Meningitis signs in MRI
Reading File
Finding Sources
Finding Sources
Searching the Web
meningitis MRI signs findings radiology leptomeningeal enhancement
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a thorough, image-rich answer. Here it is:
MRI Signs of Meningitis
MRI is the most sensitive imaging modality for meningitis. Critically, uncomplicated meningitis is frequently MRI-normal - the scan's main role is detecting complications and evaluating atypical or chronic cases.
1. Direct Signs
Leptomeningeal Enhancement (post-contrast T1 / CE-FLAIR)
The hallmark finding. Gadolinium enhancement follows the pial surface, extends into the sulci and basal cisterns in a serpentine pattern. It reflects blood-brain barrier breakdown from inflammatory mediators.
- Pyogenic/viral meningitis: thin, smooth, diffuse enhancement
- TB/fungal/carcinomatous meningitis: thick, nodular, predominantly basal enhancement
- Best detected on post-contrast FLAIR rather than standard post-contrast T1, because CE-FLAIR suppresses normal vascular enhancement and makes pathological leptomeningeal enhancement more conspicuous.
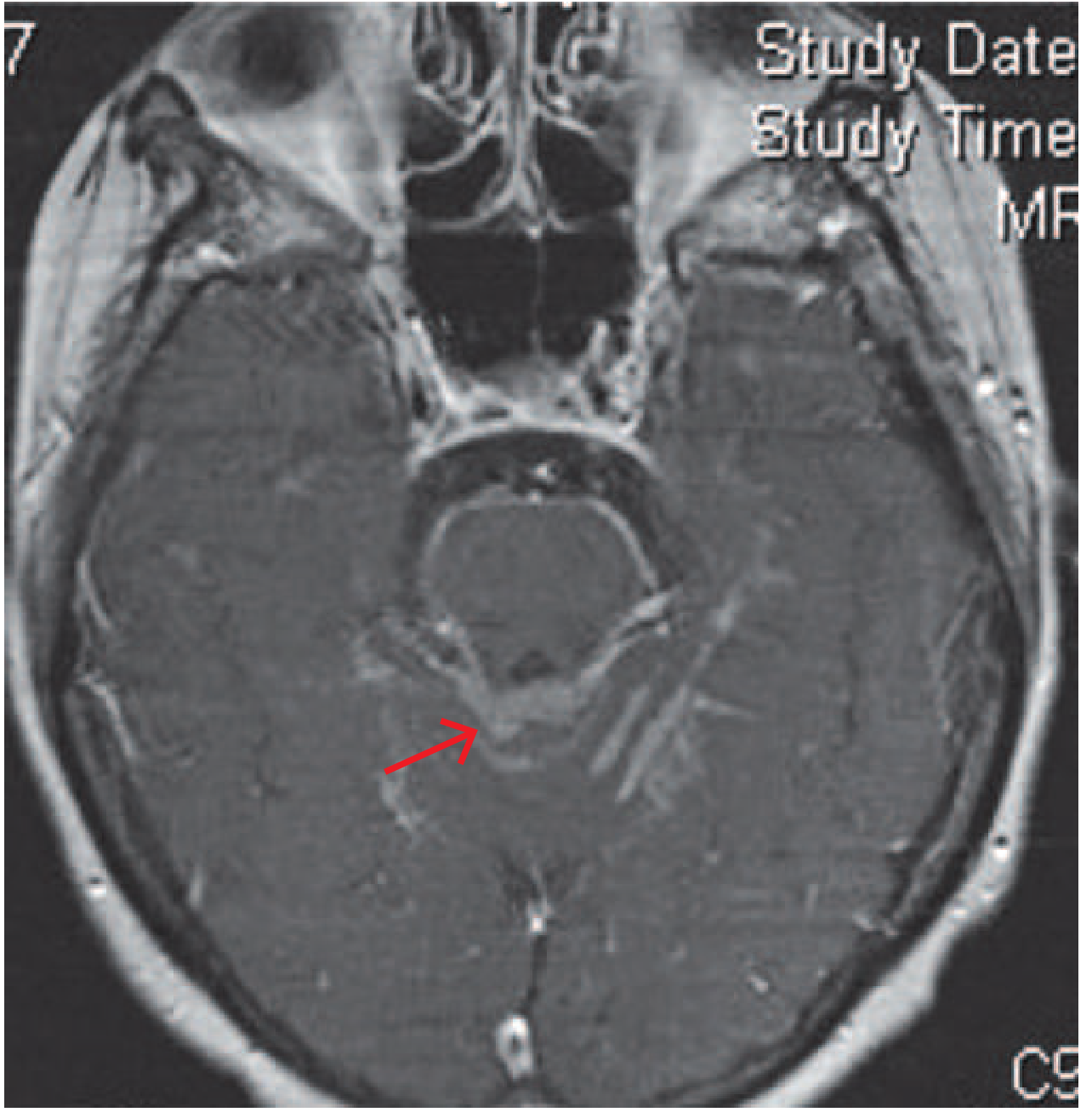
Axial post-contrast MRI in chronic carcinomatous meningitis - red arrow points to leptomeningeal enhancement around the brainstem (Harrison's Principles of Internal Medicine 22E, Fig 144-2)
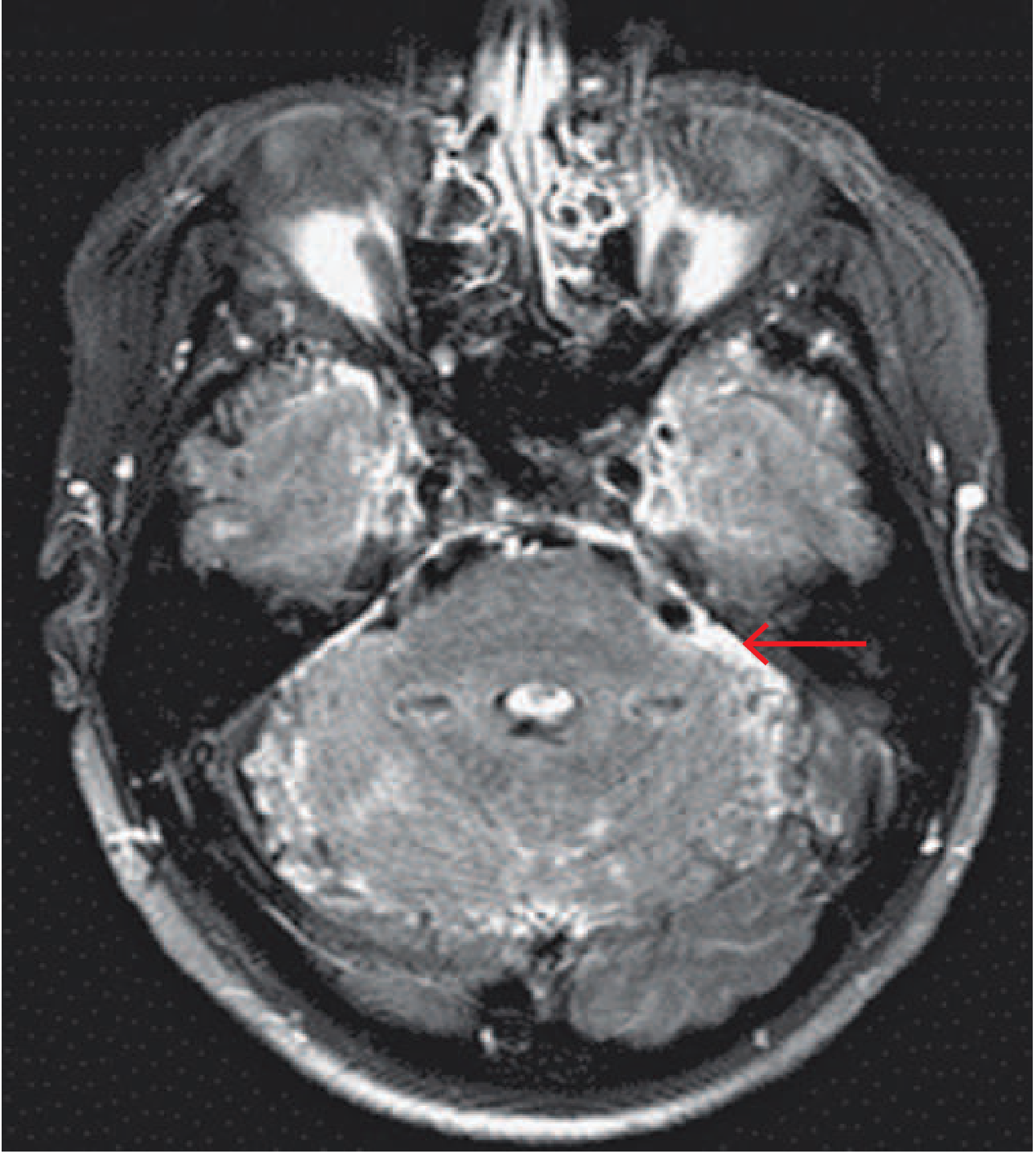
Axial post-contrast MRI in Cryptococcal meningitis - enhancement along the cerebellar folia (arrow) (Harrison's, Fig 144-2C)
FLAIR Sulcal Hyperintensity (pre-contrast)
