Here is the complete, structured account of Scabies according to Harrison's Principles of Internal Medicine 22E (2025), with nothing omitted.
SCABIES
Harrison's Principles of Internal Medicine 22E (2025)
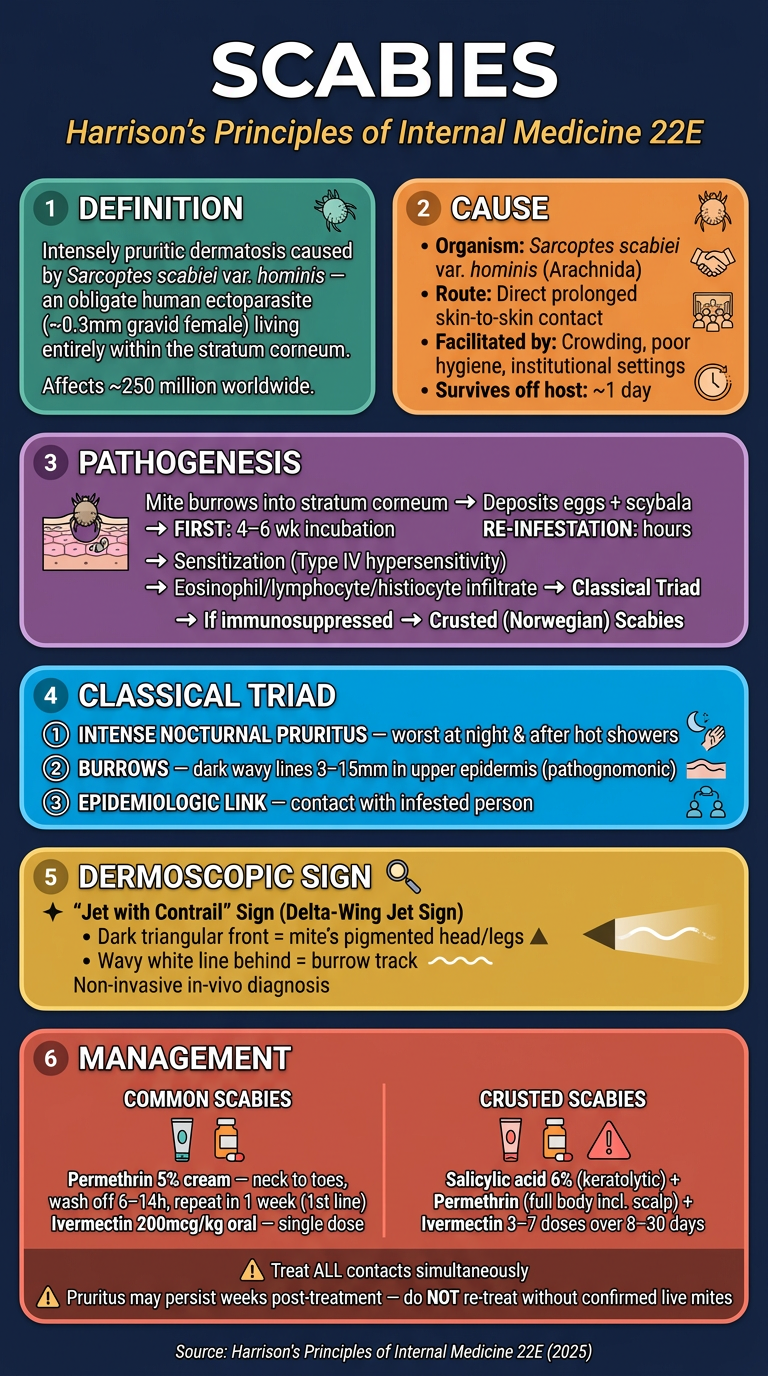
1. DEFINITION
Scabies is an intensely pruritic dermatosis caused by infestation with Sarcoptes scabiei var. hominis, an obligate human ectoparasite. Both the mites and the skin condition are called "scabies." It affects approximately 250 million persons worldwide and is classified as an infestation (not an infection), since the parasite lives entirely on the mucocutaneous surface.
