Peptic ulcer notes including pathophysiology and treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full notes.
Peptic Ulcer Disease (PUD) - Clinical Notes
1. Definition
A peptic ulcer is a break in the gastroduodenal mucosa extending through the muscularis mucosae, caused by the digestive action of acid and pepsin when mucosal defenses are overwhelmed. The name "peptic" is somewhat misleading - in the absence of acid, peptic ulcers do not occur, and nearly all can be healed with PPIs alone.
Common sites:
- First part of the duodenum (most common)
- Gastric antrum / lesser curvature (especially angularis incisura)
- Prepyloric region
- Lower esophagus (acid reflux context)
- Stoma following gastric surgery
- Meckel's diverticulum (ectopic gastric mucosa)
2. Epidemiology
- Prevalence ~2% in the US; lifetime cumulative prevalence ~10% (peaking around age 70)
- ~4 million individuals treated annually in the US
- Lifetime risk: ~10% males, ~4% females
- Duodenal ulcers (DU) > gastric ulcers (GU)
- GU: equal sex incidence, older patients, lower socioeconomic groups
- DU: historically more common in men, but gender gap narrowing as H. pylori rates fall
3. Pathophysiology
The central concept is an imbalance between aggressive and defensive forces on the gastroduodenal mucosa.
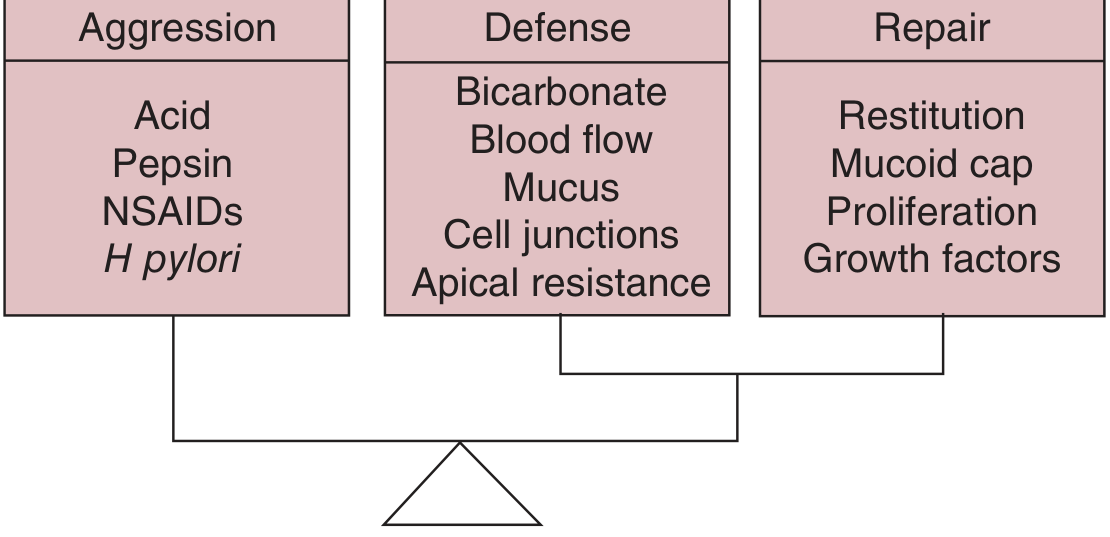
Aggressive vs. Defensive vs. Repair forces in the gastric mucosa (Schwartz's Principles of Surgery)
Aggressive Factors
| Factor | Mechanism |
|---|---|
| Hydrochloric acid | Direct mucosal injury; activates pepsinogen to pepsin |
| Pepsin | Proteolytic enzyme causing tissue breakdown |
| H. pylori | Disrupts mucosal barrier; stimulates acid secretion |
| NSAIDs/Aspirin | Inhibit COX-1 -> prostaglandin depletion -> reduced mucus/bicarbonate/blood flow |
| Bile salts | Duodenogastric reflux weakens gastric mucosal defenses |
Defensive Mechanisms
- Mucus layer - physical barrier secreted by surface cells
- Bicarbonate secretion - from surface epithelial cells, Brunner's glands, pancreatic juice
- Mucosal blood flow - delivers O2, removes H+
- Tight cell junctions and apical resistance - prevent back-diffusion of H+
- Prostaglandins (PGE2, PGI2) - stimulate mucus/bicarbonate, inhibit acid secretion
- Epithelial restitution - rapid replacement of damaged cells
Repair Mechanisms
- Restitution, mucoid cap formation, epithelial proliferation, growth factors (EGF, TGF-alpha)
4. Etiology
A. Helicobacter pylori (Major Cause)
- Implicated in >70% of PUD cases overall; up to 90% of DU
- Gram-negative, microaerophilic spiral rod residing in the mucus layer
- Mechanisms of injury:
- Urease produces ammonia -> direct mucosal toxicity and raises local pH, disrupting mucosal integrity
- Cytotoxins (VacA, CagA) cause epithelial damage and inflammation