Unenhanced FLAIR shows increased signal in the subarachnoid spaces (normally suppressed), most often over the frontal convexities and in the Sylvian fissures. This results from elevated CSF protein concentration impairing the inversion-recovery suppression pulse. Non-specific - also seen with subarachnoid hemorrhage and supplemental O2.
DWI Subarachnoid High Signal
In a minority of cases (<10%), DWI shows multiple nodular foci of high signal in the subarachnoid spaces, usually associated with FLAIR hyperintensity. This finding correlates with a poor prognosis.
2. MRI Sequences Summary
| Sequence | Key finding |
|---|---|
| Post-contrast T1 | Leptomeningeal enhancement |
| Post-contrast FLAIR | Most sensitive for leptomeningeal enhancement (suppresses vessels) |
| Pre-contrast FLAIR | Sulcal hyperintensity from raised CSF protein |
| DWI | Subarachnoid restricted diffusion (poor prognosis marker); also shows empyema/abscess |
| T2/FLAIR parenchyma | Cerebritis, edema, infarction |
| MRV | Venous sinus thrombosis |
3. Complications - MRI Signs
These are the most clinically important reasons to image:
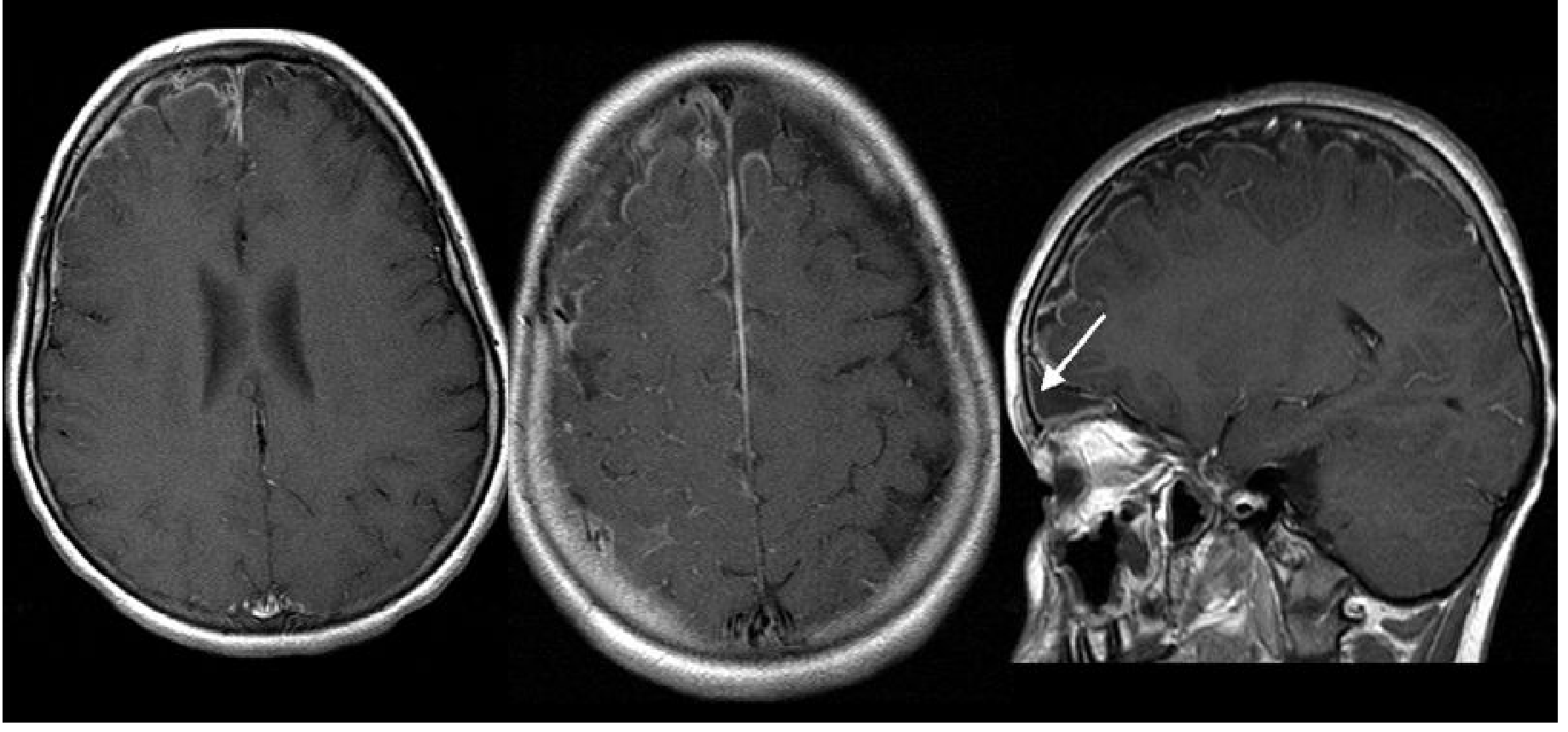
Left: pre-contrast T1 axial. Middle: post-contrast T1 axial. Right: post-contrast T1 sagittal (white arrow = meningeal/subdural enhancement in a meningitis complication) - Grainger & Allison's Diagnostic Radiology
| Complication | MRI Sign |
|---|---|
| Cerebritis | T2/FLAIR hyperintensity in cortex + white matter; gyral swelling; ill-defined enhancement |
| Brain abscess | Peripheral rim enhancement with central necrotic cavity (T1 dark, T2 bright); restricted diffusion in the core |
| Subdural effusion (sterile) | CSF-signal subdural collection, no enhancement |