2. CAUSE (ETIOLOGY)
| Feature | Detail |
|---|
| Causative organism | Sarcoptes scabiei var. hominis (human itch mite) - class Arachnida |
| Mite size | Gravid female ~0.3 mm in length |
| Life cycle site | Entire life cycle within human stratum corneum |
| Transmission | Primarily by direct, prolonged skin-to-skin contact |
| Facilitating factors | Crowding, poor hygiene, close physical contact |
| Survival off host | Mites generally die within a day without a suitable host |
| Settings | Preschools, hospitals, nursing homes, prisons, congregate settings |
| Less common route | Sharing contaminated bedding/clothing (less frequent than commonly thought) |
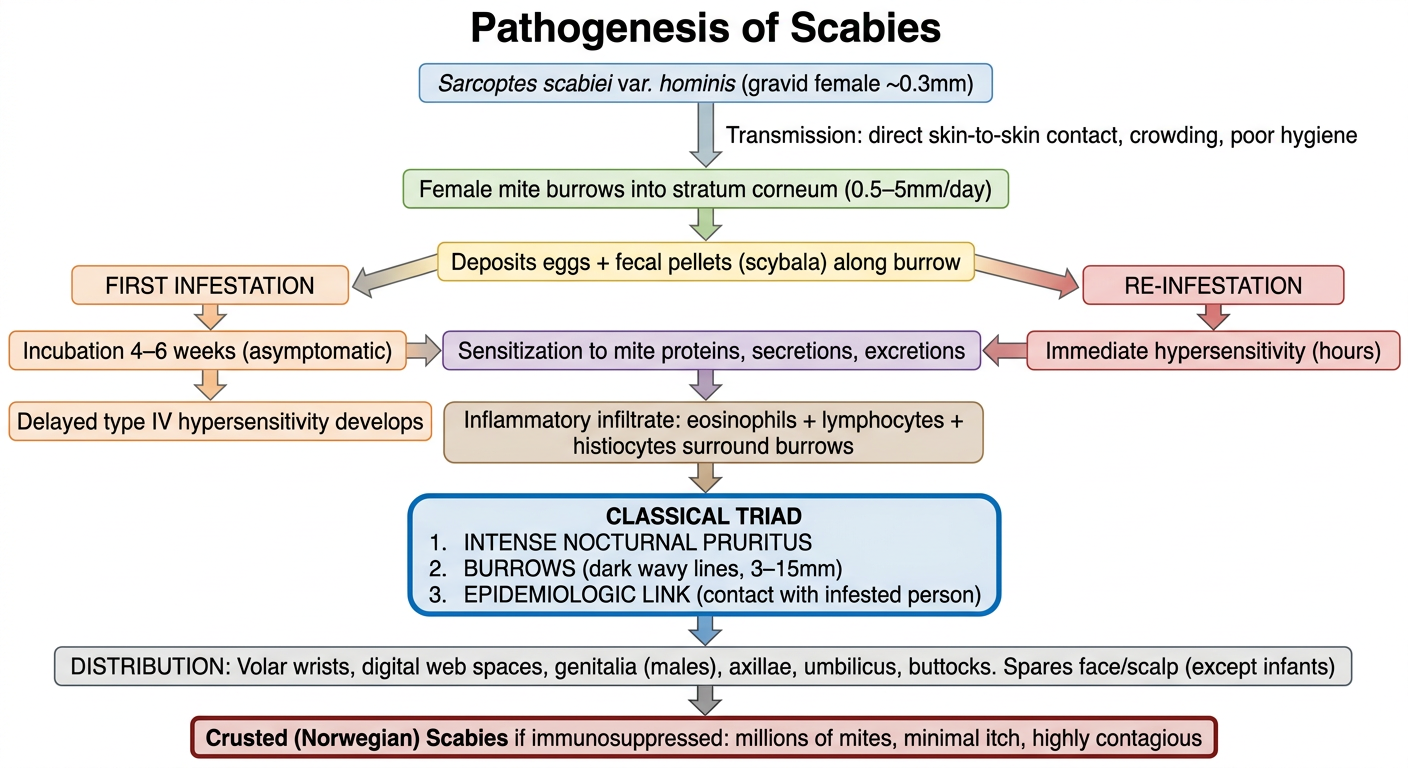
3. PATHOGENESIS FLOWCHART
Step-by-step (as per Harrison's):
Gravid female mite (~0.3mm) transferred via skin-to-skin contact
│
▼
Mite burrows superficially into the STRATUM CORNEUM
(excavates 0.5–5 mm/day by chewing + body movements)
│
▼
Deposits several EGGS per day + fecal pellets (scybala)
along the burrow track (burrow length: 3–15 mm)
│
▼
┌────┴────┐
│ │
FIRST RE-INFESTATION
INFESTATION
│ │
Incubation Immediate
4–6 weeks hypersensitivity
(silent) (hours)
│ │
└────┬────┘
▼
SENSITIZATION REACTION to mite proteins,
secretions, and excretions
│
▼
Inflammatory infiltrate surrounds burrows:
EOSINOPHILS + LYMPHOCYTES + HISTIOCYTES
│
▼
╔══════════════════════════════════════╗
║ CLASSICAL TRIAD (see below) ║
╚══════════════════════════════════════╝
│
▼
If host is immunosuppressed/has impaired
itch or scratch response
│
▼
CRUSTED (NORWEGIAN) SCABIES
(thousands-millions of mites, minimal itch,
highly contagious, resembles psoriasis)
4. CLASSICAL TRIAD
Per Harrison's 22E - when mites/eggs cannot be microscopically identified, clinical diagnosis is based on a triad of:
| # | Component | Harrison's Description |
|---|
| 1 | Pruritus | Intense, generalised; worst at night and after hot showers. First infestation: starts after 4-6 weeks; re-infestation: starts within hours |
| 2 | Physical examination findings | Pathognomonic burrows - dark wavy lines in the upper epidermis, 3-15 mm long (most obscured by excoriations or secondary bacterial infection). Also papules, vesicles, eczematous plaques, pustules, or nodules - distributed symmetrically |
| 3 | Epidemiologic link | Direct and prolonged contact with an infested person (household, sexual, or institutional contact) |
"Unrelated skin diseases are frequently misdiagnosed as scabies, particularly in presumed 'outbreak' situations." - Harrison's 22E
5. CLINICAL PHOTOGRAPH - Scabies Burrows
FIGURE 472-1 from Harrison's 22E:
"Scabies mites create short, delicate, linear burrows within the superficial epidermis. Although burrows are pathognomonic for scabies, most have been altered by scratching or secondary bacterial infection."