- Triggers gastric acid hypersecretion via stimulation of gastrin and inhibition of somatostatin
- Induces chronic active gastritis -> breaks down mucosal barrier
- Only 5-10% of infected individuals develop ulcers - host factors and bacterial strain virulence also matter
- H. pylori eradication dramatically reduces recurrence rates
B. NSAIDs / Aspirin (Second Major Cause)
- Inhibit cyclooxygenase (COX-1 predominantly) -> reduced synthesis of PGE2 and PGI2
- Loss of prostaglandins leads to:
- Decreased mucus production
- Decreased bicarbonate secretion
- Reduced mucosal blood flow
- Increased susceptibility to acid back-diffusion
- Direct topical irritation also occurs (especially with aspirin)
- COX-2 selective inhibitors (coxibs) reduce GI events by ~50% vs. non-selective NSAIDs
- Misoprostol (PGE1 analogue) can partially compensate for NSAID-induced prostaglandin depletion
C. Acid Hypersecretion
- Zollinger-Ellison Syndrome (ZES): Gastrin-secreting pancreatic/duodenal tumour (gastrinoma) -> massive acid hypersecretion -> multiple, refractory ulcers in unusual locations (distal duodenum, jejunum)
- Antral G-cell hyperfunction/hyperplasia
- Systemic mastocytosis - histamine stimulates parietal cells
D. Other Contributing Factors
| Factor | Effect |
|---|---|
| Cigarette smoking | Reduces mucosal blood flow, impairs healing, increases relapse rate |
| High-dose corticosteroids | Suppress prostaglandin synthesis |
| Alcohol | Direct mucosal irritant |
| Hypercalcemia (renal failure, hyperparathyroidism) | Stimulates gastrin production |
| Alcohol-related cirrhosis, COPD, chronic renal failure | All associated with increased PUD risk |
Gastric Ulcer Classification (Johnson-Modified)
| Type | Location | Acid Secretion | Association |
|---|---|---|---|
| I | Lesser curve near angularis incisura | Normal or low | Most common |
| II | Body of stomach + active DU | Normal/elevated | |
| III | Prepyloric | Normal/elevated | Treated like DU surgically |
| IV | Near GE junction | Normal or low | |
| V | Anywhere in stomach | Variable | NSAID-induced |
5. Pathology (Macroscopic & Microscopic)
Macroscopic:
- Ulcer base appears punched out with smooth, well-demarcated edges
- DU: usually <1 cm, in the first part of the duodenum
- GU: tend to be larger, located at lesser curve / incisura; "kissing ulcers" (anterior + posterior DU) may occur
- Fibrosis and scarring can cause pyloric stenosis or "hourglass" stomach deformity
- Chronic ulcers penetrate the muscularis into and sometimes beyond the wall
Microscopic:
- Active phase: fibrinopurulent necrotic exudate at base, granulation tissue beneath, fibrosis in deepest layer
- Granulation tissue and endarteritis obliterans visible at base
- Healing: re-epithelialization can be mistaken for neoplastic invasion