| Subdural empyema | Intermediate T1 signal (protein-rich), restricted diffusion, pachymeningeal (dural) + leptomeningeal enhancement |
| Ventriculitis | Debris layered posteriorly in ventricles; ependymal T2 hyperintensity and contrast enhancement of the ependyma; can see intraventricular purulent material with DWI restriction |
| Hydrocephalus | Dilatation of ventricles - communicating type (blocked CSF absorption) most common; non-communicating if outlet foramina blocked |
| Infarction (arterial) | DWI restriction in large vessel territories OR perforator territories (basal ganglia, internal capsule) due to vasculitis of vessels traversing exudate |
| Venous sinus thrombosis | Loss of T2 flow void in sinus; expanded sinus; MRV filling defect; hemorrhagic venous infarct |
| Labyrinthitis ossificans (late) | T2 hypointensity in cochlear lumen post-meningitis |
4. Etiology-Specific Patterns
Bacterial (Pyogenic)
- Usually normal in uncomplicated cases
- When abnormal: thin smooth leptomeningeal enhancement, sulcal FLAIR signal
- Complications (empyema, abscess, ventriculitis) show restricted diffusion on DWI
- Infarcts in 30% of neonates - Grainger & Allison's Diagnostic Radiology
Tuberculous Meningitis
- Basal meningeal enhancement (interpeduncular cistern, middle cerebral artery cisterns) - hallmark
- Communicating hydrocephalus in 50% of adults, 85% of children
- Perforator territory infarcts (basal ganglia, internal capsule, brainstem)
- Tuberculomas: T1 low, T2 low (caseated) with rim or target-sign enhancement
- MRI superior to CT for basal enhancement, hydrocephalus, and infarcts
Fungal (Cryptococcus)
