrograde) if visible |
| Pseudofusion | Pacing spike falling on native beat (spike visible but native beat already occurring); no additional activation |
| Fusion beat | Simultaneous pacing and intrinsic activation of same chamber; intermediate QRS morphology |
9. Indications for Permanent Pacing (AHA/ACC 2018/2019 Guidelines - as cited in Fuster, Ch. 38)
Sinus Node Dysfunction (SND)
- Class I (Recommended): Symptomatic bradycardia or pauses caused by SND
- Class I: Symptomatic chronotropic incompetence
- Class III (Harm): Asymptomatic sinus bradycardia or physiologic/sleep-related pauses; SND due to reversible causes
Mode of choice: DDDR (preferred); AAIR if no AV conduction disease; VVIR if permanent AF (Fuster, Ch. 38). SND accounts for 42-60% of new pacemaker implants in North America.
AV Block (Fuster, Table 39-4)
- Class I: Second-degree Mobitz type II (trifascicular block), high-grade AV block, or complete (third-degree) AV block - permanent pacing regardless of symptoms
- Class I: Neuromuscular diseases (myotonic dystrophy, Kearns-Sayre syndrome) with severe AV block or HV interval ≥70 ms
- Class I: Permanent AF with symptomatic bradycardia
- Class I: Drug-induced AV block where drug is necessary and no alternatives exist
- Class IIa: Infiltrative cardiomyopathy (sarcoidosis, amyloidosis) + Mobitz II/high-grade/complete AV block
- Class IIa: Lamin A/C gene mutations (limb-girdle, Emery-Dreifuss muscular dystrophy) + PR >240 ms + LBBB
Mode of choice for AV block:
- Complete AV block: dual-chamber (DDDR) to maintain AV synchrony
- Normal sinus function + AV block: VDD (single-lead dual-chamber tracking)
- Permanent AF + bradycardia: VVIR adequate
- SND + AV block: DDDR
Post-Cardiac Surgery/TAVR (Fuster, Table 38-6)
- Class I: New SND or AV block after CABG, AVR, MVR/repair, TVR repair causing symptoms or hemodynamic instability - permanent pacing before discharge
- Class I: New AV block after TAVR with symptoms/hemodynamic instability not resolving
10. Leadless Pacemakers (Fuster, Ch. 38)
Two commercially available systems:
| Feature | Nanostim LCP (Abbott) | Micra TCP (Medtronic) |
|---|---|---|
| Fixation | Active helix | Nitinol tines |
| Site | RV | RV apical septum |
| Trial | LEADLESS II (526 pts) | Micra TCP (725 pts) |
| Implant success | 95.8% | 99.2% |
| Major complication (6 mo) | 6.7% | 4% |
| Complications | Dislodgement 1.7%, perforation 1.3% | Perforation/effusion 1.6% |
- Post-Approval Registry (Micra, 1817 patients): 99.1% implant success; 2.7% major complications (66% less than IDE study)
- Indications: Primarily permanent AF with bradycardia, SND, AV block where single-chamber ventricular pacing is sufficient
- Limitation: No atrial pacing; no AV synchrony; however, newer dual-chamber leadless systems (Micra AV) can sense atrial contraction via RV accelerometer and provide AV-synchronous pacing
11. Antitachycardia Pacing (ATP) (Braunwald, Ch. 69)
- Delivered by ICDs to terminate ventricular tachycardia
- Burst pacing at a rate slightly faster than VT rate captures the reentrant circuit and terminates VT
- Burst ATP: All stimuli at same short cycle length
- Ramp ATP: Progressively decreasing cycle lengths (accelerating)
- ATP avoids painful defibrillation shocks; effective for slower VT (<200 bpm)
- Risk: ATP can accelerate VT - always backed by shock therapy in ICD
12. Drug Interactions with Pacemakers (Braunwald, Table 69.1)
| Drug Effect | Drugs |
|---|---|
| Raise pacing threshold | Class 1C (flecainide); chronic amiodarone (especially atrial) |
| Lower pacing threshold | Glucocorticoids; isoproterenol; epinephrine |
| Increase atrial pacing burden | Beta-blockers, amiodarone, lithium (cause sinus bradycardia) |
| Increase ventricular pacing burden | Beta-blockers, amiodarone (slow AV conduction) |
13. Key Summary: Pacing Mode Selection
| Clinical Situation | Recommended Mode |
|---|---|
| SSS, no AV disease | AAIR |
| SSS, possible AV disease | DDDR |
| Permanent AF + bradycardia | VVIR |
| AV block, normal sinus | VDD or DDDR |
| SSS + AV block | DDDR |
| AV block, permanent AF | VVIR |
| LBBB + reduced EF (CRT) | DDD-BiV or CSP |
| Pacemaker-dependent, OR | VOO (via magnet) or programmed asynchronous |
| Chronotropic incompetence | Any mode + R (rate-responsive) |
Recent Evidence Update (PubMed, 2022-2026)
- [PMID 41957548] (Clin Cardiol 2026): Meta-analysis confirms Left Bundle Branch Area Pacing (LBBAP) is superior to RV pacing in conduction system disorders - lower QRS duration, better LVEF preservation
- [PMID 40644356] (Europace 2025): Conduction system pacing ≥ biventricular pacing after AV node ablation - equivalent or better outcomes
- [PMID 36352513] (Europace 2023): Upgrading RV pacemakers to biventricular or CSP pacing - systematic review supports clinical benefit in pacing-induced cardiomyopathy
- [PMID 39892565] (Int J Cardiol 2025): Rate-adaptive pacing significantly improves exercise capacity and quality of life in chronotropic incompetence
Key Figures Available in Braunwald's (Ch. 69)
The textbook contains several key figures including:
- Figure 69.6: Permanent His bundle pacing - 12-lead ECG showing atrial-synchronous ventricular pacing with narrow QRS; isoelectric HV interval between spike and QRS; X-ray showing lead positions
- eFigure 69.7: Left bundle branch area pacing - V1-V3 comparison of BiV vs. LBBAP with QRS duration comparison; lead placement with contrast injection; PA and lateral X-rays
- Figure 69.7: Pacing lead design - passive vs. active fixation; coaxial vs. coradial lead construction
- Figure 69.9: Single chamber modes - VOO, VVI, AAI timing cycles
- eFigure 69.8: DDI and DDD pacing mode timing diagrams
Primary references: Braunwald's Heart Disease, 11e, Chapter 69 (Pacemakers/ICDs) | Fuster and Hurst's The Heart, 15th Ed, Chapters 38-39 (Cardiac Pacing) | AHA/ACC 2018 Bradycardia/CRS Pacemaker Guidelines
Explain pacemaker rhythms using ECGs
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
I have all the material needed for a comprehensive, image-rich answer. Let me now write the detailed response.
