I now have everything needed. Let me compile the full BMC MCQ guide with diagrams.
🧠 BMC HIGH-YIELD MCQ GUIDE
Sodium Handling by Renal Tubules | Dr. Hader Sakr
Batterjee Medical College - Exam Prep
BMC Past Paper Note: Since BMC past papers are internal/not publicly indexed, the "past year appearances" below are based on the standard exam pattern for BMC Physiology (Renal Block), cross-referenced with the topic weight and exam format patterns from Dr. Sakr's lectures. These are flagged as "High probability BMC appearance" based on topic frequency, not verified leaked papers.
📌 SLIDE 4-5 — Importance of Sodium
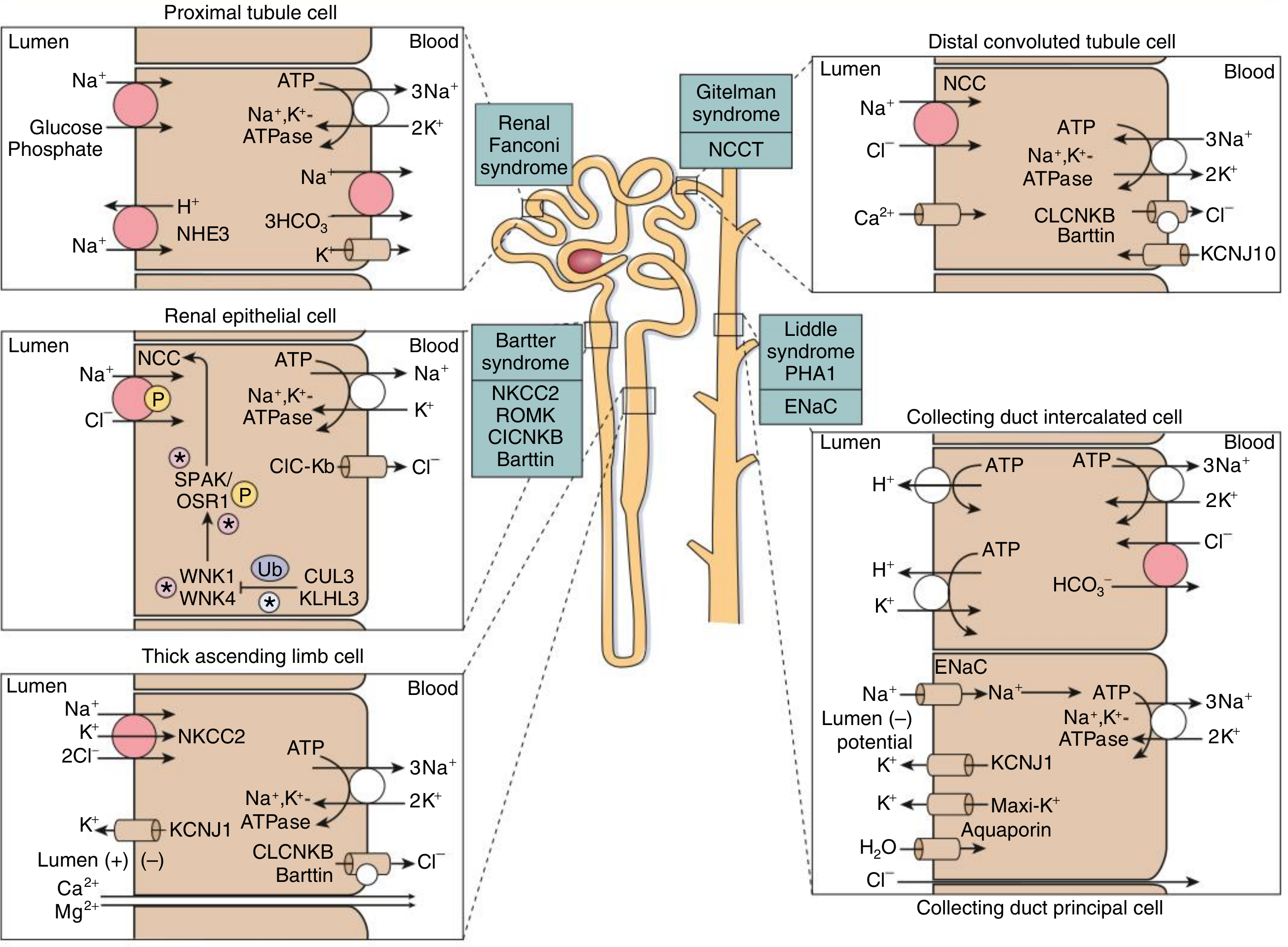
Key Diagram:
Fig. Overview of molecular sodium handling across nephron segments - Comprehensive Clinical Nephrology 7e
MCQ 1 (Slide 5)
What percentage of the filtered Na⁺ is reabsorbed by all portions of the renal tubule (excluding the thin descending loop of Henle)?
