Anatomy and physiology of anal canal General surgery perspective
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple surgical textbooks. Let me compile the complete answer.
Anatomy and Physiology of the Anal Canal - A Surgical Perspective
1. Overview and Boundaries
The anal canal is the terminal segment of the gastrointestinal tract. Surgically, it extends from the anorectal ring (a palpable ridge formed by the convergence of the puborectalis muscle, deep external sphincter, and internal sphincter) to the anal verge (junction with hair-bearing perineal skin). It measures 3-4 cm in adults, and is consistently longer in males than females.
Relations:
- Posterior: Anococcygeal ligament separates it from the coccyx
- Anterior: Perineal body separates it from the membranous urethra/penile bulb (male) or lower vagina (female)
- Lateral: Ischiorectal fossae on both sides
Anatomical vs. Surgical anal canal: The anatomical canal starts at the dentate line; the surgical canal starts at the anorectal ring - a distinction important in cancer staging and surgery.
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 1438
2. Muscular Wall - The Sphincter Complex
Here is the classic coronal cross-section anatomy of the anal canal:
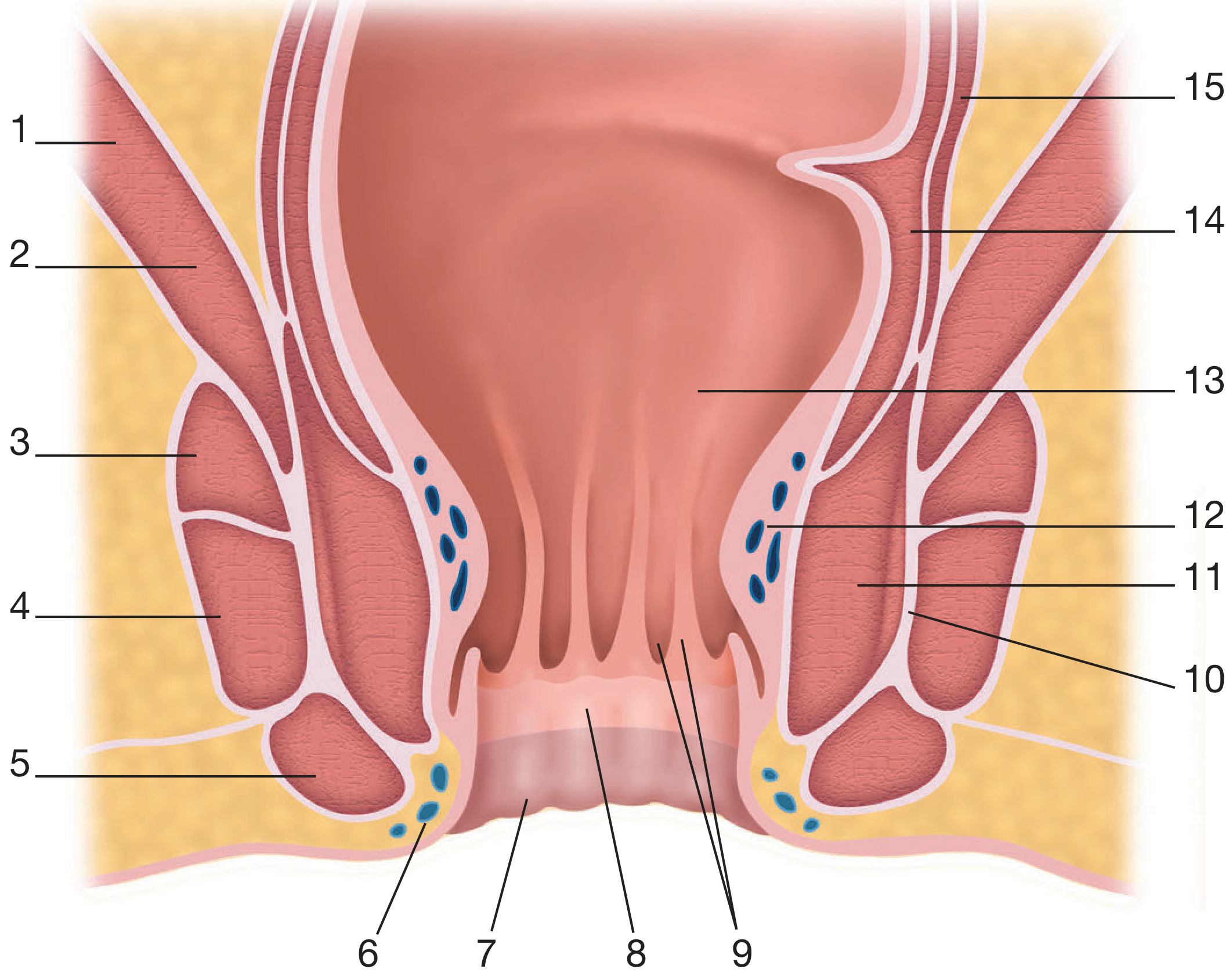
Key: 1-Levator ani (iliococcygeus), 2-Levator ani (puborectalis), 3-5 External anal sphincter (deep, superficial, subcutaneous), 6-Inferior haemorrhoidal plexus, 7-Perianal skin, 9-Anal columns and crypts, 10-Conjoined longitudinal muscle, 11-Internal anal sphincter, 12-Superior haemorrhoidal plexus, 13-Anorectal junction, 14-Circular rectal muscle, 15-Longitudinal rectal muscle
A. Internal Anal Sphincter (IAS)
- Thickened (2-5 mm) distal continuation of the circular muscle layer of the rectum
- Involuntary smooth muscle - pearly-white when exposed at operation
- Begins where rectum passes through pelvic diaphragm; its lower border is palpable as the intersphincteric groove
- Innervation: Autonomic (intrinsic non-adrenergic, non-cholinergic fibres releasing nitric oxide cause relaxation)
- Provides ~85% of resting anal canal tone (key for passive continence)
B. External Anal Sphincter (EAS)
- Forms the bulk of the sphincter complex; surrounds the IAS
- Voluntary striated muscle - red in colour
- Though classically subdivided into deep, superficial, and subcutaneous portions (Milligan-Morgan), it is functionally a single muscle (Goligher) variably divided by extensions from the longitudinal muscle
- Some fibres attach to the coccyx posteriorly; anteriorly they fuse with perineal muscles
- Innervation: Pudendal nerve (S2, S3, S4) - somatic voluntary control
- Provides active/squeeze continence
C. Puborectalis Muscle
- Part of the levator ani; forms a U-shaped sling around the anorectal junction
- Maintains the anorectal angle (~90°) - the most important single factor in continence
- Nerve supply: Sacral somatic nerves (S3, S4)
D. Longitudinal Muscle
-
Direct continuation of the outer longitudinal smooth muscle of the rectum, augmented by striated fibres from the pelvic floor
-
Passes between the external and internal sphincters (forming the intersphincteric plane)
-
Splits into multiple terminal septa inserting into skin of the lowermost anal canal and perianal skin
-
The most medial septa = anal intermuscular septum
-