Pacemaker Rhythms on ECG: A Complete Visual Guide
Sources: Braunwald's Heart Disease 11e (Ch. 69), Rosen's Emergency Medicine 9e (Ch. 66), Fuster and Hurst's The Heart 15e (Ch. 38)
The Pacing Spike: The Foundation of Every Pacemaker ECG
Before analyzing any pacemaker rhythm, recognize these fundamentals:
- Pacing spike (stimulus artifact): A sharp, narrow vertical deflection on the ECG immediately preceding a paced complex
- Unipolar leads: Produce a large, obvious spike (large "antenna" between tip electrode and pulse generator)
- Bipolar leads: Produce a small, subtle spike - easily missed on standard 12-lead ECGs (Braunwald, Ch. 69)
- Capture: A pacing spike that successfully depolarizes the chamber - confirmed by a P wave (atrial capture) or QRS complex (ventricular capture) immediately following the spike
- The key rule: Every spike should be followed by capture; every capture should be preceded by a spike (in a normally functioning device)
1. Normal Single-Chamber Ventricular Pacing (VVI)
ECG Features:
- Pacing spike immediately before each paced QRS
- Wide QRS complex (>120 ms) - because depolarization spreads via slow myocardial cell-to-cell conduction, not the fast Purkinje system
- Left bundle branch block (LBBB) morphology - because the RV apex is paced first: broad R in I, aVL; QS or rS in V1-V3; broad R in V5-V6
- Discordant ST-T changes (ST depression and T-wave inversion in leads with tall R waves = appropriate secondary repolarization changes, NOT ischemia)
- When native rate exceeds the programmed LRL, native QRS complexes appear - the pacemaker is appropriately inhibited
Rosen's (Fig. 66.1): "Each pacemaker spike is followed by a paced QRS complex with a rate of 75 beats/min. The third QRS from the left has a slightly different morphology than the paced QRS complexes. It is an intrinsic QRS complex that is sensed by the pacemaker, and a paced beat does not occur again until the programmed rate of the pacemaker is exceeded."

Key points for VVI:
- Rate = programmed lower rate limit when native rate is slow