- A. 50–70%
- B. 75–85%
- C. 96–99% ✅
- D. 100%
- E. 80–90%
Answer: C
Explanation: According to Guyton & Hall (13th ed.), 96% to over 99% of filtered Na⁺ is reabsorbed across all tubular segments except the thin descending limb. The thin descending limb lacks Na⁺ transport proteins on its luminal membrane and therefore cannot reabsorb Na⁺.
BMC Exam Tip: This exact percentage appears as a stem-completion question. Watch for the "except thin descending" qualifier - it is the classic distractor.
MCQ 2 (Slide 5)
What percentage of total kidney energy expenditure is used specifically for active Na⁺ transport?
- A. 50%
- B. 70%
- C. 80%
- D. 90% ✅
- E. 95%
Answer: D
Explanation: 90% of renal energy consumption goes to active Na⁺ transport via Na⁺/K⁺-ATPase. This Na⁺ transport powers secondary active reabsorption of glucose, amino acids, and drives Cl⁻ reabsorption by electrical gradient and H₂O by osmosis.
BMC Exam Tip: Paired frequently with "which substances are co-transported with Na⁺" - know glucose, amino acids (secondary active), Cl⁻ (electrical diffusion), H₂O (osmosis).
MCQ 3 (Slide 5)
Na⁺ reabsorption in the renal tubule is coupled with the SECRETION of which of the following?
- A. Glucose and amino acids
- B. Cl⁻ and H₂O
- C. H⁺ and K⁺ ✅
- D. HCO₃⁻ and phosphate
- E. Bicarbonate and glucose
Answer: C
Explanation: Active Na⁺ transport is coupled to secretion of H⁺ (via Na⁺/H⁺ counter-transport) and K⁺ (secondary active secretion in DCT/CDs under aldosterone). Glucose and amino acids are co-reabsorbed (not secreted) with Na⁺.
BMC Exam Tip: "Coupled with secretion" vs "coupled with reabsorption" - this distinction is commonly tested.
📌 SLIDE 7-9 — Na⁺ Reabsorption in PCT
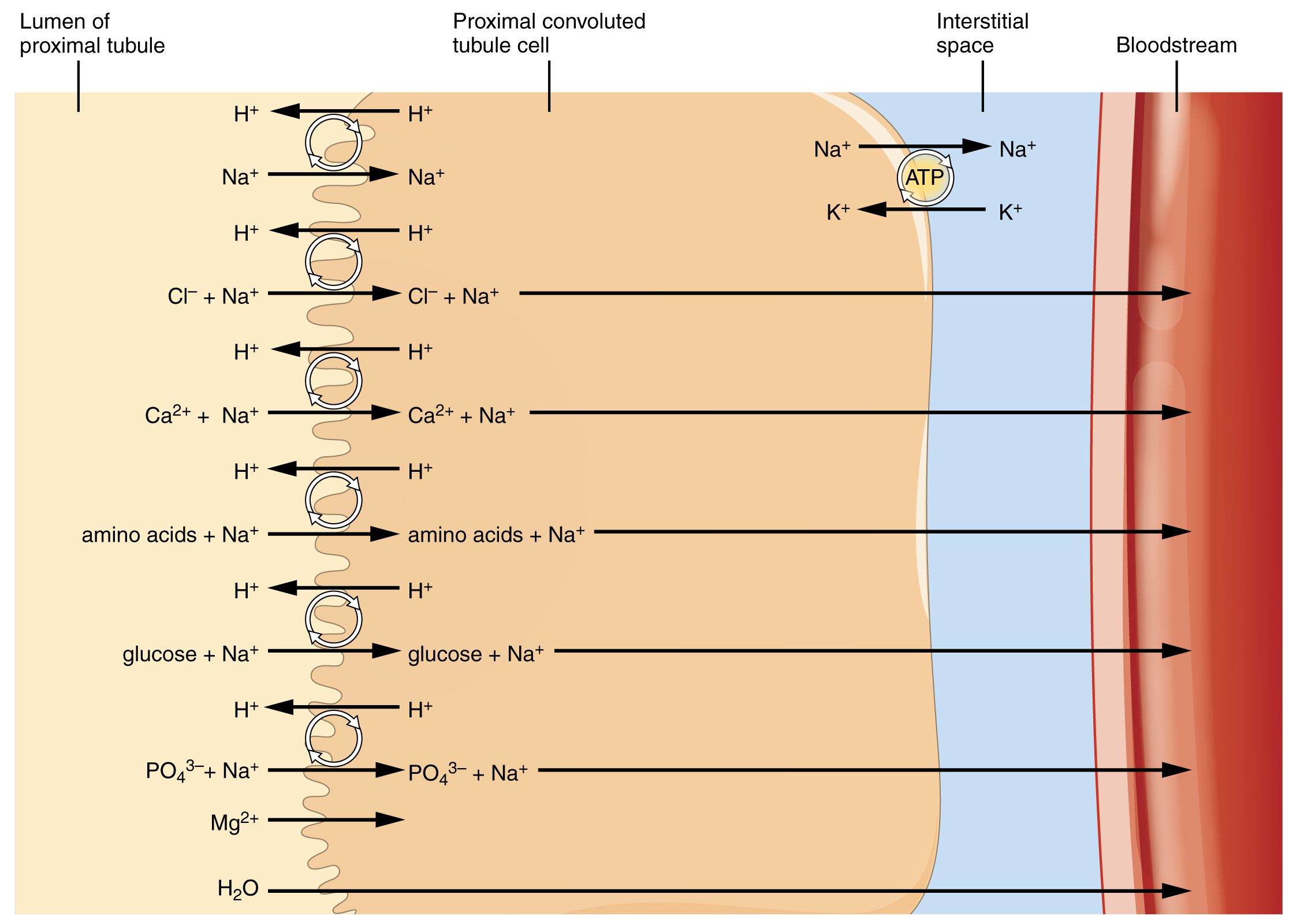
Key Diagram:
PCT reabsorption - early half cotransport vs. late half NaCl reabsorption
