upper gi bleed
Reading File
Finding Sources
Searching PubMed
"upper gastrointestinal bleeding" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive content to compile a thorough answer. Here is the full clinical overview:
Upper Gastrointestinal Bleeding (UGIB)
Definition: UGIB is any GI bleeding originating proximal to the ligament of Treitz - encompassing esophageal, gastric, and duodenal sources.

Epidemiology
- Annual incidence: 39-172 per 100,000 in Western countries (varies with H. pylori rates, NSAID use, socioeconomics)
- Overall mortality: 5-10% - unchanged since the 1970s despite advances, largely because more patients are elderly with comorbidities
- Bleeding is self-limited in ~80% without specific therapy; of the remaining 20% who rebleed, mortality rises to 30-40%
Causes (by frequency)
| Cause | Frequency |
|---|---|
| Peptic ulcer (gastric/duodenal) | ~35-40% |
| Esophageal/gastric varices | ~22% |
| Portal hypertension-related lesions | ~5% |
| Esophagitis | ~5% |
| Angioectasia / telangiectasia | ~4% |
| Mallory-Weiss tear | ~4% |
| Dieulafoy lesion | ~3% |
| GI tract neoplasm | ~3% |
| Epistaxis (swallowed blood) | ~2% |
| Erosive gastritis/duodenitis | ~1% |
| No cause found | ~7% |
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease, UCLA CURE Database, n=968)
Key Causes - Clinical Notes
Peptic Ulcer Disease - Most common cause. Associated with H. pylori, NSAIDs, aspirin, and smoking. Bleeding arteries in ulcer bases have a mean diameter of 0.7 mm. ~50% show a protruding vessel, ~50% have an adherent clot over a breached artery wall.
Esophageal/Gastric Varices - Result from portal hypertension, most often from alcoholic cirrhosis in the US. In cirrhotics presenting with UGIB, varices are the cause 59% of the time. In-hospital mortality in cirrhotic patients is essentially double that of non-cirrhotics.
Mallory-Weiss Tear - Longitudinal mucosal tear at the gastroesophageal junction from forceful retching/vomiting. Classic presentation: hematemesis following an episode of heavy retching (alcohol, DKA, chemotherapy). Usually self-limited.
Dieulafoy Lesion - Abnormally large submucosal artery that protrudes through mucosa without primary ulceration. 80-95% located within 6 cm of the GEJ along the lesser curvature of the stomach. Can cause massive, recurrent, unexplained hemorrhage.
Erosive Gastritis/Esophagitis - Common triggers: alcohol, aspirin, NSAIDs, radiation, stress (sepsis, mechanical ventilation). Infectious causes include CMV, HSV, Candida (especially in immunocompromised).
Presentation
| Presentation | Significance |
|---|---|
| Hematemesis (bright red) | Active, brisk bleeding |
| Coffee-ground emesis | Slower/stopped bleeding |
| Melena (black, tarry stool) | As little as 50-100 mL blood from upper GI |
| Hematochezia | Massive UGIB (>1000 mL) - mimics lower GI bleed |
Useful clue: Digested blood is a source of urea - an elevated BUN:creatinine ratio (>20:1) strongly suggests UGIB. Confirm with nasogastric lavage (red blood or coffee-ground aspirate).
Risk Stratification
Pre-Endoscopy Scoring Tools
Glasgow-Blatchford Score (GBS) - Uses: BUN, hemoglobin, systolic BP, HR, syncope, melena, liver disease, heart failure. Best for identifying patients who need clinical intervention. A GBS of 0-1 identifies very low-risk patients who can be managed outpatient.
AIMS65 Score - Five variables:
- Albumin < 3.0 g/dL
- INR > 1.5
- Altered mental status
- Systolic BP < 90 mmHg
- Age > 65
Score < 2 = lower risk of mortality and shorter hospital stay.
Clinical Rockall Score (pre-endoscopy) - Age, shock, comorbidities.