- Intrinsic beats reset the escape interval
- No AV synchrony - no relationship between P waves and paced QRS complexes
- Underlying P waves may be visible, dissociated from the QRS
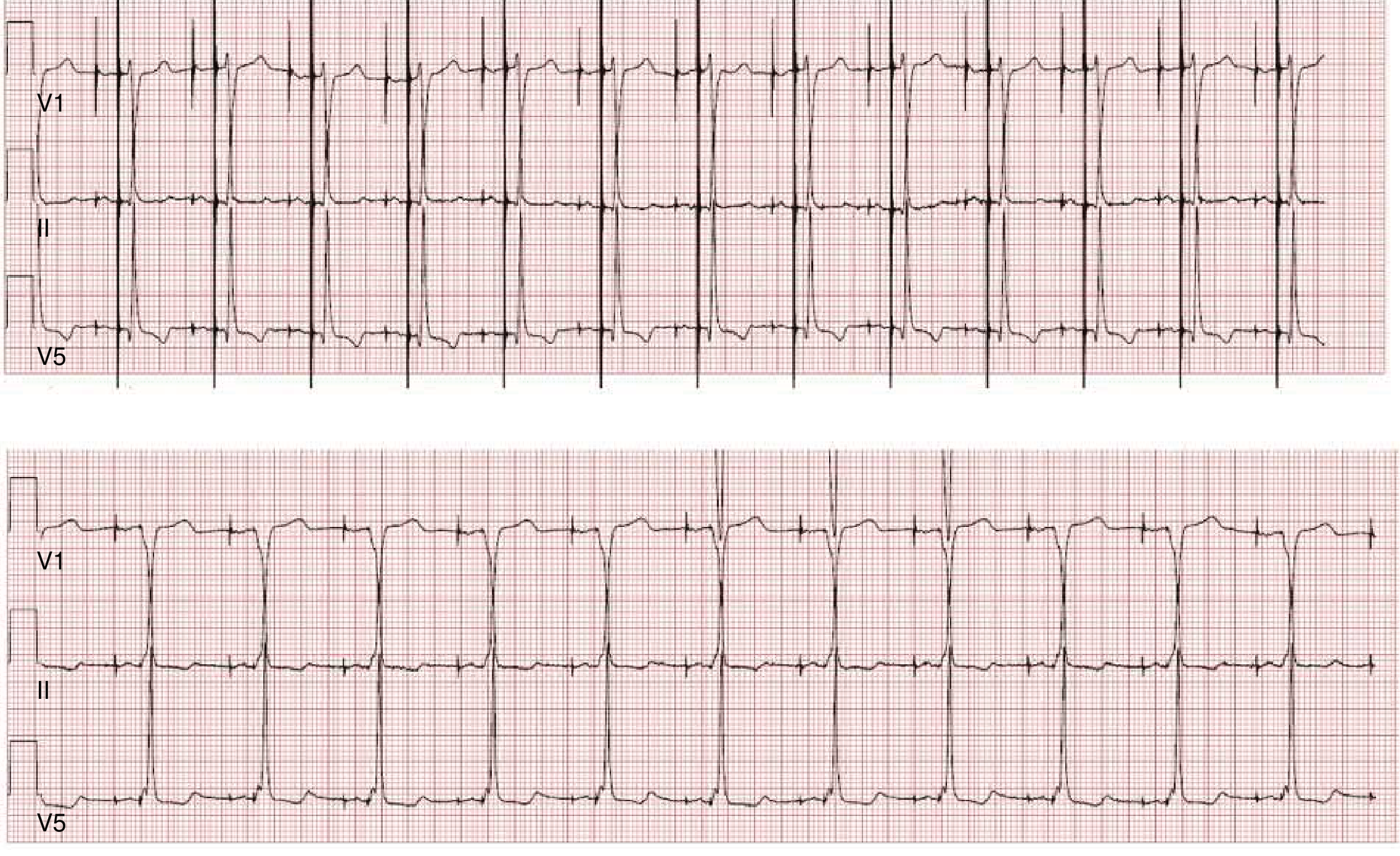
2. Normal Dual-Chamber Pacing (DDD) - 12-Lead ECG
ECG Features (Fully Paced - AP-VP):
- Two pacing spikes before each QRS complex: atrial spike → P wave → AV delay → ventricular spike → wide QRS (LBBB morphology)
- First spike (atrial) is often very small or barely visible; second spike (ventricular) is larger
- The QRS is wide with LBBB pattern (as in VVI)
- Regular rate at the programmed LRL
Rosen's (Fig. 66.2): "Each QRS complex is preceded by two pacemaker spikes. The first spike results in atrial depolarization, and the second produces a wide QRS complex. The QRS complex is conducted with a left bundle branch morphology, which is expected with endocardial pacing at the right ventricular apex."
ECG Features (P-Tracking / P-Synchronous Ventricular Pacing - AS-VP):
Rosen's (Fig. 66.3): "Paced QRS complexes occur after spontaneous or intrinsic P waves are sensed and atrioventricular conduction delay exceeds the pacemaker's programmed AV interval. Although the pacemaker is a dual-chamber device, two spikes may not always be seen preceding every QRS complex, and the presence of only one spike, or no spikes, should not be interpreted as evidence of pacemaker malfunction."
Important point: In DDD pacing, you may see:
- Two spikes (AP-VP): both chambers paced
- One spike only (AS-VP): native P sensed, ventricle paced
- No spikes (AS-VS): entirely intrinsic, pacemaker tracking and inhibiting
- The absence of visible spikes does NOT mean malfunction
3. Single-Chamber Mode Timing Diagrams (Braunwald)
The following diagram from Braunwald (Fig. 69.9) illustrates the timing logic of all three single-chamber modes:
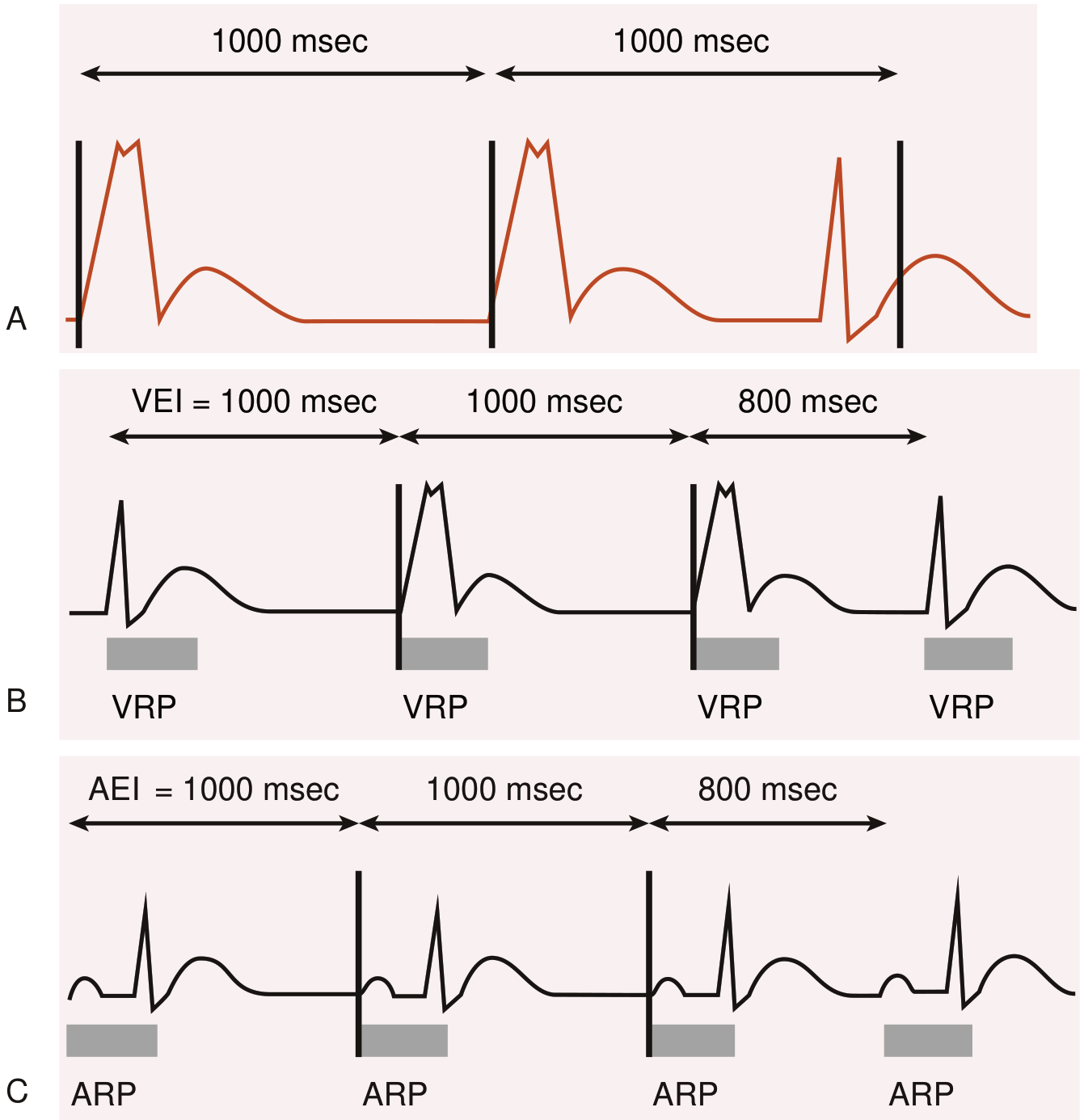
VOO (Asynchronous):
- Fixed spikes at regular intervals regardless of native beats
- Can cause R-on-T phenomenon
- Produced by magnet application over most pacemakers
