Clostridium tetani
Reading File
Finding Sources
Searching the Web
Clostridium tetani microbiology pathogenesis tetanospasmin mechanism
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Here is a full, integrated overview of Clostridium tetani drawn from multiple authoritative medical microbiology textbooks.
Clostridium tetani
Microbiology and Structure
Clostridium tetani is a large (0.5-2 × 2-18 µm), gram-positive, motile, obligately anaerobic, spore-forming rod. The key morphological feature is its terminal, round spore, which gives the organism a classic "drumstick" or "tennis racket" appearance on microscopy. The vegetative cells are extremely oxygen-sensitive, which makes culture difficult; on agar it grows as a spreading film rather than discrete colonies. The bacteria are proteolytic but unable to ferment carbohydrates.
- Medical Microbiology 9e, p. 349
- Quick Compendium of Clinical Pathology 5e
Epidemiology
-
Spores are ubiquitous in soil and in the feces of horses and other animals; they survive in adverse conditions for very long periods.
-
C. tetani transiently colonizes the GI tracts of humans and animals without causing disease.
-
Disease is rare in vaccinated populations (only ~33 cases in the US in 2017), but remains a major cause of death in developing countries, with an estimated >1 million cases worldwide and mortality rates of 30-50%.
-
At least half of all tetanus deaths occur in neonates.
-
Risk is greatest in people with inadequate vaccine-induced immunity; importantly, natural infection does not confer immunity.
-
Medical Microbiology 9e, p. 350
Toxins
C. tetani produces two toxins:
| Toxin | Properties | Significance |
|---|---|---|
| Tetanospasmin | Plasmid-encoded, heat-labile, 150-kDa neurotoxin (A-B type) | Primary virulence factor; causes tetanus |
| Tetanolysin | Oxygen-labile hemolysin, serologically related to streptolysin O | Clinical significance unknown; inhibited by oxygen and serum cholesterol |
The plasmid carrying the tetanospasmin gene is non-conjugative, so a non-toxigenic strain cannot acquire it horizontally.
Mechanism of Action of Tetanospasmin
This is one of the most potent toxins known - extremely small amounts can be lethal.
-
Synthesis: Tetanospasmin is produced during the stationary phase of bacterial growth and released upon cell lysis. The single 150-kDa peptide is cleaved by an endogenous protease into:
- Heavy chain (100 kDa, B subunit) - binding and translocation
- Light chain (50 kDa, A subunit) - enzymatic activity The two chains are held together by a disulfide bond.
-
Binding: The carboxyl-terminal domain of the heavy chain binds polysialoganglioside (sialic acid) receptors and adjacent glycoproteins on the surface of lower motor neurons at the neuromuscular junction.
-
Internalization and retrograde transport: The toxin is internalized in endosomal vesicles and transported retrograde along motor neuron axons to the motor neuron soma in the spinal cord and brainstem.
-
Transcytosis: The toxin then undergoes trans-synaptic spread to the presynaptic terminals of inhibitory interneurons (both glycinergic and GABAergic).
-
Cleavage of synaptobrevin (VAMP2): Within the inhibitory neuron, endosomal acidification causes a conformational change in the heavy chain N-terminus that inserts into the membrane, releasing the light chain into the cytosol. The light chain is a zinc endopeptidase that cleaves synaptobrevin (VAMP2), a SNARE protein required for docking of neurotransmitter vesicles onto the presynaptic membrane.
-
Result: Release of the inhibitory neurotransmitters glycine and GABA is blocked. Motor neurons lose inhibition, causing unregulated excitatory activity → spastic paralysis and uncontrolled muscle spasms.
The toxin binding is irreversible - recovery depends on the formation of new axonal terminals.
- Medical Microbiology 9e, pp. 350-351
- Jawetz, Melnick & Adelberg's Medical Microbiology 28e, p. 194
Contrast with botulinum toxin: Botulinum toxin acts at the same SNARE machinery but stays at the neuromuscular junction and blocks acetylcholine release, causing flaccid paralysis - the opposite effect.