Function during defecation: Contracts to widen the anal lumen, flatten anal cushions, shorten the canal, and evert the anal margin; subsequent relaxation helps restore the airtight seal
-
Bailey and Love's Short Practice of Surgery 28th Edition, p. 1439
3. The Intersphincteric Plane
Between the external sphincter laterally and the longitudinal muscle medially lies the intersphincteric plane - surgically important because:
- It houses the intersphincteric anal glands (the source of cryptoglandular abscesses/fistulae)
- It is a route for the spread of infection along longitudinal muscle extensions
- It can be surgically explored to access sphincter muscles (key in LIFT procedure for fistula-in-ano)
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 1439
4. Lining of the Anal Canal (Epithelium)
| Zone | Lining | Location | Significance |
|---|---|---|---|
| Upper anal canal | Columnar epithelium (rectal) | Above anorectal ring | Autonomic supply; no pain sensation |
| Transitional/ATZ | Cuboidal transitional epithelium | 1-2 cm proximal to dentate line | Contains 8-12 vertical columns of Morgagni |
| Dentate line | Serrated junction of columns + crypts | ~2 cm above anal verge | Embryological endo-ectoderm junction |
| Anoderm | Non-keratinised stratified squamous | Dentate line to anal verge | No hair/glands; richly innervated somatic sensory endings |
| Anal verge | Keratinised squamous skin | External | Hair-bearing |
The dentate line (pectinate line) is the single most important landmark in anal surgery - it determines:
-
Type of epithelium (and cancer histology)
-
Nerve supply (somatic below vs. autonomic above)
-
Venous and lymphatic drainage
-
Sensation (sharp pain felt only below the dentate line)
-
Mulholland and Greenfield's Surgery, p. 3534
5. The Anal Crypts and Glands
-
Between the bases of the columns of Morgagni lie 6-14 anal crypts (of Morgagni)
-
Each crypt contains openings of anal glands (4-8 glands total, some penetrate into the intersphincteric space)
-
When compressed by stool passage, glands exude secretions lubricating passage
-
Surgical significance: Blocked/infected anal glands → cryptoglandular infection → perianal abscess → fistula-in-ano (Parks' cryptoglandular theory)
-
Mulholland and Greenfield's Surgery, p. 3534
6. Anorectal Spaces (Surgical Importance)
These myofascial potential spaces are critical for understanding abscess spread patterns:
| Space | Location | Contents | Abscess significance |
|---|---|---|---|
| Perianal space | Subcutaneous around anus | External haemorrhoids, subcutaneous EAS, distal IAS | Perianal abscess (most common) |
| Intersphincteric space | Between IAS and EAS | Anal glands, longitudinal muscle | Intersphincteric abscess; primary site of cryptoglandular infection |
| Ischioanal/Ischiorectal space | Between ischial tuberosity laterally and sphincters medially; from skin to levator ani | Fat, inferior rectal vessels and nerves | Ischiorectal abscess (large) |
| Postanal/deep postanal space | Posterior to anus, between anococcygeal ligament and levator ani | Connects both ischiorectal spaces | Route of horseshoe abscess formation |
| Supraelevator/Pelvirectal space | Above levator ani | Pelvic organs | Supralevator abscess (rare, high, complex) |
Horseshoe abscess: Infection begins in the deep postanal space (posterior midline intersphincteric gland) and extends laterally into both ischiorectal spaces - the anococcygeal ligament prevents distal spread, forcing lateral extension.
