Acute inflammatory response for writing in prelims exam 6 or 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed to write a complete, exam-ready answer. Here is the full structured response for a 6 or 10 mark prelims question:
Acute Inflammatory Response
(Source: Robbins & Kumar Basic Pathology, Robbins Cotran & Kumar Pathologic Basis of Disease)
Definition
Acute inflammation is the rapid, stereotyped response of living tissues to injury, infection, or foreign bodies, designed to deliver leukocytes and plasma proteins to the site of damage. It is characterised by the classic cardinal signs: redness (rubor), warmth (calor), swelling (tumor), pain (dolor), and loss of function (functio laesa).
Components / Steps of Acute Inflammation
Acute inflammation has three major components:
- Dilation of small vessels (vasodilation)
- Increased vascular permeability
- Emigration of leukocytes from the microcirculation
All occur mainly in postcapillary venules and are driven by chemical mediators (cytokines, histamine, etc.).
1. Vascular Reactions
a) Changes in Vascular Flow and Caliber
- Vasodilation is the earliest change - responsible for redness and warmth.
- The most important mediator of vasodilation is histamine.
- Vasodilation is followed by slowing of blood flow (stasis) and engorgement of small vessels (hyperemia).
b) Increased Vascular Permeability
- Vasodilation is quickly followed by increased permeability of the microvasculature, leading to outpouring of protein-rich fluid into extravascular tissues - this is called exudation.
- Exudate = high protein, cellular debris, increased specific gravity (implies active inflammation).
- Transudate = low protein (mainly albumin), no cellular debris, low specific gravity (due to hydrostatic/osmotic imbalance, not inflammation).
- Pus = purulent exudate rich in neutrophils and cell debris.
Mechanism of increased permeability:
- Contraction of endothelial cells creating interendothelial gaps - elicited by histamine, bradykinin, leukotrienes.
- Occurs rapidly (within 15-30 minutes) and is short-lived.
- In burns, direct endothelial injury causes immediate, sustained leakage.