Endoscopic view of a duodenal ulcer:
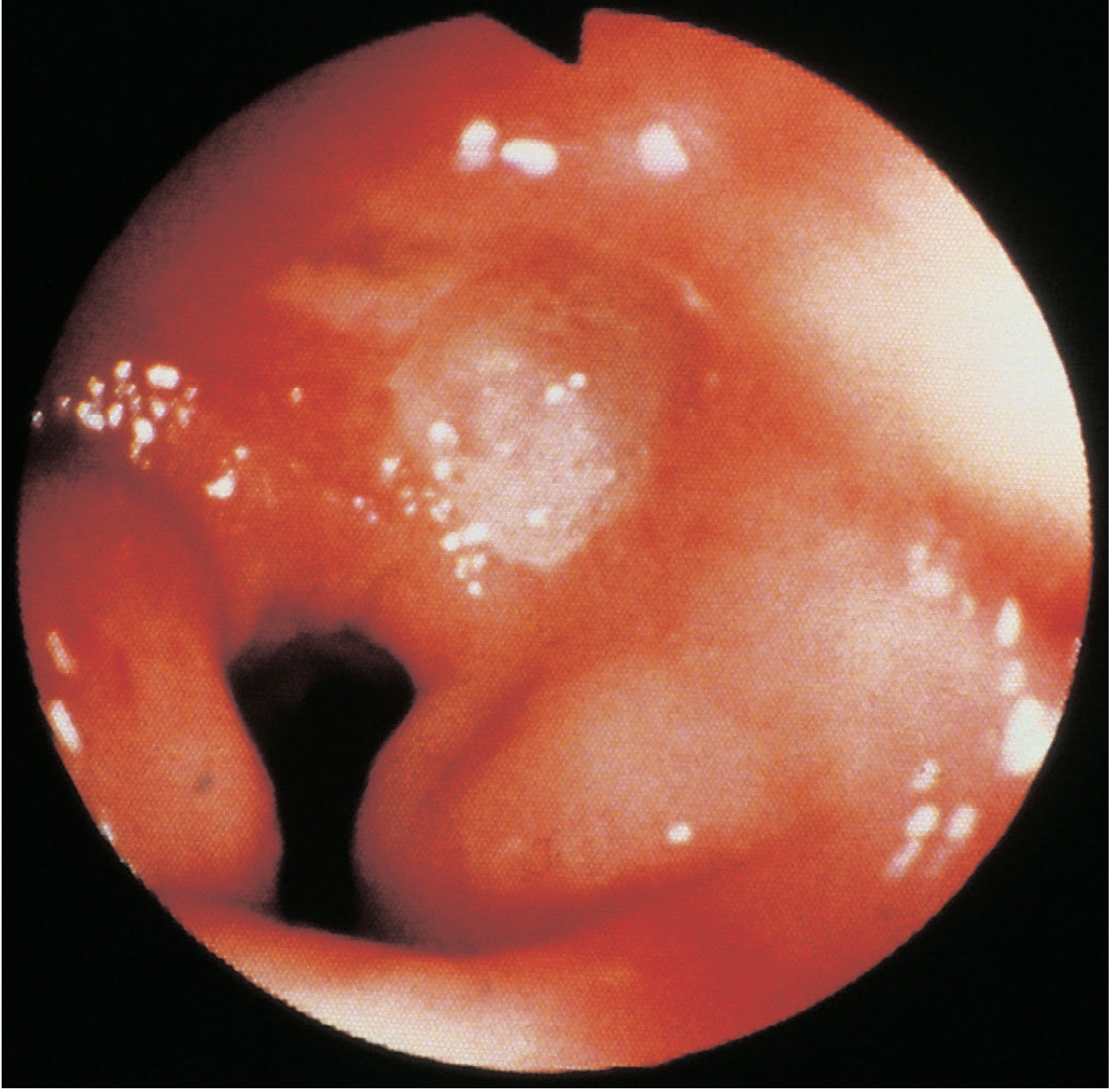
Duodenal ulcer at gastroduodenoscopy - Bailey & Love's Short Practice of Surgery
6. Clinical Features
Symptoms
- Epigastric pain - gnawing or burning; may radiate to the back (especially posterior DU eroding pancreas)
- DU: Pain classically relieved by food and antacids; occurs 2-3 hours after meals and at night ("hunger pain")
- GU: Pain may be precipitated by eating (fear of eating -> weight loss)
- Periodicity: symptoms come and go over weeks/months - related to spontaneous ulcer healing
- Nausea, bloating, vomiting (prominent if gastric outlet obstruction)
- Chronic bleeding -> microcytic (iron-deficiency) anaemia
Signs
- Epigastric tenderness on palpation
- Succussion splash if gastric outlet obstruction is present
- Signs of complications (see below)
7. Investigations
Diagnosing PUD
- Upper GI endoscopy (OGD): Gold standard; allows direct visualization, biopsy, and H. pylori testing
- ALL gastric ulcers must be biopsied (minimum 6-10 biopsies) - rule out malignancy
- Duodenal ulcers very rarely malignant
- Barium meal: "Niche" sign; less used now (superseded by endoscopy)
Testing for H. pylori
| Test | Notes |
|---|---|
| Urea breath test (UBT) | Non-invasive; gold standard for non-endoscopic testing; avoid if recent PPI/antibiotics |
| Stool antigen test | Reliable; avoid within 2 weeks of antibiotics or 2 weeks of PPIs |
| Rapid urease test (CLO test) | Done at endoscopy on biopsy |
| Histology | Biopsy at endoscopy; identifies organism and grades gastritis |
| Serology (IgG) | High sensitivity but cannot distinguish active vs. past infection; not useful post-treatment |
Ruling Out Gastrinoma
- Fasting serum gastrin level - if >1000 pg/mL with gastric pH <2, highly suggestive of ZES
- Secretin stimulation test - paradoxical gastrin rise is diagnostic
- Indicated when: H. pylori-negative, NSAID-negative, unusual ulcer location, multiple/refractory ulcers
8. Complications
The three main complications in order of frequency: Bleeding > Perforation > Obstruction
A. Bleeding (Most Common)
- Bleeding peptic ulcers are the most common cause of upper GI bleeding requiring hospitalization
- Posterior DU classically erodes the gastroduodenal artery
- Presentation: haematemesis, melena, haemodynamic instability
- Forrest classification guides endoscopic management (Ia: spurting; Ib: oozing; IIa: visible vessel; IIb: adherent clot; IIc: flat spot; III: clean base)
- Blatchford score (pre-endoscopy): predicts need for intervention
- Rockall score (post-endoscopy): predicts rebleeding and mortality
- Management: resuscitation + urgent endoscopy + haemostasis (injection adrenaline, thermal coagulation, clips) + PPI infusion post-endoscopy + H. pylori eradication
