analyse_media
Reading File
Searching PubMed
ventricular tachycardia wide complex ECG diagnosis criteria
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is a full ECG interpretation and clinical analysis.
ECG Report - Mr. Yogendra K. Verma, 52M, ICU-2
Date/Time: 04-07-2026, 01:24:36
Settings: 25 mm/s, 20 mm/mV (double standard sensitivity - all amplitudes appear twice as tall as on a standard 10 mm/mV tracing)
Automated Measurements
| Parameter | Value |
|---|---|
| Heart Rate | 153 bpm |
| P wave duration | 79 ms |
| PR (PQ) interval | 67 ms (likely spurious - see below) |
| QRS duration | 138 ms (broad) |
| QT / QTcHOD | 327 / 489 ms (prolonged) |
| P/QRS/T Axis | -123° / 117° / 46° |
| RV5 / SV1 | 0.695 / 0.278 mV |
| RV5+SV1 | 0.973 mV |
Primary Diagnosis: Ventricular Tachycardia (VT)
This ECG shows a regular wide-complex tachycardia at 153 bpm that fulfills multiple criteria for VT.
Brugada Criteria Applied (Step-by-Step)
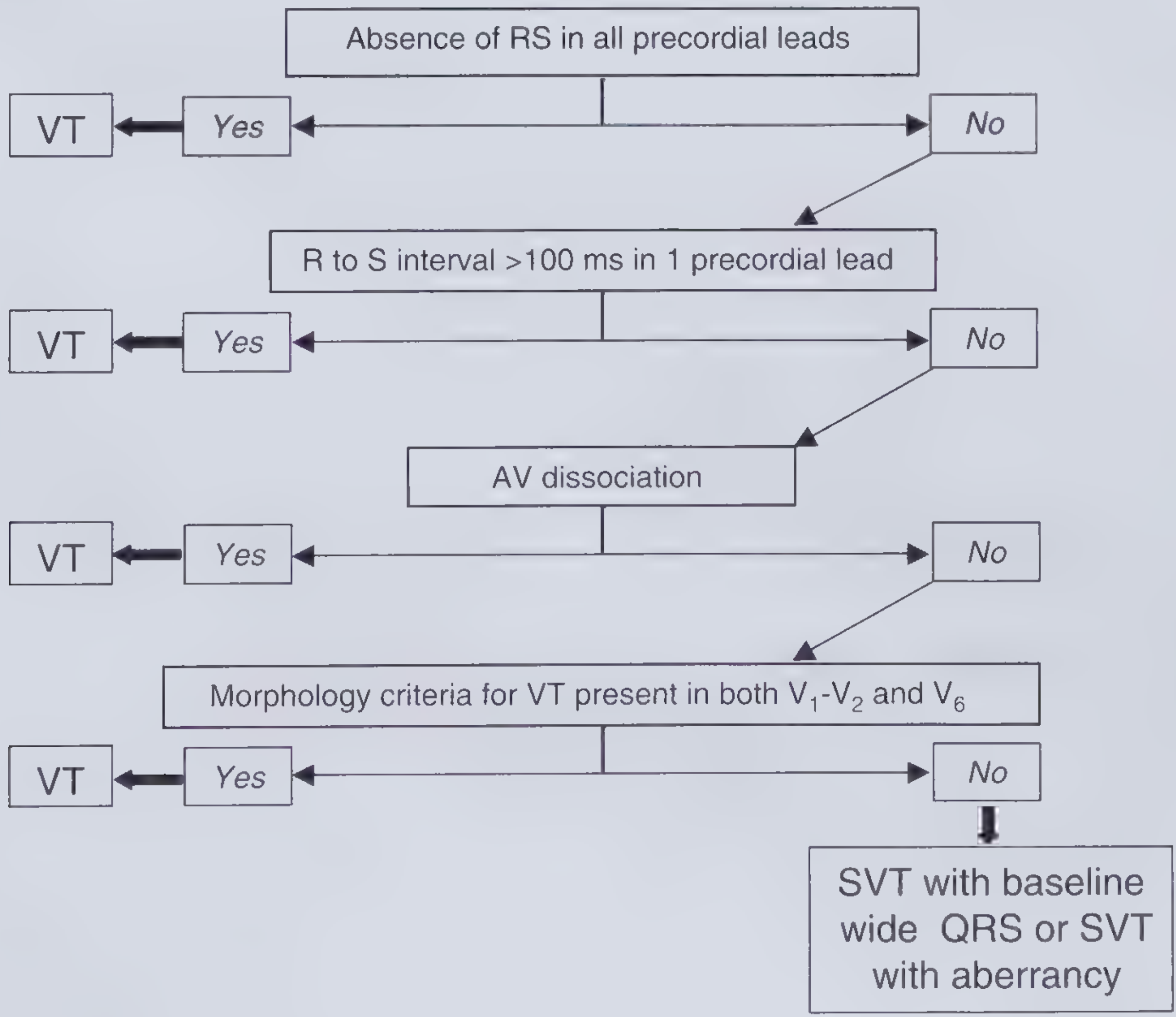
Step 1 - Absence of RS complex in ALL precordial leads?