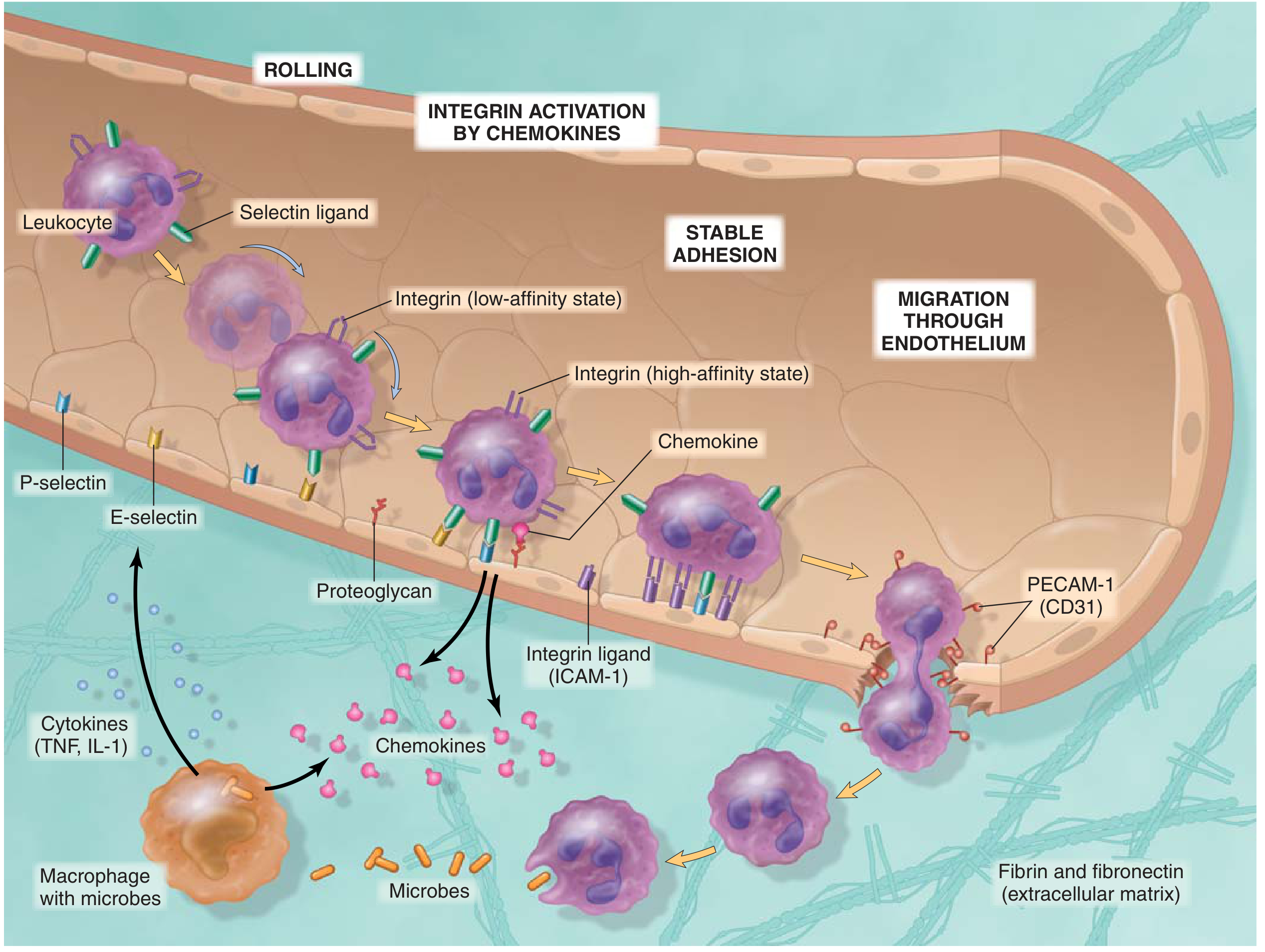
2. Leukocyte Recruitment (Cellular Events)
This is the most important component of the defensive reaction. The sequence is:
Step 1: Margination and Rolling
- Under normal laminar flow, leukocytes are pushed to the periphery of the vessel as blood slows (stasis).
- Leukocytes move to the vessel wall - margination.
- They then bind loosely and tumble along the endothelial surface - rolling.
- Mediated by selectins: E-selectin and P-selectin on endothelium; L-selectin on leukocytes.
- P-selectin is stored in Weibel-Palade bodies; mobilised within minutes by histamine/thrombin.
Step 2: Firm Adhesion
- Activated endothelium expresses ICAM-1 (intercellular adhesion molecule-1).
- Leukocytes express integrins (LFA-1, MAC-1) which bind ICAM-1 in a high-affinity state after activation by chemokines.
- This causes firm, stable adhesion.
Step 3: Transmigration (Diapedesis)
- Leukocytes squeeze between endothelial cells (predominantly at intercellular junctions).
- Mediated by PECAM-1 (CD31) - expressed on both leukocytes and endothelium.
- Leukocytes then penetrate the basement membrane using collagenases.
Step 4: Chemotaxis
- Leukocytes migrate toward the site of injury along a chemical gradient (chemotaxis).
- Key chemoattractants:
- Exogenous: bacterial products (e.g., N-formyl-methionine peptides)
- Endogenous: C5a (complement), LTB4 (arachidonic acid metabolite), IL-8 (chemokine)
3. Phagocytosis and Killing
Once at the site, neutrophils and macrophages perform phagocytosis:
- Recognition and attachment - opsonins (IgG, C3b) coat the target and bind receptors (Fc receptor, CR1).
- Engulfment - cytoplasmic extensions surround the particle forming a phagosome.
- Killing and degradation - phagosome fuses with lysosome to form phagolysosome.
Killing mechanisms:
- Oxygen-dependent (most important): Respiratory burst generates reactive oxygen species (ROS) via NADPH oxidase; myeloperoxidase (MPO) converts H2O2 + Cl- to hypochlorous acid (HOCl) - potent microbicidal agent.
- Oxygen-independent: Bactericidal permeability increasing protein (BPI), defensins, lysozyme, lactoferrin, acid hydrolases.