VVI:
- Pacing spike → wide QRS when rate falls below LRL
- Native QRS inhibits the pacemaker, resets escape interval
AAI:
- Pacing spike → P wave when sinus rate falls below LRL
- Native P waves inhibit the pacemaker
- Native conduction to ventricles produces narrow QRS (if intact)
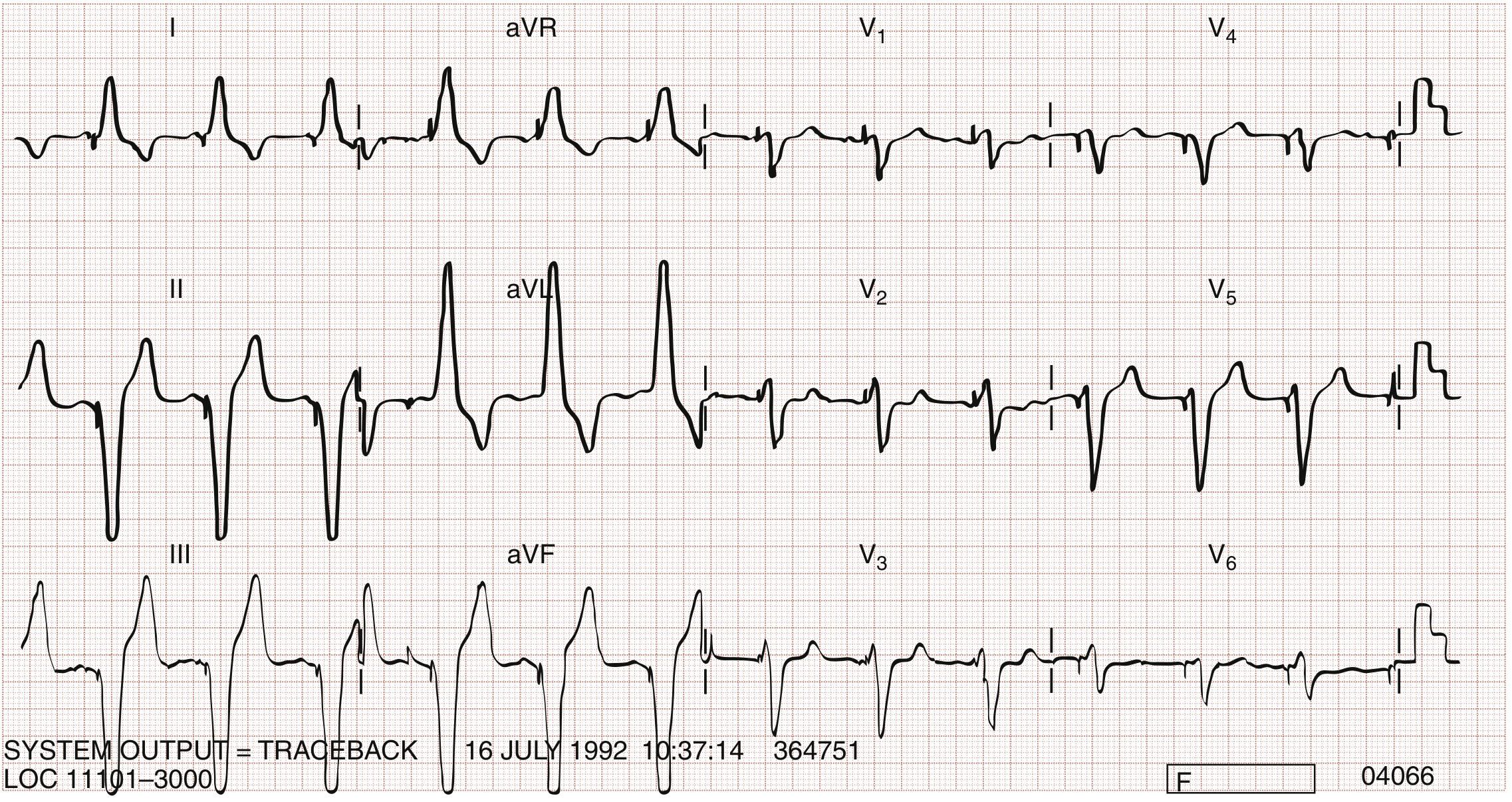
4. Biventricular (CRT) Paced Rhythm
Rosen's (Fig. 66.4): "The paced QRS complexes have an S wave in lead I and an R wave in lead V1, that are distinctly different from the morphology and axes seen with right ventricular apical pacing."
CRT vs. RV Pacing Morphology Comparison:
| Feature | RV Apical Pacing | Biventricular (CRT) Pacing |
|---|---|---|
| QRS width | Very wide (>160 ms) | Narrower (may approach 120-130 ms) |
| Lead I | Broad R | S wave (negative) |
| V1 | QS or rS (negative) | Positive R or Rs |
| Axis | Left axis | More rightward/superior |
| QRS morphology | Pure LBBB | RBBB-like or intermediate |
The positive R in V1 and S wave in lead I are the hallmarks of CRT that distinguish it from standard RV pacing.
5. Failure to Capture
Definition: Pacing spike present but NOT followed by a P wave or QRS complex
ECG Features:
- Pacing spikes fire at the programmed rate
- Spikes are NOT followed by captured complexes (no P or QRS after the spike)
- The ventricular rate may be dangerously slow if the patient is pacemaker-dependent
- Intermittent failure to capture: some spikes capture, others do not
Causes (Rosen's, Box 66.2):
- Lead displacement (most common, especially within first month)
- Lead fracture (current leakage)
- Battery depletion (late sign)
- Exit block: ischemia/infarction at lead tip, hyperkalemia, amiodarone
- Lead disconnection from pulse generator
Clinical Note: An RV-paced complex that shows RBBB morphology (rather than LBBB) suggests lead displacement - the lead is no longer in the RV apex (Rosen's, Key Concepts).
6. Undersensing (Failure to Sense)
Definition: Pacemaker fails to detect intrinsic cardiac activity → fires inappropriately
ECG Features:
- Pacing spikes appear too early - earlier in the cycle than expected based on programmed rate
- Spike may or may not produce capture (depends on whether it falls in the refractory period)
- Native beats are present but not recognized by the device
- If a spike falls during the T wave → risk of R-on-T and VF
Rosen's: "Undersensing is typically recognized electrocardiographically as the appearance of pacemaker spikes occurring earlier in the cycle than would be expected, based on the programmed rate."
Braunwald's Undersensing ECG (eFig. 69.9):

Key distinguishing point: Undersensing → spikes come too early (shorter cycle than expected). Oversensing → spikes come too late or not at all (artificially prolonged interval or absent spikes).
7. Oversensing (Inappropriate Inhibition)
Definition: Pacemaker senses non-cardiac or non-relevant signals → inappropriately inhibits pacing output
ECG Features:
- Prolonged pauses in pacing (longer than programmed escape interval)
- In pacemaker-dependent patients: flat line / profound bradycardia
- Irregular pacing intervals
- The pacemaker "thinks" it is seeing cardiac activity and withholds output
Common Sources of Oversensed Signals:
- T wave oversensing: More common in ICDs; the tall T wave exceeds sensing threshold
- Myopotentials (pectoralis muscle): More common with unipolar leads - patient moving arms
- Electromagnetic interference (EMI): Electrocautery in OR (most common clinical concern), MRI, arc welders
- Crosstalk: Ventricular channel senses the atrial pacing spike in DDD pacemakers
Management: Apply magnet (converts to asynchronous VOO/AOO/DOO) - overrides sensing, restores fixed-rate pacing, confirms device function.
8. Pacemaker-Mediated Tachycardia (PMT / Endless-Loop Tachycardia)
Mechanism (Braunwald, Ch. 69):
- A PVC (or any beat) conducts retrogradely to the atrium
- The retrograde P wave is sensed by the atrial channel outside the PVARP
- This sensed atrial event triggers ventricular pacing after the AV delay
- That paced ventricular beat again conducts retrogradely...