Pathogenesis
C. tetani is non-invasive. Infection remains strictly localized in devitalized tissue (wound, burn, umbilical stump). The organism requires a low oxidation-reduction potential (anaerobic environment), facilitated by:
- Necrotic tissue
- Calcium salts
- Associated pyogenic infections
Disease is almost entirely a toxemia - the volume of infected tissue is small, but the toxin spreads via the bloodstream and nervous system.
Clinical Forms of Tetanus
1. Generalized Tetanus (most common)
- Incubation: Days to weeks; shorter incubation = worse prognosis
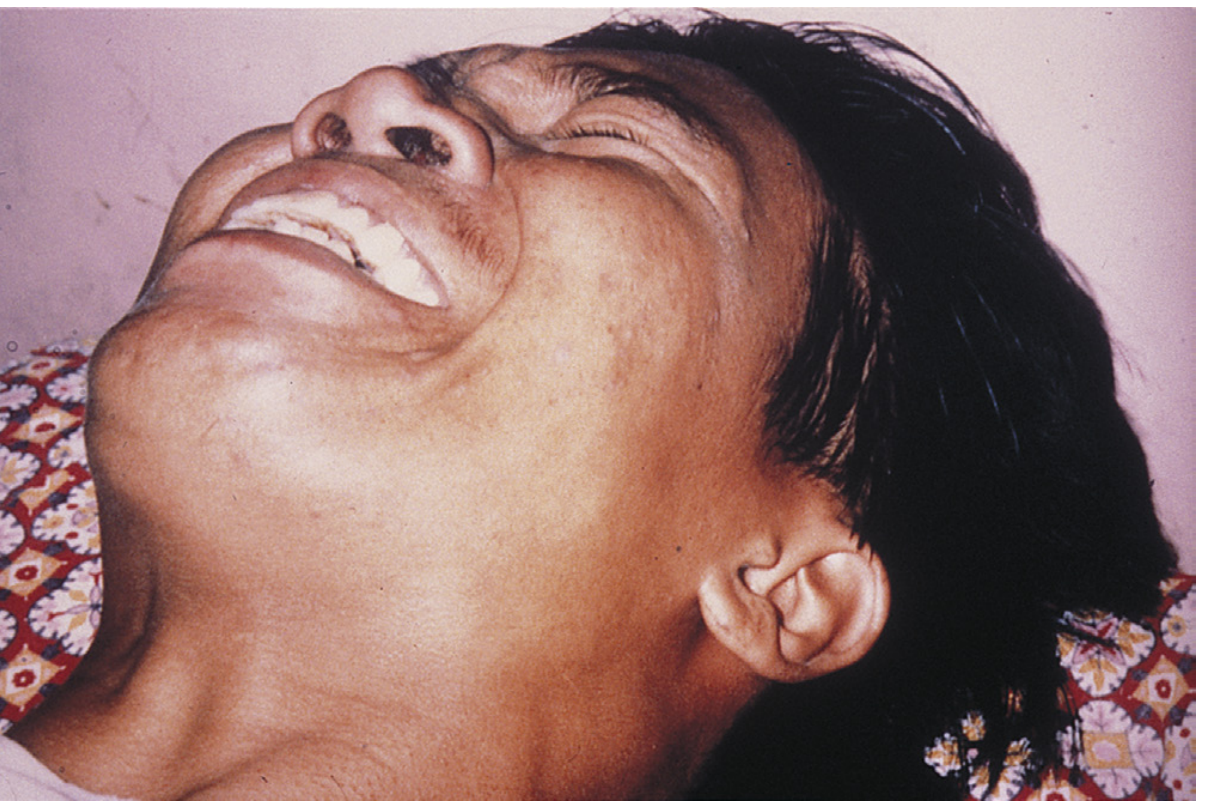
- Progression: Trismus (lockjaw, masseter spasm) is the most common presenting sign → risus sardonicus (sardonic smile from sustained facial muscle contraction) → opisthotonos (persistent spasms of the back muscles)
- Any external stimulus can precipitate generalized tetanic spasm
- Autonomic involvement in severe disease: cardiac arrhythmias, fluctuating blood pressure, profound sweating, dehydration
- Patient remains fully conscious; pain can be intense
- Death is typically from respiratory failure

2. Localized Tetanus
- Muscle rigidity confined to the site of primary infection
- Generally better prognosis
3. Cephalic Tetanus
- Primary infection site is the head (e.g., ear infection, facial wound)
- Involves short cranial motor nerves; very poor prognosis
4. Neonatal Tetanus (Tetanus neonatorum)
- Entry via infected umbilical stump (unsterile cord cutting in developing countries)
- Progresses to generalized tetanus
- Mortality >90%; developmental defects in survivors
- Almost exclusively a disease of developing countries
Diagnosis
Diagnosis is clinical - there is no reliable laboratory test.