MCQ 4 (Slide 8)
What percentage of filtered Na⁺ is reabsorbed by the proximal convoluted tubule (PCT)?
- A. 25%
- B. 40–50%
- C. 60–65% ✅
- D. 75–80%
- E. 90%
Answer: C
Explanation: The PCT reabsorbs 60–65% of the filtered Na⁺ load. It follows gradient-time transport. The PCT is the single most important segment for bulk Na⁺ reabsorption.
BMC Exam Tip: This is one of the most frequently tested numerical facts in renal block. Memorize: PCT = 65%, TAL = 25%, Early DCT = 7%, Late DCT/CD = 3%.
MCQ 5 (Slide 8-9)
In the FIRST half of the PCT, Na⁺ is co-transported with all of the following EXCEPT:
- A. Glucose
- B. Amino acids
- C. HCO₃⁻
- D. Chloride ✅
- E. Phosphate
Answer: D
Explanation: In the first half of the PCT, Na⁺ is co-transported with glucose, amino acids, sulphate, phosphate, organic acids, and HCO₃⁻. Chloride (NaCl) is the primary anion reabsorbed in the second (late) half of PCT, not the first half. This is a classic "EXCEPT" trap in BMC exams.
BMC Exam Tip: First half PCT = glucose + amino acids + HCO₃⁻. Late half PCT = NaCl. Know this distinction cold.
MCQ 6 (Slide 9)
A patient with reduced carbonic anhydrase (CA-IV) activity in the PCT luminal membrane would MOST LIKELY develop:
- A. Hyperkalemia
- B. Metabolic acidosis with loss of Na⁺, K⁺, and HCO₃⁻ ✅
- C. Metabolic alkalosis with Na⁺ retention
- D. Hypernatremia
- E. Hypochloremia with metabolic alkalosis
Answer: B
Explanation: CA-IV in the luminal membrane catalyzes H⁺ + HCO₃⁻ → CO₂ + H₂O. Without this, H⁺ cannot be neutralized in the lumen, Na⁺/H⁺ counter-transport fails, Na⁺ is lost, and HCO₃⁻ is wasted in urine → metabolic acidosis. This is the mechanism of carbonic anhydrase inhibitors (acetazolamide/Diamox).
BMC Exam Tip: Acetazolamide mechanism is always testable. CA-IV = luminal, CA-II = intracellular. Both are needed.