- → "Endless loop" - the pacemaker is trapped in a reentrant circuit
ECG Features:
- Sudden regular tachycardia at or near the programmed upper rate limit (typically 120-150 bpm)
- Ventricular pacing spikes at the upper rate limit
- Retrograde P waves visible after each paced QRS (if discernible) - negative in inferior leads
- Device markers show: AS → VP → AS → VP pattern (retrograde P sensed as AS, triggers VP)
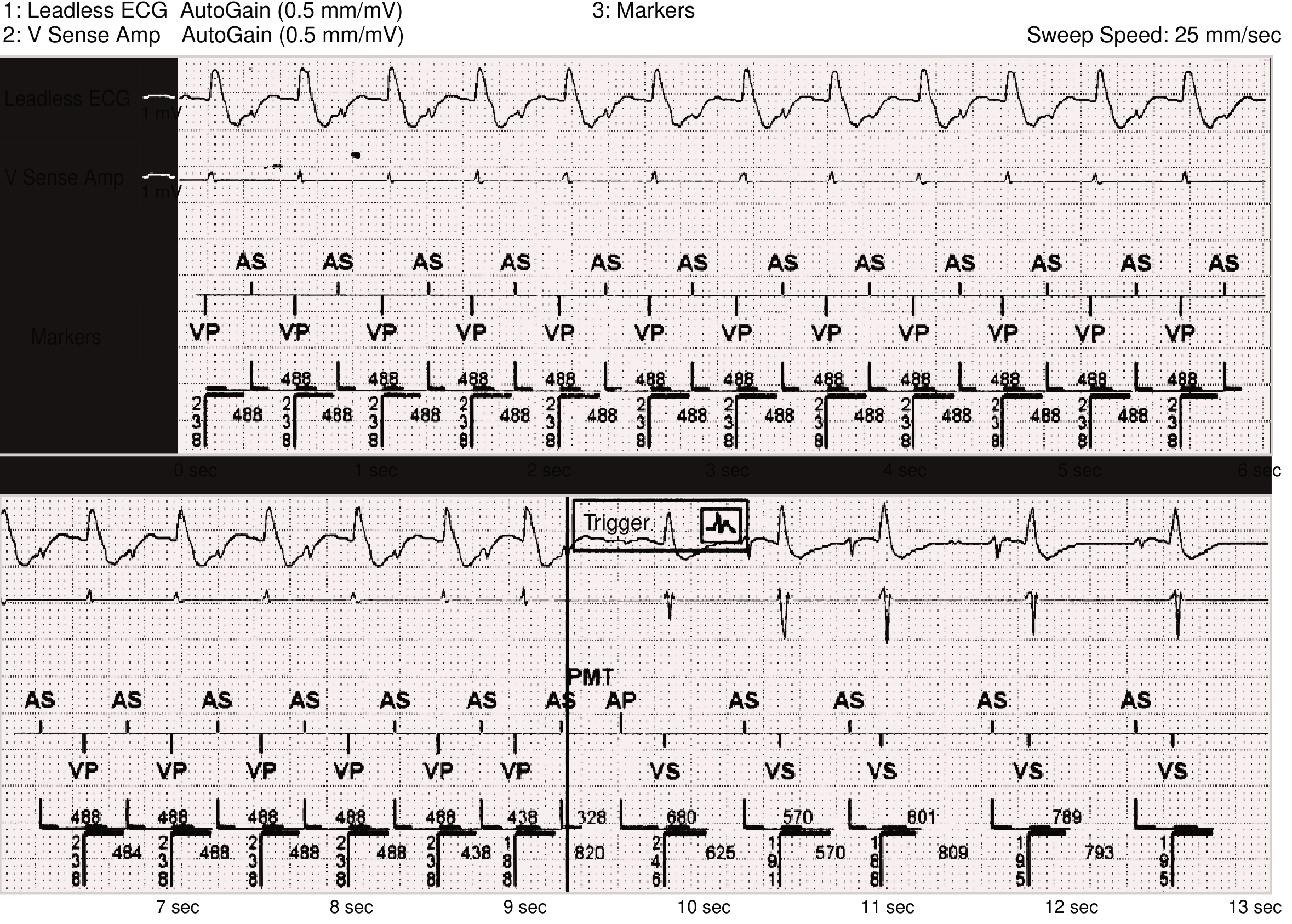
Termination/Prevention:
- Magnet application: Converts to asynchronous, breaks the loop
- Reprogram PVARP: Lengthen to exceed VA conduction time
- PMT detection algorithms: Device extends PVARP after a PVC, or omits tracking for one atrial event to break the cycle
9. Pacemaker Upper Rate Behavior (Wenckebach/2:1 Block)
In DDD mode, when the atrial rate exceeds the upper rate limit:
Wenckebach Upper Rate Behavior:
- The AV interval progressively lengthens (device delays VP to avoid exceeding URL)
- Eventually a P wave falls within the PVARP → not tracked → dropped VP