High-Risk Features
| Very Low Risk | High Risk |
|---|---|
| Age < 60 | Advanced age |
| No major comorbidities | Significant comorbidities |
| No red hematemesis | Red hematemesis |
| Hemodynamically stable | Hemodynamically unstable |
| Normal labs | Abnormal labs (low Hgb, elevated INR, elevated BUN) |
| Negative NG aspirate | Red blood on NG aspirate |
(Tintinalli's Emergency Medicine)
Initial Management
Resuscitation (ABC First)
- Two large-bore IVs; type & crossmatch
- Massive transfusion protocol (MTP) if large blood product need anticipated
- Transfusion threshold: Hgb ≤ 7 g/dL in most patients; ≤ 9 g/dL in elderly or those with comorbidities (e.g., coronary artery disease)
- Correct coagulopathy if INR elevated or platelets < 50,000
- Airway: intubation of hemodynamically unstable UGIB patients is high-risk - aggressively resuscitate before intubation, use reduced induction agent doses
Medical Therapy
| Drug | Dose | Indication |
|---|---|---|
| Omeprazole (PPI) | 80 mg IV bolus, then 8 mg/h infusion | Peptic ulcer bleeding |
| Octreotide | 50 mcg IV bolus, then 25-50 mcg/h infusion | Variceal bleeding |
| Antibiotics (ciprofloxacin 400 mg IV or ceftriaxone 1 g IV) | Standard dosing | Cirrhosis with UGIB (reduces bacterial translocation, mortality) |
| Tranexamic acid | Controversial - recent meta-analysis shows no clear benefit in UGIB |
High-dose PPI after endoscopic hemostasis reduces rebleeding risk for peptic ulcer; effect lasts 72 hours (main rebleeding risk period).
Endoscopy
Timing: Upper endoscopy (EGD) within 24 hours after adequate resuscitation for most patients with overt UGIB. Urgent endoscopy (< 12 hours) for actively unstable patients.
Forrest Classification (Peptic Ulcer Stigmata)
| Class | Finding | Rebleeding Risk (untreated) | Endoscopic Tx Needed? |
|---|---|---|---|
| Ia | Active spurting | ~90% | Yes |
| Ib | Active oozing | ~10-20% | Yes (if other stigmata) |
| IIa | Non-bleeding visible vessel (NBVV) | ~50% | Yes |
| IIb | Adherent clot | ~33% | Yes (clot removal + treat) |
| IIc | Flat pigmented spot | ~5-10% | No |
| III | Clean base | ~1-2% | No |
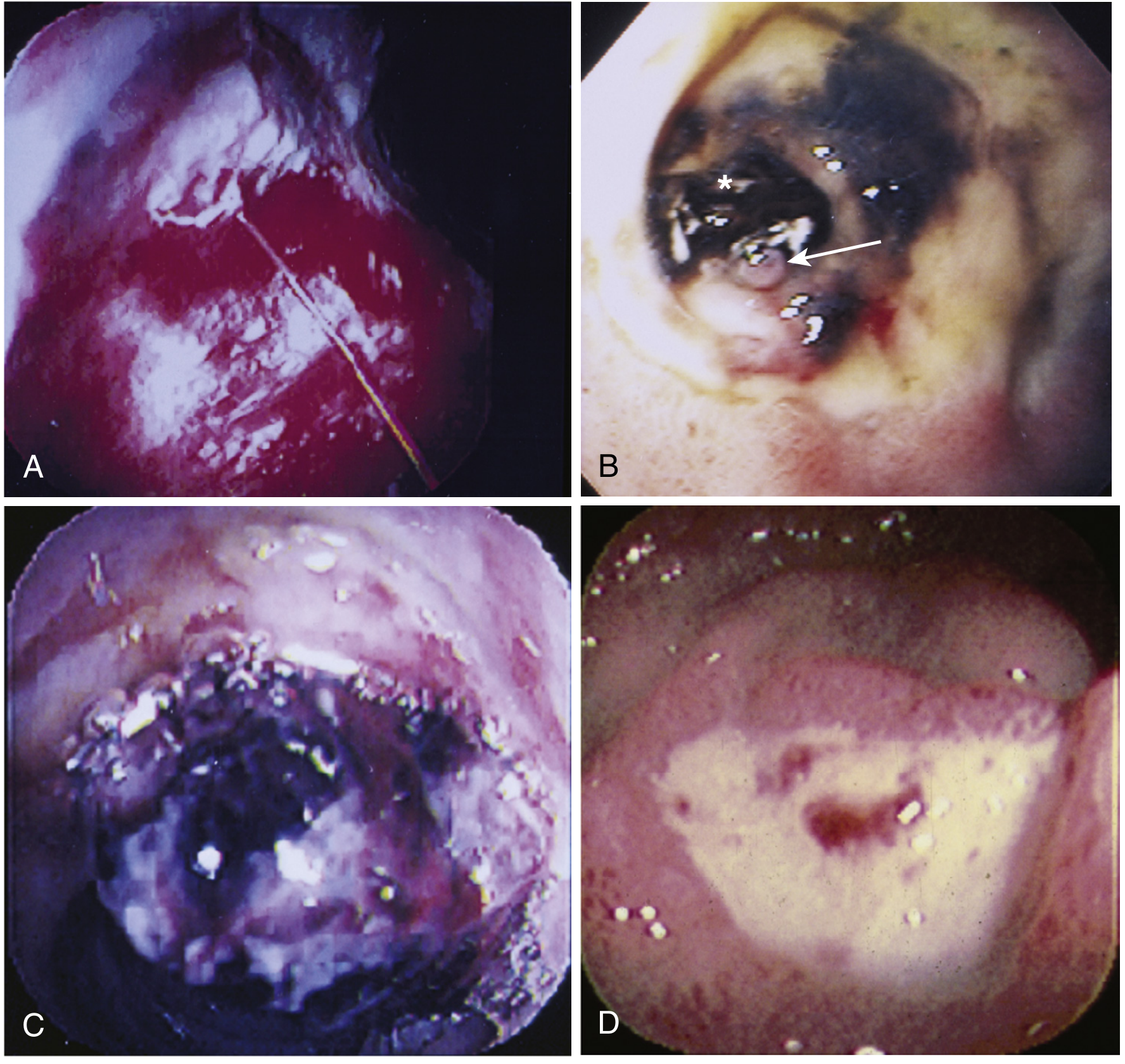
Endoscopic stigmata of recent peptic ulcer hemorrhage - Sleisenger & Fordtran's
Endoscopic Hemostasis Techniques