📌 SLIDE 11-14 — Loop of Henle & Early DCT
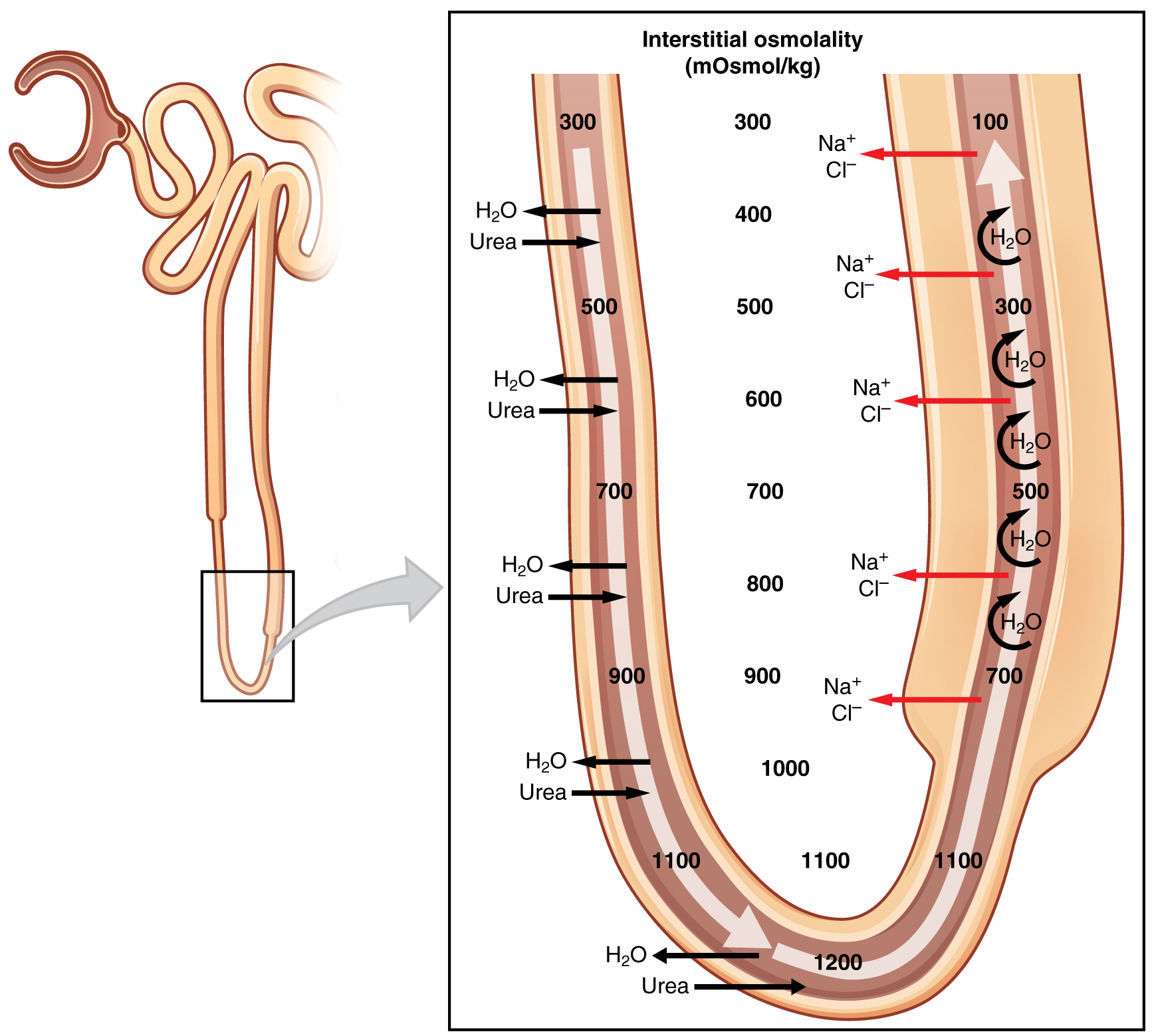
Key Diagram:
Loop of Henle segments - osmolarity changes and permeability features
MCQ 7 (Slide 11)
Which segment of the loop of Henle is IMPERMEABLE to Na⁺ transport proteins and channels on the luminal membrane?
- A. Thin ascending limb
- B. Thick ascending limb
- C. Thin descending limb ✅
- D. Early DCT
- E. Medullary collecting duct
Answer: C
Explanation: The thin descending limb lacks Na⁺ transport proteins on its luminal membrane entirely. It only reabsorbs water (highly water permeable). As a result, Na⁺ concentration and tubular osmolarity actually INCREASE as fluid moves down (up to 1200-1400 mOsm/L). This is a classic BMC MCQ stem.
BMC Past Year Pattern: "A segment reabsorbs water but not Na⁺" - answer always = thin descending limb.
MCQ 8 (Slide 12-13)
The Na⁺/K⁺/2Cl⁻ cotransporter (NKCC2) in the thick ascending limb serves which of the following purposes via K⁺ back-flux into the lumen?