- Results in irregular ventricular rhythm that mimics Wenckebach block
- ECG: Progressive AV delay → dropped beat → regular cycle restarts
2:1 Pacemaker Block:
- Every alternate P wave falls within the TARP (AV interval + PVARP)
- Only every other P wave is tracked → ventricular rate = ½ atrial rate
- ECG: Sudden drop of ventricular rate to half the atrial rate
- Regular P waves; every other P followed by VP spike + wide QRS; alternating P waves with no response
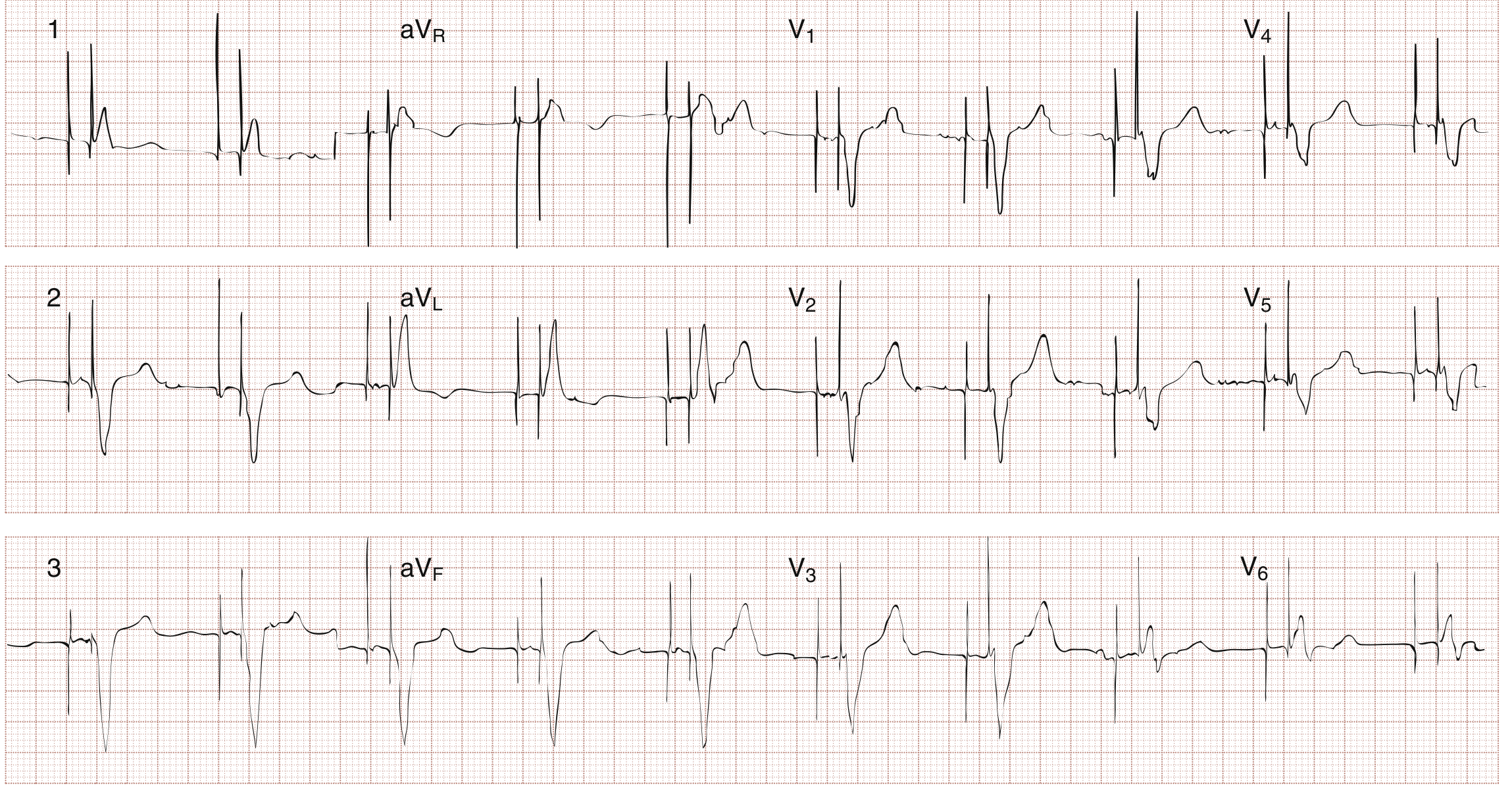
10. His Bundle Pacing - ECG Pattern
Key ECG Feature: Pacing spike followed by a narrow QRS (with or without an isoelectric interval)
- Selective HBP: Spike → isoelectric interval (= HV conduction time, ~35 ms) → narrow QRS (identical to intrinsic QRS)
- Non-selective HBP: Spike → narrow QRS with slight pre-excitation morphology (local myocardium + His bundle captured)
- V1: rSR' or similar to native conduction
- X-ray: Lead tip near the tricuspid annulus/His bundle region
The narrow QRS on the ECG (vs. wide QRS with RV pacing) is the entire point - it confirms physiologic conduction.
