Give me details about gastritis
Reading File
Finding Sources
Searching PubMed
gastritis diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent content from multiple authoritative textbooks. Let me compile the comprehensive answer.
Gastritis
Gastritis is histologically documented inflammation of the gastric mucosa. This is an important distinction: the term should not be used interchangeably with "dyspepsia" or applied to mucosal erythema seen at endoscopy alone. When inflammatory cells are absent or sparse, the term gastropathy is more accurate. The correlation between histologic gastritis, clinical symptoms, and endoscopic findings is generally poor. - Harrison's Principles of Internal Medicine 22E, p. 2580; Robbins & Cotran Pathologic Basis of Disease
Classification
Gastritis is classified by time course, histologic features, and anatomic distribution:
I. Acute Gastritis
- Acute H. pylori infection
- Other acute infectious gastritides: bacterial (non-HP), H. heilmannii, phlegmonous, mycobacterial, syphilitic, viral, parasitic, fungal
II. Chronic Atrophic Gastritis
- Type A: Autoimmune, body-predominant
- Type B: H. pylori-related, antral-predominant
- Indeterminate
III. Uncommon forms (eosinophilic, lymphocytic, collagenous, granulomatous, reflux, radiation)
- Harrison's, Table 335-10
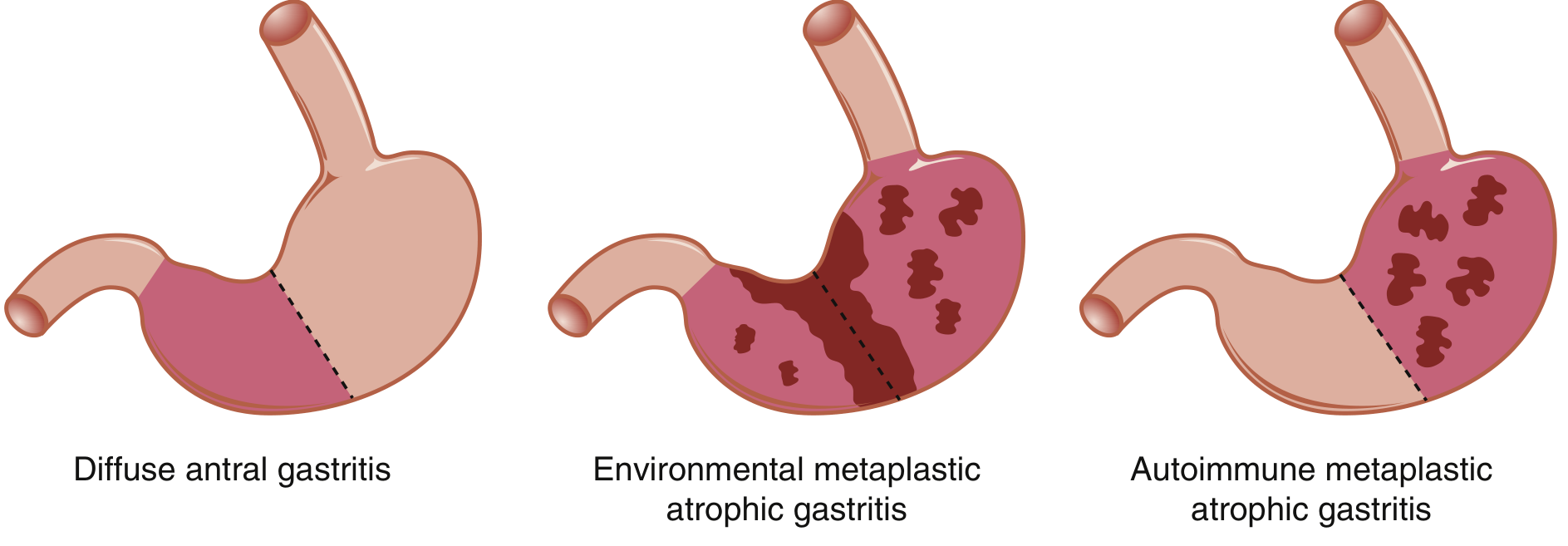
Topographic Patterns of Chronic Gastritis
Etiology and Pathophysiology
1. H. pylori Gastritis (Most Common Cause of Chronic Gastritis)
H. pylori is a gram-negative, helical/spiral-shaped, flagellated bacterium. It infects over 50% of the world's population - 70-80% in developing nations - making it the most common chronic bacterial infection in humans. Infection is typically acquired in childhood and strongly linked to low socioeconomic status. - Sleisenger & Fordtran's, p. 910
Mechanism:
- Infects superficial layers of gastric mucosa, initially causing diffuse antral gastritis
- Induces persistent neutrophilic + chronic inflammatory infiltrate (lymphocytes, plasma cells)