- A. Generating a lumen-negative potential
- B. Generating a lumen-positive potential that drives paracellular cation reabsorption ✅
- C. Directly secreting K⁺ into the tubular lumen
- D. Preventing K⁺ accumulation in the cell
- E. Activating aldosterone receptors
Answer: B
Explanation: K⁺ that enters TAL cells via NKCC2 refluxes back into the lumen through ROMK (K⁺ channels). This creates a lumen-positive potential that drives paracellular reabsorption of Na⁺, K⁺, Ca²⁺, and Mg²⁺. This is also why loop diuretics (furosemide) block not just Na⁺/Cl⁻ but also Ca²⁺ and Mg²⁺ reabsorption.
BMC Exam Tip: "Lumen positive in TAL" is a very high-yield fact. It's the mechanism for paracellular Mg²⁺/Ca²⁺ reabsorption and the reason loop diuretics cause hypercalciuria and hypomagnesemia.
MCQ 9 (Slide 13)
A child presents with polyuria, renal salt wasting, hypokalemia, hypercalciuria, and metabolic alkalosis. Genetic testing reveals a defect in the Na⁺/K⁺/2Cl⁻ cotransporter. What is the MOST LIKELY diagnosis?
- A. Gitelman syndrome
- B. Liddle syndrome
- C. Bartter syndrome ✅
- D. Pseudohypoaldosteronism type 1
- E. Gordon syndrome
Answer: C
Explanation: Bartter syndrome is caused by loss-of-function mutation in NKCC2 in the TAL → Na⁺, K⁺, Cl⁻, and Ca²⁺ are all lost → salt wasting, volume depletion, hypokalemia, hypercalciuria, and metabolic alkalosis (compensatory H⁺ secretion in DCT). Gitelman syndrome affects NCC in DCT and has hypocalciuria (opposite finding).
BMC Past Year Pattern: Bartter vs. Gitelman distinction is a very commonly tested clinical scenario in BMC renal physiology. Key differentiator: Bartter = hypercalciuria; Gitelman = hypocalciuria.
MCQ 10 (Slide 14)
The early distal tubule (cortical diluting segment) reabsorbs Na⁺ via which transporter?
- A. ENaC
- B. NKCC2
- C. Na⁺/H⁺ counter-transporter
- D. Na⁺/Cl⁻ co-transporter (NCC) ✅
- E. Na⁺/K⁺ ATPase on the luminal membrane
Answer: D
Explanation: The early DCT reabsorbs ~7% of filtered Na⁺ via the apical Na⁺/Cl⁻ co-transporter (NCC). This is impermeable to water (diluting segment), so tubular fluid osmolarity falls to ~60 mOsm/L. NCC is the site of action for thiazide diuretics.
BMC Exam Tip: NKCC2 → TAL → furosemide. NCC → Early DCT → thiazides. ENaC → Late DCT/CDs → aldosterone/spironolactone. Know all three cold.
📌 SLIDE 15-16 — Late DCT and Collecting Ducts
MCQ 11 (Slide 16)
Aldosterone increases Na⁺ reabsorption in the late DCT and collecting ducts by acting on which cell type and channel?
- A. Intercalated (I) cells via H⁺-ATPase
- B. Principal (P) cells via ENaC channels ✅
- C. Macula densa cells via NKCC2
- D. Mesangial cells via cGMP
- E. PCT cells via Na⁺/H⁺ exchange
Answer: B
Explanation: Aldosterone acts on principal (P) cells of the late DCT and CDs, increasing: (a) number of apical ENaC channels, (b) number of basolateral Na⁺/K⁺-ATPase molecules, and (c) ATP generation. Na⁺ enters via ENaC and is extruded basolaterally via Na⁺/K⁺-ATPase. This occurs in exchange for K⁺ secretion.
BMC Past Year Pattern: "Aldosterone mechanism" appears in virtually every BMC renal exam. Know: principal cell, ENaC, basolateral Na⁺/K⁺-ATPase.
MCQ 12 (Slide 16)
In the late DCT and collecting duct, the luminal negative potential generated by Na⁺ reabsorption drives which of the following?
- A. Active K⁺ reabsorption
- B. Paracellular Cl⁻ reabsorption ✅
- C. Paracellular Ca²⁺ reabsorption
- D. Active H₂O transport
- E. HCO₃⁻ secretion
Answer: B
Explanation: Na⁺ moves from lumen into the principal cell via ENaC, creating a lumen-negative potential. This electrical gradient drives paracellular Cl⁻ reabsorption. (Contrast with TAL where lumen is positive, driving paracellular Ca²⁺/Mg²⁺.)