B. Perforation
- Anterior DU most commonly perforates into the peritoneal cavity
- Presents with sudden severe epigastric pain, rigid abdomen, free air under diaphragm on erect CXR
- Emergency surgery: closure with omental patch (Graham patch)
- Conservative management (Taylor's method) in selected patients who have sealed spontaneously
C. Gastric Outlet Obstruction (Pyloric Stenosis)
- Results from fibrosis and scarring of a DU or pyloric channel ulcer
- Presents with recurrent vomiting (non-bile stained), succussion splash, weight loss, metabolic alkalosis (hypochloraemic, hypokalaemic)
- Treatment: correct metabolic derangements first, then endoscopic balloon dilatation or surgery
9. Treatment
A. Lifestyle Modifications
- Stop smoking (reduces mucosal blood flow and delays healing)
- Avoid NSAIDs and aspirin if possible
- Limit alcohol
- Dietary modification (avoid foods that trigger symptoms)
B. Medical Treatment
1. Acid Suppression
Proton Pump Inhibitors (PPIs) - First-line
- Mechanism: irreversibly inhibit H+/K+-ATPase (proton pump) on the parietal cell
- Drugs: omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole
- Superior to H2 blockers in healing rate and symptom relief
- Standard dose for 4-8 weeks heals most DU; 8 weeks for GU
- For NSAID-related ulcers: continue PPI while NSAID cannot be stopped
H2-Receptor Antagonists - Second-line (less used now)
- Mechanism: competitive blockade of histamine H2 receptors on parietal cells
- Drugs: ranitidine (withdrawn many markets due to NDMA), famotidine, cimetidine
- Less potent than PPIs; some tachyphylaxis develops
Vonoprazan (Potassium-competitive acid blocker, PCAB)
- Newer class; blocks the K+-binding site of the proton pump; acid suppression is faster and more sustained than PPIs
- Recent meta-analysis (2024, PMID: 39294424) confirms non-inferiority to PPIs for ulcer treatment and prevention, with possible advantages in H. pylori eradication regimens
2. H. pylori Eradication Therapy
Eradication dramatically reduces recurrence (from ~80% to <5% at 1 year):
Standard Triple Therapy (7-14 days):
- PPI (standard dose BD) + Clarithromycin 500 mg BD + Amoxicillin 1 g BD
- Eradication rate ~70-85% (declining due to clarithromycin resistance)
Bismuth Quadruple Therapy (where clarithromycin resistance is high):
- Bismuth subcitrate + Metronidazole + Tetracycline + PPI (14 days)
- Eradication rate >90%
Concomitant Therapy (all 4 drugs simultaneously):
- PPI + Clarithromycin + Amoxicillin + Metronidazole (14 days)
Sequential Therapy:
- PPI + Amoxicillin (5 days) -> PPI + Clarithromycin + Metronidazole (5 days)
Confirm eradication with urea breath test or stool antigen at least 4 weeks after completing antibiotics (avoid PPIs 2 weeks before testing).