- Often unremarkable on MRI
- Gelatinous pseudocysts along Virchow-Robin spaces (basal ganglia, midbrain) - isointense to CSF, bilateral, symmetric
- Basal leptomeningeal enhancement when present
- Cryptococcomas = granulomas in basal ganglia, similar to tuberculomas
Carcinomatous / Chronic Meningitis
- Thick nodular leptomeningeal enhancement, often in basal cisterns
- More irregular vs. the thin smooth enhancement of acute infection
- Cranial nerve enhancement (follow nerves for thickening/signal)
Key Practical Points
- CE-FLAIR > CE-T1 for detecting leptomeningeal enhancement (suppresses background vascular signal)
- Normal MRI does not exclude meningitis - LP is required
- MRI before LP is indicated when: focal neurological signs, papilloedema, GCS <12, uncontrolled seizures
- DWI restriction in subarachnoid spaces = poor prognosis marker
- Basal enhancement + hydrocephalus + perforator infarcts = TB until proven otherwise
Sources: Grainger & Allison's Diagnostic Radiology; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; PMC Neuroimaging Review (2024); Medscape - Bacterial Meningitis Imaging
Cerebellar signs in tonsillar ectopia
Finding Sources
Finding Sources
Searching the Web
Chiari I malformation tonsillar ectopia cerebellar signs clinical features
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have everything needed for a thorough, well-referenced answer. Here it is:
Cerebellar Signs in Tonsillar Ectopia (Chiari I Malformation)
Overview