BMC Exam Tip: Lumen charge = critical. TAL = lumen positive → Ca²⁺/Mg²⁺. Late DCT/CD = lumen negative → Cl⁻.
MCQ 13 (Slide 16)
What percentage of filtered Na⁺ is reabsorbed by the late DCT and collecting ducts under aldosterone control?
- A. 25%
- B. 10%
- C. 7%
- D. 3% ✅
- E. Less than 1%
Answer: D
Explanation: Although only ~3% of filtered Na⁺ is handled here, this segment is critical because it is the fine-tuning segment under hormonal control. Small changes in reabsorption here have major effects on final urine Na⁺ output and blood pressure regulation.
📌 SLIDE 18-21 — Regulation of Na⁺ Excretion (GFR & Pressure)
MCQ 14 (Slide 19)
Glomerulo-tubular balance (GT balance) ensures that the PCT reabsorbs a constant PERCENTAGE of filtered Na⁺ rather than a constant amount. What percentage is this?
- A. 45%
- B. 50%
- C. 65% (2/3) ✅
- D. 75%
- E. 90%
Answer: C
Explanation: GT balance states that when GFR increases, tubular reabsorption increases proportionally so that the PCT always reabsorbs ~65% (2/3) of the filtered load. This is hormone-independent and prevents flooding of distal segments. Main site: PCT (also loop of Henle participates).
BMC Past Year Pattern: "GT balance - which site?" = PCT. "GT balance - hormone dependent?" = No.
MCQ 15 (Slide 20-21)
Which of the following best explains the mechanism of pressure diuresis and natriuresis when arterial blood pressure (ABP) rises?
- A. Increased aldosterone secretion
- B. Increased renal sympathetic activity
- C. Decreased peritubular capillary hydrostatic pressure allowing Na⁺ retention
- D. Increased peritubular capillary hydrostatic pressure → back-leak of Na⁺ into tubular lumen ✅
- E. Increased ANP secretion as the primary mechanism
Answer: D
Explanation: Elevated ABP → increased peritubular capillary hydrostatic pressure (HP) → rise in interstitial fluid HP → Na⁺ back-leaks into tubular lumen → reduced net Na⁺ reabsorption → increased urine output (natriuresis). Additionally, angiotensin II secretion decreases with rising ABP. This mechanism is independent of hormones and nervous system.
BMC Exam Tip: The key phrase is "back-leak" into lumen. Also note: increased ABP decreases Ang II → less Na⁺ retention. Two mechanisms act together.
MCQ 16 (Slide 19-20)
A sudden increase in GFR would MOST LIKELY result in:
- A. Proportional increase in Na⁺ excretion
- B. No change in Na⁺ excretion due to auto-regulation
- C. Only a slight increase in Na⁺ excretion due to glomerulo-tubular balance ✅
- D. Massive natriuresis
- E. Decreased urine output
Answer: C
Explanation: GT balance means that as GFR rises, PCT reabsorption also rises proportionally (reabsorbing 65% of the larger filtered load). Only a slight net increase in Na⁺ excretion occurs. Without GT balance, any GFR fluctuation would cause dangerous Na⁺ and water losses.
📌 SLIDE 22-25 — Hormonal Control of Na⁺ Excretion
MCQ 17 (Slide 22-23)
Angiotensin II is considered the MOST POWERFUL Na⁺-retaining hormone. Which of the following is NOT a direct mechanism of its action?
- A. Stimulates aldosterone secretion
- B. Stimulates Na⁺/K⁺-ATPase in PCT
- C. Stimulates Na⁺/H⁺ counter-transport in PCT
- D. Dilates efferent arteriole to reduce filtration fraction ✅
- E. Constricts efferent arteriole to increase peritubular capillary reabsorption
Answer: D
Explanation: Angiotensin II CONSTRICTS (not dilates) the efferent arteriole, which: increases FF (filtration fraction), reduces RBF, raises peritubular capillary oncotic pressure (π), and lowers peritubular HP → all favor Na⁺ and water reabsorption by peritubular capillaries in PCT. Dilation would have the opposite effect.
BMC Exam Tip: "Most powerful Na⁺-retaining hormone" = Angiotensin II (not aldosterone). Three mechanisms: direct PCT action + aldosterone stimulation + efferent arteriole constriction.
MCQ 18 (Slide 24-25)
Atrial natriuretic peptide (ANP) decreases Na⁺ reabsorption by which combination of mechanisms?