3. Cytoprotective Agents
- Misoprostol (PGE1 analogue): Replaces prostaglandins; used for prevention of NSAID-induced ulcers in high-risk patients; side effects: diarrhoea, abdominal cramps
- Sucralfate: Forms a physical barrier over the ulcer base; binds to proteins in necrotic tissue; effective but requires multiple daily doses
- Bismuth compounds: Cytoprotective + anti-H. pylori activity
4. PPI Prophylaxis for NSAID Users
- Indicated in patients with: prior ulcer, age >65, high-dose NSAIDs, concurrent corticosteroids or anticoagulants
- A 2025 Cochrane review (PMID: 40337979) confirms PPIs effectively prevent NSAID-induced ulcers and dyspepsia
- COX-2 selective inhibitors (e.g. celecoxib) as an alternative to non-selective NSAIDs where cardiovascular risk allows
C. Surgical Treatment
Elective surgery for PUD is now very rarely performed - reserved for:
- Failure of medical therapy
- Ulcers failing to heal after multiple courses with confirmed H. pylori eradication
- Complications requiring emergency surgery (perforation, uncontrolled bleeding)
Historical procedures for DU (now rarely performed electively):
| Procedure | Description | Notes |
|---|---|---|
| Billroth I gastrectomy | Resect distal stomach, anastomose to duodenum | |
| Billroth II (Polya) gastrectomy | Resect 2/3 stomach, close duodenum, anastomose stomach to jejunum | |
| Truncal vagotomy + drainage | Vagotomy reduces acid; drainage procedure (pyloroplasty or gastroenterostomy) needed to prevent gastroparesis | |
| Highly selective vagotomy (HSV) | Divide vagal fibres to acid-secreting corpus only; preserves antral innervation - no drainage needed | Lowest side-effect profile; now virtually obsolete |
Post-gastrectomy complications: dumping syndrome (early/late), afferent loop syndrome, bile reflux gastritis, malabsorption, weight loss, anastomotic ulceration.
10. Refractory Ulcers
An ulcer failing to heal after 8-12 weeks of appropriate therapy. Approach:
- Confirm NSAID cessation; check compliance
- Confirm H. pylori eradication with repeat biopsy or breath test
- Culture and sensitivity to guide re-eradication
- Measure fasting serum gastrin - rule out ZES
- Consider rare causes: Crohn's disease, cytomegalovirus, tuberculosis, lymphoma
- Consider IgG4-related disease (rare)
11. Gastric Ulcers - Key Points vs. Duodenal Ulcers
| Feature | Gastric Ulcer | Duodenal Ulcer |
|---|---|---|
| Acid secretion | Normal or low (Type I/IV) | Often elevated |
| Malignancy risk | Yes - all GU must be biopsied | Virtually nil |
| Pain pattern | Worsened by eating | Relieved by eating |
| Age | Older | Younger |
| Sex | Equal | More in men (historically) |
| Confirm healing | Mandatory repeat endoscopy | Not required |
12. Special Situations
Zollinger-Ellison Syndrome: Long-term high-dose PPI; surgery for tumour if localisable (often part of MEN-1).
PUD in Pregnancy: Symptoms often improve (progesterone may reduce gastric acid); PPIs generally avoided in first trimester if possible; antacids and sucralfate preferred.
Stress Ulcers (Curling's ulcer - burns; Cushing's ulcer - head injury):
- Cushing's ulcer: due to vagal stimulation from raised ICP causing acid hypersecretion
- Curling's ulcer: ischaemia/reduced mucosal blood flow
- ICU prophylaxis: PPI or H2 blocker in at-risk patients (mechanical ventilation, coagulopathy)
Sources:
- Schwartz's Principles of Surgery, 11th Ed. - Pathophysiology and Etiology, Medical & Surgical Treatment
- Bailey and Love's Short Practice of Surgery, 28th Ed. - Clinical features, Pathology, Treatment
- Robbins & Kumar Basic Pathology - Pathogenesis, Epidemiology
- Guyton & Hall Textbook of Medical Physiology - Basic mechanisms, mucosal defense
- Recent evidence: Vonoprazan vs. PPIs (Dig Dis Sci 2024, PMID 39294424); PPI prevention of NSAID ulcers (Cochrane 2025, PMID 40337979)
This is a shared conversation. Sign in to Orris to start your own chat.