Tonsillar ectopia refers to caudal displacement of the cerebellar tonsils through the foramen magnum - the hallmark of Chiari I Malformation (CM-I). Diagnosis requires ≥5 mm of tonsillar descent below the foramen magnum in adults (age-adjusted thresholds apply - see table below). Despite striking imaging findings, many patients are entirely asymptomatic, and clinical severity correlates imperfectly with the degree of herniation.
The symptoms arise from three mechanisms:
- Compression of the cerebellar tonsils, caudal brainstem, and upper cervical cord at the foramen magnum
- Disruption of CSF flow dynamics at the craniocervical junction
- Syringomyelia from pressure-wave transmission into the central canal of the cord (in ~50-70% of symptomatic cases)
Age-Adjusted Normal Limits for Tonsillar Position
| Decade of Life | Upper Limit of Normal (below foramen magnum) |
|---|---|
| 1st (children) | 6 mm |
| 2nd - 3rd | 5 mm |
| 4th - 8th | 4 mm |
| 9th | 3 mm |
(Bradley & Daroff's Neurology, Table 104.5)
Cerebellar and Posterior Fossa Signs
1. Headache - "Chiari Headache"
The most common symptom. Characteristically:
- Suboccipital, pressing, continuous (waxing and waning, not episodic)
- May radiate behind the eyes or to the vertex
- Almost never hemicranial
- Triggered or worsened by Valsalva maneuvers - coughing, sneezing, laughing, straining, bearing down
- Exacerbations can be explosive rather than throbbing
2. Cerebellar Ataxia
- Gait ataxia with difficulty in tandem standing and walking
- Most typical finding on neurological exam: a vestibular-generated dysequilibrium
- Limb ataxia may be present but is less prominent than gait ataxia
- Favored by Chiari over syrinx as the cause: when ataxia is present alongside nystagmus - Adams & Victor's Principles of Neurology, 12th Ed.