- Mulholland and Greenfield's Surgery, p. 3535
7. Blood Supply
Arterial:
- Superior rectal artery - terminal branch of inferior mesenteric artery; supplies upper anal canal; runs posterior to the rectum and bifurcates to supply the anal submucosa (branches not constant - Thomson)
- Middle rectal arteries - branches of internal iliac
- Inferior rectal arteries - branches of internal pudendal artery; supply the sphincter complex and lower anal canal
Venous drainage:
- Upper half: Superior rectal veins → inferior mesenteric vein (portal system); middle rectal veins → internal iliac veins
- Lower half: Inferior rectal veins → internal pudendal veins → internal iliac veins (systemic)
- Portosystemic anastomosis at the dentate line; direct arteriovenous communications exist in the submucosal vascular plexuses (explains bright red colour of haemorrhoidal bleeding)
Anal cushions (at 3, 7, 11 o'clock positions): Vascular sinusoids supported by fibroelastic connective tissue and smooth muscle - contribute to the airtight anal seal. These are NOT varicosities.
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 1440
8. Lymphatic Drainage
| Level | Drainage pathway | Nodes |
|---|---|---|
| Above dentate line | Upward with superior rectal vessels | Pararectal → inferior mesenteric nodes → para-aortic; also laterally via middle/inferior rectal vessels to internal iliac nodes |
| Below dentate line | Downward and lateral | Superficial → deep inguinal lymph nodes |
| Anal transition zone (ATZ) | Both routes possible | Both inguinal AND pelvic nodal basins |
Surgical significance: Unexplained inguinal lymphadenopathy should prompt careful anal canal examination. Lower anal canal SCCs can present with inguinal nodal metastases.
- Maingot's Abdominal Operations, p. 899
9. Nerve Supply
| Structure | Innervation | Type | Significance |
|---|---|---|---|
| IAS | Autonomic (sympathetic L1-L2, parasympathetic S2-S4) | Involuntary | Reflex relaxation on rectal distension (RAIR) |
| EAS | Pudendal nerve (S2, S3, S4) | Somatic, voluntary | Squeeze continence, urge suppression |
| Puborectalis | Sacral somatic nerves (S3, S4) | Somatic | Anorectal angle maintenance |
| Below dentate line | Inferior rectal branch of pudendal nerve | Somatic sensory | Pain, temperature, touch - explains pain in fissure/haemorrhoidectomy |
| Above dentate line | Autonomic fibres | Autonomic | Only stretch-sensitive - no sharp pain |
Clinical pearl: Injections or procedures above the dentate line are relatively painless (e.g., rubber band ligation of internal haemorrhoids). Below the dentate line, anything causes sharp pain - hence local anaesthesia is required for fissurectomy and operations on the anoderm.
10. Physiology - Continence Mechanism
Faecal continence is maintained by multiple complementary mechanisms:
- Anorectal angle (~90°): Maintained by puborectalis sling - the single most important factor (Parks)
- Internal sphincter: Provides ~85% of resting anal canal pressure; continuously tonically contracted
- External sphincter: Voluntary squeeze; provides active/urge continence
- Anal cushions: Vascular submucosal cushions that provide a fine airtight seal
- Rectal capacity and compliance: Acts as a reservoir - allows accommodation of stool
- Rectoanal inhibitory reflex (RAIR): Rectal distension → IAS relaxes (sampling reflex) → anoderm "samples" contents → conscious decision to defecate or retain
Defecation: Involves rectal contraction, puborectalis relaxation (straightening anorectal angle), EAS relaxation, and longitudinal muscle contraction (widens lumen, shortens canal). After defecation, EAS and IAS contract to restore continence.
Summary Box (Bailey & Love)
| Feature | Internal Sphincter | External Sphincter |
|---|---|---|
| Muscle type | Smooth (involuntary) | Striated (voluntary) |
| Innervation | Autonomic | Pudendal nerve |
| Colour at surgery | Pearly white | Red |
| Primary role | Resting tone (85%) | Active squeeze |
| Thickness | 2-5 mm | Variable |
Key surgical principles:
- The anorectal ring must never be completely divided (causes incontinence)
- Lymphatics above the dentate line drain to mesorectal and pelvic nodes; below to inguinal nodes
- The intersphincteric plane is the key surgical plane for fistula surgery
- Cryptoglandular infection is the origin of nearly all perianal abscesses and fistulae
Sources: Bailey and Love's Short Practice of Surgery, 28th Edition | Mulholland and Greenfield's Surgery, 7th Edition | Maingot's Abdominal Operations
This is a shared conversation. Sign in to Orris to start your own chat.