- Microscopy and culture are insensitive (culture positive in only ~30% of cases)
- Tetanus toxin is not detectable in blood (it binds irreversibly to neurons)
- Antibodies to the toxin are also typically absent
- Differential diagnosis: strychnine poisoning (also blocks glycine receptors, clinically identical)
- Confirmatory test (reference labs only): mouse toxin neutralization assay
Treatment
Treatment must begin promptly - antitoxin is only effective before the toxin binds to nerve tissue.
| Component | Agent | Purpose |
|---|---|---|
| Wound care | Debridement | Remove source of toxin production |
| Antibiotics | Penicillin or metronidazole (preferred) | Kill bacteria, reduce toxin production |
| Passive immunization | Human Tetanus Immunoglobulin (HTIG) 250-500 units IM | Neutralize unbound circulating toxin |
| Active immunization | Tetanus toxoid | Infection does NOT confer immunity |
| Muscle relaxants | Benzodiazepines | Control spasms |
| Supportive | Mechanical ventilation | Manage respiratory failure |
Why prefer metronidazole over penicillin? Penicillin is a GABA antagonist, similar in mechanism to tetanus toxin itself, potentially worsening CNS excitability. Metronidazole avoids this issue and has equivalent antimicrobial activity.
Prevention
- Primary series: 3 doses of tetanus toxoid (as part of DTaP or Td)
- Booster: Every 10 years
- Vaccination is highly effective and the most important preventive measure
- For wound prophylaxis in unvaccinated or incompletely vaccinated individuals: both toxoid and HTIG may be given simultaneously
Summary Table
| Feature | Detail |
|---|---|
| Organism | Gram-positive, anaerobic, spore-forming rod |
| Spore | Terminal, round - "drumstick" / "tennis racket" |
| Toxin | Tetanospasmin (plasmid-encoded, 150 kDa, A-B toxin) |
| Toxin target | VAMP2/synaptobrevin on inhibitory interneurons |
| Neurotransmitters blocked | Glycine + GABA |
| Result | Spastic paralysis |
| Key clinical sign | Trismus → risus sardonicus → opisthotonos |
| Diagnosis | Clinical only |
| Treatment | HTIG + wound debridement + metronidazole + toxoid + benzodiazepines |
| Prevention | DTaP series + 10-year boosters |
Sources: Medical Microbiology 9e (Murray); Jawetz, Melnick & Adelberg's Medical Microbiology 28e; Quick Compendium of Clinical Pathology 5e; Bailey & Love's Surgery 28e; Rosen's Emergency Medicine.
Make FMGE EXAM QUESTION 2026 , 150 QUESTION INCLUDING BIOCHEMISTRY, PHARMACOLOGY,PHYSIOLOGY . WITH EXPLANATION
Asking for Preferences
Reading File
Running Command
mkdir -p /home/daytona/workspace/fmge-2026 && ls /home/daytona/workspace/fmge-2026/
Make FMGE EXAM QUESTION 2026 , 150 QUESTION INCLUDING BIOCHEMISTRY, PHARMACOLOGY,PHYSIOLOGY . WITH EXPLANATION
This is a shared conversation. Sign in to Orris to start your own chat.