3. Nystagmus - The Most Specific Ocular Sign
Tonsillar ectopia involves the vestibulocerebellum (flocculus, paraflocculus/tonsils, uvula, nodulus) and caudal medulla, explaining the rich array of eye movement abnormalities:
| Type | Notes |
|---|---|
| Downbeat nystagmus (DBN) | Hallmark - both spontaneous and positional; may have torsional component; worse on lateral gaze |
| Positional nystagmus | |
| Primary-position unidirectional horizontal nystagmus | |
| Periodic alternating nystagmus (PAN) | |
| Rebound nystagmus (including torsional rebound) | |
| Convergence nystagmus | |
| Divergence nystagmus / divergence paralysis |
Key caveat: Despite DBN being the "classic" finding, it is rarely seen even with tonsillar herniation as striking as 20 mm. Nystagmus is difficult to appreciate even with Fresnel lens examination - Bradley & Daroff's Neurology, 12th Ed.
Craniocervical anomalies (including tonsillar ectopia, platybasia, basilar invagination) are listed as a leading cause of downbeat nystagmus in the differential - Localization in Clinical Neurology, 8e.
4. Other Ocular Motor Abnormalities
From the vestibulocerebellar involvement:
- Impaired smooth pursuit (especially downward gaze)
- Impaired VOR cancellation
- Saccadic dysmetria (hypermetric or hypometric saccades)
- Skew deviation - accentuated or alternating on lateral gaze
- Internuclear ophthalmoplegia (INO)
- Square-wave jerks
5. Oscillopsia and Vestibular Symptoms
- Oscillopsia brought on or accentuated by head movements
- Dizziness and vertigo (75.8% prevalence in symptomatic CM-I vs 17-18% in tonsillar ectopia without CM-I criteria)
- Cervical pain with head movement
Long Tract and Brainstem Signs (When Medulla Descends)
When herniation is more severe and the medulla descends below the foramen magnum, additional signs emerge:
| System | Signs |
|---|---|
| Corticospinal | Spastic quadriparesis/paraparesis; prominent in lower limbs |
| Sensory | Sensory tract involvement in lower extremities |
| Cranial nerves (lower) | Dysphagia, hoarseness, palatal weakness (IX, X involvement) |
| Respiratory | Sleep-related breathing disorders, central apnea |
| Lower cranial nerve | Dysarthria, tongue wasting (if syringobulbia co-exists) |
| Sphincter | Bladder and bowel dysfunction (usually from syrinx) |
Syringomyelia Overlay (CM-I Associated)
When syringomyelia is present (the most common associated finding), additional signs include:
- Cape-like dissociated sensory loss (pain and temperature lost, light touch preserved) over shoulders and arms
- Wasting and weakness of the hands/upper limbs
- Painless burns or injuries to the hands (classic presentation)
- Segmental areflexia in upper limbs with hyperreflexia below
Clinical features that favor Chiari over syrinx as the dominant cause: nystagmus, cerebellar ataxia, head/neck pain, prominent corticospinal and sensory tract involvement in the lower extremities, hydrocephalus - Adams & Victor's Principles of Neurology, 12th Ed.
Special Points
- Children <3 years: vomiting and gastric reflux may be the sole manifestations
- Pediatric presentation: oropharyngeal dysfunction, scoliosis, failure to thrive
- Neurological exam is often completely normal - even with significant herniation
- Symptoms are typically exacerbated by any action that increases intrathoracic or intraabdominal pressure (Valsalva)
- At least a quarter of symptomatic patients first develop symptoms following minor head or neck injury
MRI Evaluation
- Best sequence: T2-weighted sagittal MRI of brain + cervical spine
- Assesses: tonsil position, posterior fossa volume, syrinx, brainstem compression
- Phase-contrast (cine) MRI: evaluates CSF flow at foramen magnum - pulsatile systolic tonsillar descent and obstruction of CSF flow are positive findings predictive of surgical response
- Dynamic MRI useful when clinical presentation is equivocal
Sources: Bradley & Daroff's Neurology in Clinical Practice, 8th Ed.; Adams & Victor's Principles of Neurology, 12th Ed.; Localization in Clinical Neurology, 8th Ed.; Radsource - Chiari I Malformation; JBSR 2023 - Cerebellar Tonsil Ectopia and Headache
Tests for cerebellar signs
Finding Sources
Finding Sources
Searching the Web
clinical examination tests cerebellar signs ataxia dysmetria assessment neurology
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Excellent - I now have comprehensive, structured textbook content. I have everything I need for a detailed answer.