- A. Inhibits ENaC + inhibits Na⁺/K⁺-ATPase + increases GFR via mesangial relaxation and afferent arteriole dilation ✅
- B. Inhibits NKCC2 + stimulates aldosterone
- C. Stimulates renin + blocks NCC in DCT
- D. Inhibits Na⁺/H⁺ exchange in PCT + constricts afferent arteriole
- E. Directly inhibits H⁺ secretion only
Answer: A
Explanation: ANP increases cGMP synthesis which:
- Relaxes mesangial cells → ↑ surface area for filtration → ↑ GFR
- Dilates afferent arteriole → ↑ GFR
- Inhibits apical ENaC channels (direct effect on P cells)
- Inhibits basolateral Na⁺/K⁺-ATPase
- Inhibits renin → ↓ Ang II and aldosterone (indirect)
- Directly inhibits aldosterone secretion from adrenal cortex
BMC Exam Tip: ANP = released from atria when ECF expands → promotes salt & water excretion. The cGMP mechanism and mesangial relaxation are favorite exam points.
📌 SLIDE 26-28 — Sympathetic Stimulation & Diuretics
MCQ 19 (Slide 26)
Sympathetic stimulation increases Na⁺ reabsorption through all of the following EXCEPT:
- A. Increases renin secretion → more Ang II
- B. Direct stimulation of Na⁺ reabsorption in PCT and TAL
- C. Increases filtration fraction by constricting renal vessels
- D. Inhibits aldosterone secretion ✅
- E. Increases Na⁺/K⁺-ATPase activity
Answer: D
Explanation: Sympathetic stimulation increases (not inhibits) aldosterone secretion indirectly via increased renin → Ang II → aldosterone. It also directly reabsorbs Na⁺ in PCT and TAL and increases filtration fraction. All effects favor Na⁺ retention.
MCQ 20 (Slide 27-28)
A patient is prescribed furosemide (Lasix). Which transporter does it inhibit and where?
- A. NCC in early DCT
- B. ENaC in late DCT and collecting ducts
- C. Na⁺/H⁺ exchanger in PCT
- D. Na⁺/K⁺/2Cl⁻ (NKCC2) in the thick ascending limb ✅
- E. Na⁺/K⁺-ATPase in the basolateral membrane
Answer: D
Explanation: Furosemide (frusemide/Lasix) is a loop diuretic that inhibits NKCC2 in the TAL → blocks 25% of filtered Na⁺ reabsorption → massive diuresis. It also prevents the lumen-positive potential → reduces paracellular Ca²⁺ and Mg²⁺ reabsorption → hypercalciuria, hypomagnesemia.
BMC Past Year Pattern: "Diuretic mechanism" MCQs appear in EVERY renal exam at BMC. Match: Loop diuretic (furosemide) → NKCC2/TAL. Thiazide → NCC/early DCT. Spironolactone/Aldactone → ENaC/late DCT+CD.
MCQ 21 (Slide 28)
A patient on spironolactone (Aldactone) for heart failure would be expected to have:
- A. Hypokalemia and metabolic alkalosis
- B. Hypernatremia and hypokalemia
- C. Hyperkalemia and increased Na⁺ excretion ✅
- D. Hyponatremia and increased K⁺ excretion
- E. Metabolic acidosis with hypernatremia
Answer: C
Explanation: Spironolactone is an aldosterone antagonist that blocks ENaC and the Na⁺/K⁺ exchange in late DCT and CDs. Result: Na⁺ is NOT reabsorbed (excreted in excess) and K⁺ is NOT secreted (retained in body = hyperkalemia). It is a potassium-sparing diuretic.
BMC Exam Tip: "K⁺-sparing diuretics" = spironolactone/aldactone, amiloride, triamterene. All block the late DCT/CD segment via different mechanisms.