Neutrophil Extracellular Traps (NETs)
- Activated neutrophils release chromatin + histones forming fibrillar networks that trap and kill microbes extracellularly.
- NETs form at the cost of neutrophil death.
4. Mediators of Inflammation
| Mediator | Source | Actions |
|---|---|---|
| Histamine | Mast cells, basophils | Vasodilation, increased permeability |
| Serotonin | Platelets | Vasoconstriction, increased permeability |
| Prostaglandins (PGE2, PGI2) | Arachidonic acid via COX | Vasodilation, fever, pain |
| Leukotrienes (LTC4, LTD4, LTE4) | Arachidonic acid via LOX | Increased permeability, bronchoconstriction |
| LTB4 | Arachidonic acid | Potent chemotaxis for neutrophils |
| PAF (Platelet-activating factor) | Leukocytes, mast cells | Increased permeability, platelet aggregation |
| TNF, IL-1 | Macrophages | Endothelial activation, fever, systemic effects (acute phase response) |
| IL-8 (CXCL8) | Macrophages, endothelium | Neutrophil chemotaxis |
| C3a, C5a | Complement | Vasodilation, chemotaxis (anaphylatoxins) |
| Bradykinin | Kinin system | Vasodilation, pain, increased permeability |
| Nitric oxide (NO) | Endothelium, macrophages | Vasodilation, microbicidal |
5. Morphologic Patterns of Acute Inflammation
| Pattern | Features | Example |
|---|---|---|
| Serous | Watery fluid, low protein, few cells | Blister in skin burns |
| Fibrinous | Fibrin exudate - "bread-and-butter" pericarditis | Uremic pericarditis |
| Purulent (Suppurative) | Pus - rich in neutrophils, liquefactive | Lung abscess, furuncle |
| Ulceration | Surface epithelial defect due to necrosis | Peptic ulcer |
6. Outcomes of Acute Inflammation
Three possible outcomes:
-
Complete resolution - removal of cellular debris and microbes by macrophages; resorption of edema via lymphatics. Occurs when injury is limited and parenchymal cells can regenerate. This is the ideal outcome.
-
Healing by scarring (fibrosis) - occurs after substantial tissue destruction, in tissues incapable of regeneration, or when there is abundant fibrin. Connective tissue replaces the damaged area.
-
Progression to chronic inflammation - when the injurious agent persists or healing is impaired. Characterized by macrophages, lymphocytes, plasma cells, and fibrosis.
7. Termination of Acute Inflammation
The reaction subsides because:
- No further leukocyte recruitment (stimulus eliminated)
- Mediators are short-lived and decline if not continuously produced
- Neutrophils have short life spans (they undergo apoptosis)
- Active "stop" signals are generated: lipoxins, resolvins, protectins (derived from omega-3 fatty acids) suppress inflammation
Summary Table (for quick revision)
| Component | Key Event | Key Mediator |
|---|---|---|
| Vasodilation | Erythema, warmth | Histamine, NO |
| Increased permeability | Exudate formation | Histamine, bradykinin, LTC4 |
| Leukocyte rolling | Selectin-mediated | E/P-selectin, L-selectin |
| Firm adhesion | Integrin-ICAM binding | LFA-1/MAC-1, ICAM-1 |
| Transmigration | Diapedesis | PECAM-1 (CD31) |
| Chemotaxis | Directed migration | C5a, LTB4, IL-8 |
| Killing | Respiratory burst | NADPH oxidase, MPO |
Sources: Robbins & Kumar Basic Pathology, 11th ed.; Robbins, Cotran & Kumar Pathologic Basis of Disease, 10th ed.
Exam tip (6 marks): Cover definition + 3 vascular events + leukocyte steps (rolling-adhesion-transmigration-chemotaxis) + outcomes in 3-4 short paragraphs.
Exam tip (10 marks): Add mediators table, morphologic patterns, phagocytosis mechanisms (O2-dependent vs. O2-independent), NETs, and termination of the response.
This is a shared conversation. Sign in to Orris to start your own chat.