Clinical Tests for Cerebellar Signs
The neurological examination of cerebellar function is organized across five domains: eyes, speech, hands, legs, and gait. The SARA scale (Scale for Assessment and Rating of Ataxia) formalizes eight of these into a validated clinical tool.
Mnemonic: DANISH
A useful aide-memoire for cerebellar signs:
| Letter | Sign |
|---|---|
| D | Dysdiadochokinesia |
| A | Ataxia (gait/truncal) |
| N | Nystagmus |
| I | Intention tremor |
| S | Slurred (scanning) speech |
| H | Hypotonia / past-pointing |
Domain 1: Gait and Stance
Normal Gait Observation
Ask the patient to walk normally. Look for:
- Variable stride length
- Veering to one side (toward the side of the lesion in unilateral disease)
- Wide-based gait - compensatory in moderate-severe ataxia
- Staggering, inability to maintain a straight line
Tandem (Heel-to-Toe) Walking
Most sensitive gait test for subtle ataxia. The patient walks placing one foot directly in front of the other. Swaying, stepping out, or falling indicates cerebellar dysfunction.
Single-leg Stance / Hopping
Reveals subtle balance deficits. Ask the patient to stand on each foot alternately, then hop. Inability disproportionate to lower limb weakness suggests cerebellar or vestibular pathology.
Detecting subtle difficulty: observe patients running or walking up/down stairs - these stress the system more than level walking - Bradley & Daroff's Neurology in Clinical Practice
Domain 2: Stance and Truncal Stability
Romberg's Test
- Stand with feet together, arms by sides
- First with eyes open, then eyes closed
- Positive Romberg = patient falls when eyes are closed but not open → implies proprioceptive or vestibular deficit (not pure cerebellum)
- Cerebellar lesion: patient is unsteady with both eyes open and closed (the cerebellum cannot integrate the remaining senses - it is a processing, not sensing, problem)
Balance requires input from proprioception, vestibular system, and vision. At least 2 are needed. Romberg removes vision. If the patient falls only with eyes closed, the cerebellar integration is intact but one of the other two systems is deficient - Shambaugh Surgery of the Ear
Sharpened (Tandem) Romberg
More sensitive. Patient stands with feet in tandem (heel-to-toe), arms folded across the chest. Normal healthy individuals can maintain this position for ≥30 seconds.
Sitting Without Back Support
Patients with truncal ataxia (vermis lesions) sway or cannot sit still without support.
Domain 3: Upper Limb (Hand) Tests
1. Finger-Nose-Finger Test (FNF)
The patient extends the arm and alternately touches:
- Their own nose
- The examiner's outstretched index finger
Performed at increasing speed. Look for:
- Intention tremor - oscillation that increases as the target is approached (pathognomonic of cerebellar disease)
- Past-pointing (dysmetria) - over- or undershooting the target
- Decomposition of movement - jerky, broken up action
- Perform with eyes open and then eyes closed (closed removes visual correction and exaggerates cerebellar dysmetria; worsening = cerebellar; remaining the same = proprioceptive problem)
2. Finger Chase Test
The patient's index finger follows the examiner's moving index finger as precisely as possible. Reveals over- or undershoot (dysmetria) and inability to smooth-track a moving target.
3. Dysdiadochokinesia Test (Rapid Alternating Movements)
Patient rapidly alternates pronation and supination of the hand, slapping the palm then the dorsum onto their own thigh (or the examiner's hand). Assess:
- Rate - normal is rapid and regular
- Rhythm - should be uniform
- Amplitude - should be consistent
Slow, irregular, or variable amplitude = dysdiadochokinesia. Reflects the cerebellar failure to switch agonist/antagonist muscle groups rhythmically.