- cag pathogenicity island (cag PAI): strains expressing CagA are associated with more severe disease and higher cancer risk
- Activates NF-κB in gastric epithelial cells → upregulation of IL-8 and other pro-inflammatory cytokines
- Urease produces NH3 from urea, damaging mucosal cells
- Oxidative stress via reactive oxygen species contributes to DNA damage
- Induces MALT (mucosa-associated lymphoid tissue), which can give rise to B-cell lymphomas (MALTomas)
Progression:
- Antral-predominant → can progress to pangastritis with glandular atrophy → intestinal metaplasia → dysplasia → gastric adenocarcinoma (Correa cascade)
- H. pylori gastritis with antral predominance → increased acid → predisposes to peptic ulcer disease (duodenal)
- Pangastritis with atrophy → reduced acid → predisposes to gastric ulcer and cancer
- Robbins & Cotran, p. 720; Bailey & Love's Surgery 28th Ed., p. 1177
2. Autoimmune Atrophic Gastritis (Type A)
- Circulating anti-parietal cell and anti-intrinsic factor antibodies
- Affects the gastric body/corpus (oxyntic glands), sparing the antrum
- Loss of parietal cells → achlorhydria + loss of intrinsic factor
- Loss of intrinsic factor → vitamin B12 malabsorption → pernicious anaemia if untreated
- Achlorhydria → hypergastrinaemia (antral G-cells overactivated) → ECL cell hyperplasia → possible carcinoid tumors
- Associated with gastric cancer risk; endoscopic surveillance may be warranted
- Bailey & Love's, p. 1177; Robbins & Cotran, p. 720
3. NSAIDs and Alcohol
- NSAIDs inhibit COX-1 → reduce prostaglandin synthesis → impair mucosal protective mechanisms → erosive/chemical gastritis
- One of the most common causes of acute/erosive gastritis in clinical practice
- Robbins & Cotran, p. 719
4. Acute Infectious (Phlegmonous / Emphysematous Gastritis)
- Phlegmonous gastritis: infection of gastric submucosa and muscularis propria by invasive organisms (gram-negative bacilli, anaerobes, streptococci, fungi). Often spares the mucosa.