📋 HIGH-YIELD SUMMARY CHEATSHEET
🔢 Na⁺ Reabsorption - Numbers to Memorize
| Segment | % of Filtered Na⁺ | Transporter (Apical) | Water Permeability | Osmolarity |
|---|
| PCT | 65% | Na⁺/glucose, Na⁺/AA, Na⁺/H⁺, Na⁺/Cl⁻ (late) | Permeable | 300 mOsm |
| Thin Descending LOH | 0% (NO Na⁺ transport) | None | High (aquaporins) | ↑ to 1200-1400 |
| Thin Ascending LOH | Small, passive | Passive diffusion | Impermeable | ↓ to 300 |
| Thick Ascending LOH | 25% | NKCC2 (furosemide target) | Impermeable | ↓ to 100 |
| Early DCT | 7% | NCC (thiazide target) | Impermeable | ↓ to 60 |
| Late DCT + CD | 3% | ENaC (aldosterone/spironolactone) | ADH-dependent | Variable |
🧬 Transporter Cheat Card
| Transporter | Segment | Drug that blocks it | Disease if defective |
|---|
| NKCC2 | TAL thick ascending | Furosemide (Lasix) | Bartter syndrome |
| NCC | Early DCT | Thiazides (HCTZ) | Gitelman syndrome |
| ENaC | Late DCT/CD | Spironolactone, Amiloride | Liddle syndrome (gain of function) |
| Na⁺/H⁺ (NHE3) | PCT | Acetazolamide (indirect) | — |
| Na⁺/K⁺-ATPase | Basolateral everywhere | — | — |
💊 Hormone Quick-Fire Table
| Hormone | Effect on Na⁺ | Site | Mechanism |
|---|
| Aldosterone | ↑ reabsorption | Late DCT + CD | ↑ ENaC + ↑ Na⁺/K⁺-ATPase |
| Angiotensin II | ↑ reabsorption (MOST POWERFUL) | PCT + adrenal + efferent art | Na⁺/H⁺ + Na⁺/K⁺-ATPase + ↑aldosterone + ↑FF |
| Cortisol | Weak ↑ | PCT | Weak mineralocorticoid activity |
| Estrogen | ↑ reabsorption | Renal tubule | — |
| ANP | ↓ reabsorption | Late DCT/CD + mesangial | ↑cGMP → inhibit ENaC + Na⁺/K⁺-ATPase + ↑GFR |
| PGE₂ | ↓ reabsorption | CD | ↑IC Ca²⁺ → inhibit ENaC + Na⁺/K⁺-ATPase |
| Sympathetic | ↑ reabsorption | PCT + TAL | ↑ renin → Ang II + direct tubular effect |
⚡ GT Balance - 3 Key Points
- Site: PCT (primary), Loop of Henle (secondary)
- Reabsorbs constant 65% (2/3) of filtered load regardless of GFR
- Hormone-independent - works in isolated kidney
🩺 Clinical Syndromes Quick Card
| Syndrome | Defect | Key Features |
|---|
| Bartter | NKCC2 (TAL) | Salt wasting, hypokalemia, metabolic alkalosis, HYPERcalciuria |
| Gitelman | NCC (DCT) | Same but HYPOcalciuria, hypomagnesemia |
| Liddle | ENaC gain-of-function | HTN, hypokalemia, low aldosterone |
| PHA type 1 | ENaC loss-of-function | Salt wasting, HYPERkalemia |
🎯 BMC EXAM TIPS - Final 48 Hours
-
Numbers are king - 65% PCT, 25% TAL, 7% early DCT, 3% late DCT/CD, 96-99% total. Write them 5 times.
-
Thin descending = NO Na⁺ transport - This appears almost every exam. The only segment that cannot reabsorb Na⁺.
-
Lumen charge trick:
- TAL = Lumen positive → drives Ca²⁺/Mg²⁺/Na⁺ paracellular
- Late DCT/CD = Lumen negative → drives Cl⁻ paracellular
-
Diuretic-transporter-segment matching is almost always 1-2 MCQs per BMC renal exam.
-
Bartter vs Gitelman - Always asked as a clinical vignette. Key: Bartter = hypercalciuria. Gitelman = hypocalciuria + hypomagnesemia.
-
"Most powerful Na⁺ retaining hormone" = Angiotensin II (NOT aldosterone - trick question).
-
ANP mechanism: cGMP is the second messenger - mesangial relaxation + ENaC inhibition + anti-aldosterone. Volume expansion → ANP → natriuresis.
-
Pressure natriuresis = back-leak mechanism + ↓Ang II. This is hormone-independent by pressure alone.
-
For EXCEPT/NEGATIVE questions - read every option twice. BMC loves double-negatives in diuretic and hormonal questions.
-
Acetazolamide → inhibits CA → ↓H⁺ secretion → ↓Na⁺/H⁺ exchange → Na⁺, K⁺, HCO₃⁻ lost → metabolic acidosis (it is self-limiting).
Sources: Dr. Hader Sakr lecture (BMC), Guyton & Hall Medical Physiology 13th Ed. (Unit V, Ch. 26), Ganong's Review of Medical Physiology 25th Ed. (Section VII, Ch. 37), Comprehensive Clinical Nephrology 7e, Harrison's Principles of Internal Medicine 22e.