4. Rebound Test (Stewart-Holmes Sign)
The examiner asks the patient to flex the elbow against resistance, then suddenly releases. Normally the patient arrests the movement rapidly (check reflex). In cerebellar disease, the arm rebounds and flies up, sometimes striking the patient's own face - failure of the check reflex due to absent antagonist muscle dampening.
5. Hyperdysmetria / Overshoot on Resistance
When moving a limb against resistance, sudden removal of resistance causes excessive overshoot. Reflects impaired dampening by the cerebellar system.
Domain 4: Lower Limb Tests
Heel-Shin Test
- Patient lies supine
- Lifts one leg, places the heel on the opposite knee, then slides it down the shin to the ankle
- Repeat several times, then with the other leg
The heel should track a straight line. In cerebellar ataxia, the heel deviates off the shin or oscillates laterally - the leg equivalent of the FNF test. Also reveals intention tremor in the lower limb.
Domain 5: Speech
Scanning/Staccato Speech
Ask the patient to speak in normal conversation and count from 1 to 10. Cerebellar speech is:
- Slow with irregular force and rhythm
- Unnecessary hesitations between words
- Words broken into separate syllables (scanning or syllabic speech)
- May sound explosive or slurred
- Distinct from dysarthria of upper/lower motor neuron origin
Domain 6: Eye Movement Examination
Eye movement abnormalities are often diagnostic and highly specific to cerebellar pathology:
| Test | What to Look For | Implication |
|---|---|---|
| Fixation | Square-wave jerks (small involuntary saccades breaking fixation) | Common in Friedreich ataxia |
| Smooth pursuit | Saccadic (cogwheel) pursuit instead of smooth tracking | Cerebellar hemisphere dysfunction |
| Saccades | Dysmetric (hypo- or hypermetric) saccades | Multiple ataxia types |
| Gaze-evoked nystagmus | Nystagmus in eccentric gaze (end-gaze) | Many cerebellar disorders |
| Downbeat nystagmus (DBN) | Fast phase beating downward, worse on lateral gaze | Cervicomedullary junction / flocculus |
| Rebound nystagmus | Nystagmus on returning to primary gaze after sustained lateral gaze | Cerebellar |
| VOR cancellation | Ask patient to fix on their own thumb while rotating in a chair - inability to suppress VOR | Flocculonodular lobe |
SARA Scale (Formal Clinical Rating)
| Domain | Test |
|---|---|
| 1 | Gait |
| 2 | Stance |
| 3 | Sitting |
| 4 | Speech disturbance |
| 5 | Finger chase |
| 6 | Nose-finger test |
| 7 | Fast alternating hand movements |
| 8 | Heel-shin slide |
Each scored 0-4 (0 = normal), total 0-40. Note: eye movements are not included in SARA and must be assessed separately.
Summary: Localizing Value
| Sign | Localization |
|---|---|
| Gait ataxia + truncal sway | Vermis / midline (e.g., alcohol, medulloblastoma) |
| Limb dysmetria (ipsilateral) | Cerebellar hemisphere (same side as lesion) |
| Intention tremor | Cerebellar outflow (dentate nucleus / superior cerebellar peduncle) |
| Downbeat nystagmus | Flocculus / cervicomedullary junction |
| Dysdiadochokinesia | Cerebellar hemisphere |
| Scanning speech | Vermis / bilateral hemispheres |
A key principle: cerebellar signs are ipsilateral to the lesion (unlike upper motor neuron signs which cross). The patient veers toward the side of the lesion. - Bradley & Daroff's Neurology in Clinical Practice
Sources: Bradley & Daroff's Neurology in Clinical Practice, 8th Ed. (SARA section); Shambaugh Surgery of the Ear; Medscape Neurological Examination; StatPearls - Cerebellar Dysfunction
This is a shared conversation. Sign in to Orris to start your own chat.