- Emphysematous gastritis: severe form with gas-producing organisms (Clostridium perfringens, E. coli, S. aureus); gas visible in gastric wall and portal venous system on CT/plain films
- Risk factors: heavy alcohol intake, recent GI surgery, corrosive ingestion, AIDS, immunosuppression, diabetes
- Presentation: septic appearance, acute upper abdominal pain, peritonitis, fever, hypotension
- Can be fatal; may progress to gastric gangrene
- Sleisenger & Fordtran's, p. 909
5. Reflux Gastritis
- Caused by enterogastric bile reflux
- Histologically distinct from other types
- Common after gastric surgery; occasionally occurs without prior surgery
- Bailey & Love's, p. 1177
Clinical Features
| Feature | Acute Gastritis | Chronic Gastritis |
|---|---|---|
| Symptoms | Epigastric pain, nausea, vomiting (or asymptomatic) | Often clinically silent |
| Course | Sudden onset | Slowly progressive |
| Key finding | Mucosal erythema, erosions | Mucosal atrophy, intestinal metaplasia |
| Main risk | Erosions, bleeding | Peptic ulcer, gastric cancer, MALToma |
Clinical manifestations correlate poorly with histologic severity. Many patients with extensive chronic gastritis remain asymptomatic for years. - Harrison's, p. 2581
Complications
| Complication | Underlying Form |
|---|---|
| Peptic ulcer disease (duodenal) | H. pylori antral gastritis (hyperchlorhydria) |
| Peptic ulcer disease (gastric) | Pangastritis with atrophy |
| Gastric adenocarcinoma | Intestinal metaplasia → dysplasia (all forms of chronic gastritis) |
| MALToma (B-cell lymphoma) | H. pylori-induced MALT |
| Pernicious anaemia | Autoimmune atrophic gastritis |
| ECL cell carcinoid | Autoimmune gastritis (chronic hypergastrinaemia) |
- Robbins & Cotran, p. 720
Diagnosis
- Gold standard: Mucosal biopsy at endoscopy with histopathology
- H. pylori testing:
- Non-invasive: urea breath test (UBT), stool antigen test, serology (less reliable for active infection)
- Invasive: rapid urease test (RUT), histology, culture from endoscopic biopsy
- Autoimmune gastritis: serum anti-parietal cell antibodies, anti-intrinsic factor antibodies, low vitamin B12, elevated gastrin, low pepsinogen I
- Imaging (CT/plain films): useful in emphysematous gastritis (gas in gastric wall, portal venous gas)
- Sleisenger & Fordtran's, p. 909; Tietz Textbook of Laboratory Medicine
Management
H. pylori Eradication
Eradication is the cornerstone of treatment for H. pylori gastritis, PUD, and MALToma. Eradication rates of up to 90% are achievable. Reinfection is uncommon (<0.5%). - Bailey & Love's, p. 1177
Standard regimens:
- Triple therapy (7-14 days): PPI + clarithromycin + amoxicillin (or metronidazole)
- Bismuth quadruple therapy: PPI + bismuth + metronidazole + tetracycline (preferred where clarithromycin resistance is high)
- Concomitant / sequential therapy in areas of high resistance
- Confirm eradication with UBT or stool antigen test ≥4 weeks after completing therapy
Acid Suppression
- PPIs (omeprazole, pantoprazole, etc.): mainstay for symptom relief and mucosal healing
- H2-receptor antagonists (ranitidine, famotidine): second-line
NSAID-Induced Gastritis
- Discontinue or minimize NSAID use
- PPI co-prescription when NSAIDs cannot be stopped
- Switch to COX-2 selective inhibitor (lower GI risk)
Autoimmune Atrophic Gastritis
- Lifelong vitamin B12 supplementation (IM or oral)
- Monitor for pernicious anaemia, iron deficiency
- Endoscopic surveillance for gastric dysplasia/cancer
Phlegmonous/Emphysematous Gastritis
- Broad-spectrum IV antibiotics
- Surgical intervention if necrosis, perforation, or failure to respond to antibiotics
- Supportive ICU care for septic patients
Recent Evidence
- A 2024 systematic review and meta-analysis (PMID: 39575409) on H. pylori prevalence in China (2014-2023) highlights the ongoing high burden of infection, particularly important given gastric cancer rates.
- A 2025 meta-analysis (PMID: 40822578) examines interactions between H. pylori and the gut microbiome, suggesting microbiome disruption may contribute to clinical outcomes beyond the stomach itself.
- A 2025 systematic review (PMID: 40532847) on emphysematous gastritis provides updated characterization of this rare but potentially fatal form.
Sources: Robbins & Cotran Pathologic Basis of Disease | Harrison's Principles of Internal Medicine 22E (2025) | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Bailey & Love's Short Practice of Surgery 28th Ed. | Tietz Textbook of Laboratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.