- Injection therapy: Epinephrine (1:20,000) in 4 quadrants around bleeding site (0.5-1 mL aliquots)
- Thermal/contact coagulation: Multipolar electrocoagulation probe (10 Fr), thermocoagulation - firm pressure, low power (12-15 W), 10-second pulses
- Mechanical: Hemoclips placed across vessel/NBVV; over-the-scope clips (OTSC) for refractory cases
- Non-contact: Argon plasma coagulation (APC), laser
- Combination therapy (injection + thermal or clips) reduces rebleeding to ~15% vs. ~30% with monotherapy alone
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease)
Variceal Bleeding - Special Management
- Octreotide infusion (reduces portal pressure) - start immediately
- Antibiotics mandatory in all cirrhotics with UGIB (ciprofloxacin or ceftriaxone) - proven to reduce mortality
- Endoscopic variceal band ligation (EVL) - treatment of choice for esophageal varices
- Sclerotherapy - alternative
- Balloon tamponade (Sengstaken-Blakemore or Minnesota tube) - temporary bridge in refractory hemorrhage
- TIPS (Transjugular Intrahepatic Portosystemic Shunt) - for refractory variceal bleeding unresponsive to endoscopic + pharmacologic therapy
- Beta-blocker prophylaxis (propranolol/nadolol) + EVL for secondary prevention
When Endoscopy Fails - Salvage Options
- Repeat endoscopy - for recurrent bleeding after initial hemostasis
- Angiography with transcatheter arterial embolization (TAE) - for high surgical risk patients
- Surgery - oversewing of ulcer base, antrectomy, or gastrectomy. Reserved for those failing endoscopic/angiographic therapy
Recent Evidence (2024-2026)
- Tranexamic acid (TXA): A 2025 meta-analysis (PMID 40029534) found no clear benefit for TXA in acute GI bleeding - not currently recommended as routine adjunct
- Over-the-scope clips (OTSC): A 2025 systematic review/meta-analysis (PMID 39500365) shows OTSCs are superior to standard clips for refractory or recurrent nonvariceal UGIB, particularly for Forrest Ia/IIa lesions in fibrotic ulcer beds
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease (9780323609623) | Tintinalli's Emergency Medicine (9781260019933) | Frameworks for Internal Medicine (9781496359308) | PubMed 40029534, 39500365
This is a shared conversation. Sign in to Orris to start your own chat.