- Harrison's Principles of Internal Medicine 22E, Fig. 472-1
6. DERMOSCOPY (DERMATOSCOPY) IN SCABIES
Harrison's 22E specifically mentions dermatoscopic imaging as a diagnostic tool:
"Dermatoscopic imaging of papulovesicular lesions... also may be diagnostic."
The classic dermoscopic sign is the "jet with contrail" sign (also called the "delta-wing jet" sign):
- The dark triangular front end = the mite's pigmented front legs and mouthparts (head)
- The wavy white/translucent line behind it = the burrow track in the stratum corneum
- This allows non-invasive, in-vivo visualization of the mite within its burrow, avoiding the need for skin scraping in many cases
- Harrison's lists dermoscopy alongside skin scraping, biopsy, cyanoacrylate adhesive lift, and cellophane tape methods as confirmatory techniques
7. DISTRIBUTION OF LESIONS
Per Harrison's:
- Always involved in males: penile glans, shaft, and scrotum
- Common sites: volar wrists, digital web spaces, axillae, intertriginous areas, around navel and belt line, buttocks, upper thighs
- Spared (except in infants): face, neck, scalp, palms, and soles
- Infants: generalized, including face, scalp, palms, soles
8. DIAGNOSIS
| Method | Notes |
|---|
| Skin scraping | Gold standard - unroof burrow with sterile needle/scalpel, examine microscopically for mites, eggs, scybala |
| Biopsy | Histology shows mite, eggs, fecal pellets |
| Cellophane tape / cyanoacrylate adhesive lift | Lifted from lesion surface |
| Dermoscopy | "Jet with contrail" sign - in-vivo, non-invasive |
| Clinical (triad) | Used when mites/eggs cannot be identified |
9. MANAGEMENT
(Harrison's 22E Treatment section)
Standard (Common) Scabies
| Drug | Route | Instructions |
|---|
| Permethrin 5% cream | Topical | Apply thinly but thoroughly from jawline to toes after bathing; special attention to interdigital spaces, navel, under nails. Wash off 6-14 hours later with soap and water. Repeat in 1 week (eggs are relatively resistant). Less toxic than lindane. Effective against lindane-resistant strains. |
| Ivermectin 200 mcg/kg | Oral (single dose) | Effective in healthy patients with common (non-crusted) scabies. Not FDA-approved for scabies but approved for hookworm and strongyloidiasis. |
| Crotamiton | Topical | FDA-approved; alternative |
| Spinosad | Topical | FDA-approved; alternative |
| Lindane 1% | Topical | FDA-approved but NOT recommended - more toxic, resistance exists |
Crusted (Norwegian) Scabies
| Step | Action |
|---|
| Keratolytic first | 6% salicylic acid to debulk crusts before scabicide |
| Topical | Permethrin applied to entire skin surface, including scalp, face, and ears |
| Oral | Ivermectin: 3-7 doses over 8-30 days |
| Combination | Both topical permethrin + oral ivermectin + keratolytic required |
Post-Treatment Notes (Harrison's)
- Within 1 day of properly administered treatment, infestation is noncommunicable - patient may return to work/school
- Pruritus may persist for weeks after treatment - dead mites and their detritus continue to provoke hypersensitivity reaction
- Do NOT re-treat immediately for persistent itch alone (unless live mites confirmed)
- All close contacts and household members must be treated simultaneously
- Clothing and bedding should be laundered
Source: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill Medical), Chapter 472 - Ectoparasite Infestations and Arthropod Injuries