- V1-V3: QS pattern (no S wave, so no RS)
- V4-V9: Monophasic tall R waves with no S wave
- YES - No RS complex in any precordial lead → DIAGNOSIS: VT (criterion met at Step 1; further steps not required)
Even proceeding further for completeness:
Step 2 - R-to-S interval >100 ms in any precordial lead?
- The QRS is 138 ms throughout - highly likely YES
Step 3 - AV dissociation?
- The PR interval of 67 ms is implausibly short for a conducted sinus beat - this is almost certainly a machine artifact from misidentifying noise as a P wave
- True independent P waves cannot be confirmed due to heavy baseline artifact, but the very short "PR" strongly suggests no true AV conduction → AV dissociation likely present
Step 4 - VT morphology criteria?
- V1: QS pattern (a classic VT morphology criterion)
- V6: Monophasic tall R wave without a Q wave
All four Brugada steps favor VT.
Key ECG Features Supporting VT
| Feature | Finding | Significance |
|---|---|---|
| QRS width | 138 ms | Ventricular origin (>120 ms) |
| Rate | 153 bpm | Sustained tachycardia |
| QRS axis | +117° (right axis) | Extreme/northwest axis supports VT |
| P/QRS axis discordance | P axis -123°, QRS axis +117° | Near-opposite axes - AV dissociation |
| V1-V3 morphology | QS / deep rS (no RS) | Absence of RS = VT criterion |
| V4-V9 morphology | Monophasic, tall concordant R waves | Positive concordance across precordials |
| Precordial concordance | All V leads positive (V4-V9) | Strongly favors VT; extremely rare in SVT with aberrancy |
| QTc | 489 ms (prolonged) | Secondary to wide QRS |
Positive Precordial Concordance
The transition from QS complexes in V1-V3 to uniformly tall positive R waves in V4-V9 constitutes positive precordial concordance - all chest leads deflect in the same (positive) direction. This pattern is a strong independent marker of VT and is rarely seen in SVT with aberrant conduction. - Tintinalli's Emergency Medicine, p. 158
Northwest/Extreme QRS Axis (-123° to +117° range suggests a rightward-superior axis)
A QRS axis in the "northwest" quadrant (negative in lead I, positive in aVR) is virtually diagnostic of VT when combined with tachycardia. The tall positive QRS in aVR is a key finding here. - Frameworks for Internal Medicine, p. 90
Why NOT SVT with Aberrancy?
The key distinguishing features make SVT with aberrancy extremely unlikely:
- Classic LBBB aberrancy would show a classic rS or QS in V1 but also show a positive RS in V5-V6, not a uniform tall monophasic R wave
- Classic RBBB aberrancy would show a triphasic RSR' pattern in V1, not QS
- Positive precordial concordance is the hallmark of VT, not bundle branch block
- The PR of 67 ms is physiologically impossible for a conducted supraventricular beat (minimum physiologic PR is ~100 ms) - confirms AV dissociation
Clinical Urgency
This is a hemodynamically significant rhythm requiring urgent assessment:
-
Immediate: Assess hemodynamic stability (BP, consciousness, perfusion)
- If unstable: Synchronized DC cardioversion immediately
- If stable: Proceed with pharmacologic management
-
Pharmacologic options (stable VT):
- IV Amiodarone 150 mg over 10 min, then 1 mg/min infusion (first-line)
- IV Procainamide 20-50 mg/min (if no structural heart disease)
- Avoid adenosine, verapamil, and diltiazem (dangerous in VT)
-
Investigate underlying cause: Check electrolytes (K+, Mg2+), troponin, echo for structural heart disease (ischemic cardiomyopathy is the most common substrate for sustained VT)
-
Correct reversible causes: Hypokalemia, hypomagnesemia, ischemia
Summary
Diagnosis: Monomorphic Ventricular Tachycardia (MVT) - Rate 153 bpm, QRS 138 ms, positive precordial concordance, northwest axis, probable AV dissociation. This is an ICU emergency. Immediate hemodynamic assessment and rhythm termination are required.
Based on Brugada criteria - Frameworks for Internal Medicine, p. 90; Tintinalli's Emergency Medicine, p. 158
This is a shared conversation. Sign in to Orris to start your own chat.