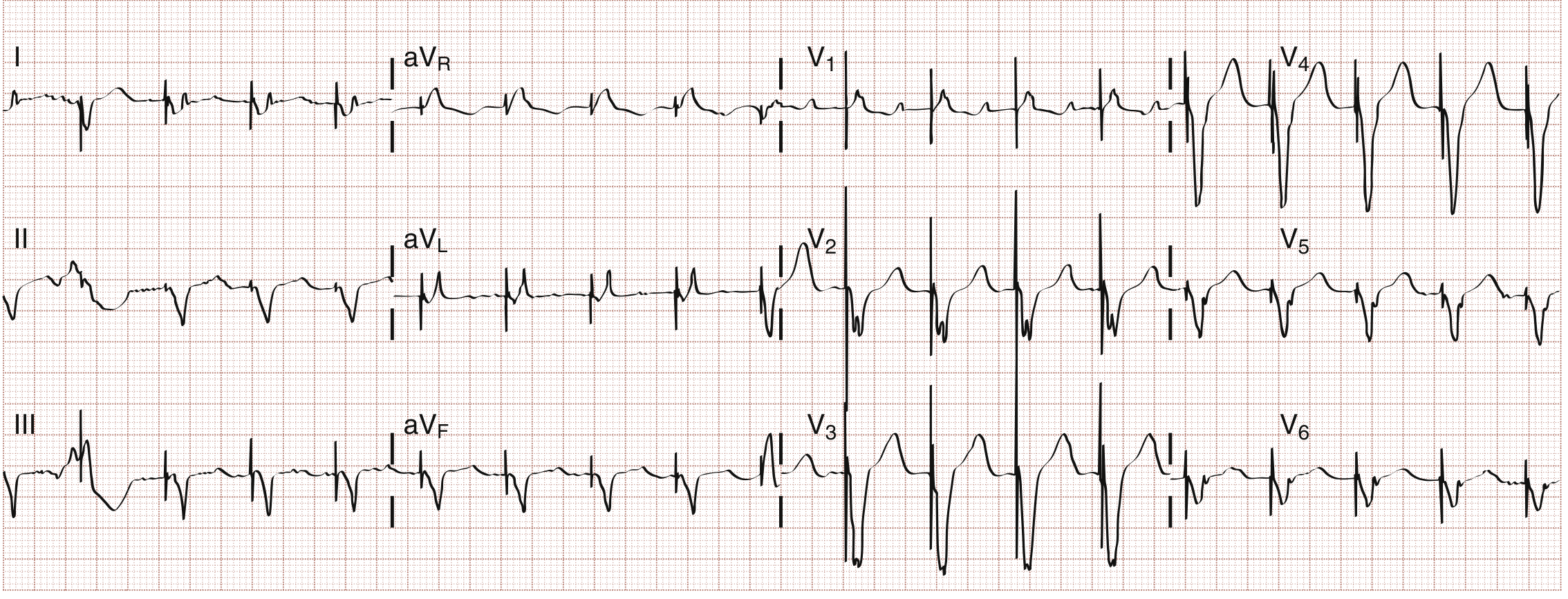
11. Mode Switch - ECG Appearance
When a DDD pacemaker detects a rapid atrial tachyarrhythmia (AF, atrial flutter):
- Device automatically switches from DDD (P-tracking) to VVIR or DDI to prevent rapid ventricular tracking
- ECG: Transition from regular P-synchronous VP to ventricular pacing at a non-tracking rate
- Rate abruptly changes; P waves no longer tracked
- Returns to DDD when atrial rate slows
12. Fusion and Pseudofusion Beats
These are normal findings on pacemaker ECGs, not malfunctions:
Fusion Beat:
- Simultaneous pacing and intrinsic activation of the SAME chamber
- QRS morphology is intermediate between pure paced and pure intrinsic
- Occurs when intrinsic beat and paced beat merge
- Normal finding
Pseudofusion Beat:
- Pacing spike falls ON a native beat already in progress
- The spike contributes nothing to depolarization (myocardium already refractory)
- QRS morphology = identical to native QRS (the spike is cosmetic)
- Marker channels show "sensed" annotation at the same time as the spike
- Normal finding - does NOT indicate failure to sense (the device DID sense, but after output was already committed)
Summary ECG Recognition Table
| ECG Finding | Interpretation |
|---|---|
| Spike → wide LBBB QRS, no P spike | VVI or VDD ventricular pacing |
| Two spikes → P then wide QRS | DDD, fully paced (AP-VP) |
| Native P → pause → spike → wide QRS | DDD P-tracking (AS-VP) |
| Spike → wide QRS with R in V1, S in I | Biventricular/CRT pacing |
| Spike → NO QRS | Failure to capture |
| Spike → narrow QRS ± isoelectric interval | His bundle pacing |
| Spike too early (before escape interval) | Undersensing |
| Long pause, no spike (pacemaker-dependent) | Oversensing / failure to pace |
| Regular tachycardia at URL, retrograde P after QRS | Pacemaker-mediated tachycardia |
| Progressive AV prolongation → dropped beat | Upper rate Wenckebach behavior |
| Every other P tracked, rate halved | 2:1 pacemaker block (TARP exceeded) |
| Intermediate QRS morphology | Fusion beat (normal) |
| Spike on native QRS, morphology unchanged | Pseudofusion (normal) |
| RBBB morphology in paced rhythm | Abnormal - lead displacement |
| Fixed-rate spikes ignoring native beats | Asynchronous mode / magnet effect |
Sources: Rosen's Emergency Medicine 9e, Ch. 66 (Figs. 66.1-66.7) | Braunwald's Heart Disease 11e, Ch. 69 (Figs. 69.9, 69.11, 69.13, eFig. 69.9) | Fuster and Hurst's The Heart 15e, Ch. 38
This is a shared conversation. Sign in to Orris to start your own chat.