explain in detail transcient ischemic stroke in detail
Reading File
search_medical_text
transient ischemic attack TIA definition pathophysiology etiology
search_medical_text
TIA clinical features diagnosis ABCD2 score workup management treatment
search_medical_image
transient ischemic attack TIA brain MRI DWI imaging
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive, detailed explanation of Transient Ischemic Attack (TIA).
Transient Ischemic Attack (TIA)
1. Definition
Historically, TIA was defined as focal neurological symptoms resolving within 24 hours of onset. This time-based definition was revised by the AHA/ASA in 2009 to a tissue-based definition:
"A transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction."
This shift was driven by evidence that ~1/3 of all TIAs show signs of true infarction on neuroimaging, making the 24-hour cutoff insufficient. Most TIAs last fewer than 1–2 hours. If imaging is unavailable and symptoms last more than 24 hours, the episode is classified as a clinical stroke.
(Adult Patients With Suspected TIA in the Emergency Department, p. 2)
2. Pathophysiology
TIA results from transient focal ischemia — a temporary reduction in cerebral blood flow severe enough to impair neuronal function but not cause permanent infarction. The underlying mechanisms include:
A. Thromboembolism (most common)
- A clot (thrombus or embolus) temporarily occludes a cerebral artery, then spontaneously dissolves before permanent tissue death.
- Sources:
- Cardiac emboli (atrial fibrillation, valvular disease, intracardiac thrombus)
- Artery-to-artery emboli (atherosclerotic plaques, especially at the carotid bifurcation)
B. Small Vessel Occlusion (Lacunar TIA)
- Lipohyalinosis or microatheroma occludes small penetrating arteries (lenticulostriate, basilar perforators).
- Strongly associated with hypertension and diabetes.
C. Hemodynamic TIA
- Systemic hypoperfusion (e.g., cardiac failure, severe hypotension) in the setting of pre-existing stenosis.
- Often causes stereotyped, repetitive symptoms triggered by positional changes.
D. Rare Causes
- Hypercoagulable states (antiphospholipid syndrome, thrombophilias)
- Vasculitis (SLE, giant cell arteritis)
- Hematologic disorders (polycythemia vera, sickle cell disease)
- Cervical artery dissection (carotid or vertebral)
3. Risk Factors
| Modifiable | Non-Modifiable |
|---|---|
| Hypertension | Age (risk doubles each decade after 55) |
| Atrial fibrillation | Male sex |
| Diabetes mellitus | Race (Black > White) |
| Hyperlipidemia | Family history / genetics |
| Smoking | Prior TIA or stroke |
| Obesity & physical inactivity | |
| Carotid artery stenosis | |
| Heavy alcohol use |
4. Clinical Features
Symptoms are sudden in onset, focal, and transient — they should be negative (loss of function), not positive (e.g., not tingling/jerking from seizure).
By Vascular Territory:
Anterior Circulation (Carotid Territory — MCA/ACA)
- Contralateral limb weakness or sensory loss (face, arm, leg)
- Aphasia (dominant hemisphere)
- Amaurosis fugax — transient monocular visual loss ("curtain coming down") from ophthalmic artery ischemia
- Hemineglect (non-dominant hemisphere)
Posterior Circulation (Vertebrobasilar Territory — PCA, PICA, AICA)
- Vertigo, nausea, vomiting
- Diplopia or other cranial nerve palsies
- Dysarthria, dysphagia
- Bilateral or crossed weakness/sensory loss
- Cerebellar ataxia
- Homonymous hemianopia
- "Drop attacks" — sudden loss of postural tone without LOC
Key rule: Isolated vertigo, isolated diplopia, or isolated syncope are generally NOT sufficient for TIA diagnosis unless accompanied by other brainstem/cerebellar signs.
5. Differential Diagnosis
TIA is a clinical diagnosis of exclusion. Mimics must be ruled out:
| Condition | Distinguishing Features |
|---|---|
| Focal seizure (Todd's paralysis) | Positive symptoms (jerking), postictal phase |
| Hypoglycemia | BG < 60 mg/dL; resolves with glucose |
| Complex migraine with aura | Slow "march" of symptoms, headache follows |
| Multiple sclerosis | Prior episodes, MRI white matter lesions |
| Brain tumor | Progressive course, papilledema |
| Vestibular neuritis | Pure prolonged vertigo without other focal signs |
| Hemiplegic migraine | Family history, prolonged aura |
| Functional neurological disorder | Variable, inconsistent exam |
6. Diagnostic Workup
TIA is a neurological emergency — the highest stroke risk is in the first 48 hours.
Immediate Assessment
| Test | Purpose |
|---|---|
| Blood glucose | Exclude hypoglycemia |
| CBC, coagulation (PT/INR, aPTT) | Hematologic causes |
| BMP / electrolytes | Metabolic mimics |
| ECG | Detect atrial fibrillation |
| Cardiac troponin | Rule out concomitant ACS |
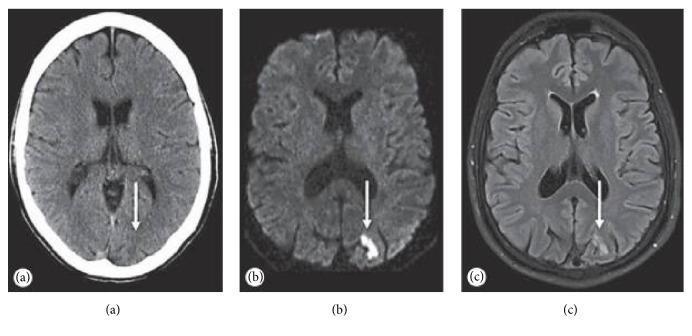
Neuroimaging
MRI with DWI is the gold standard:
- DWI (Diffusion-Weighted Imaging) — detects acute ischemia within minutes; reveals small cortical/subcortical infarcts that confirm the event was ischemic.
- CT is insensitive for early ischemic change but useful to rule out hemorrhage if MRI is unavailable.
- FLAIR — shows established infarcts; less sensitive than DWI in the acute phase.
Vascular Imaging
- CT Angiography (CTA) or MR Angiography (MRA) of the head and neck — to evaluate for carotid stenosis, intracranial stenosis, vertebrobasilar disease, dissection.
- Carotid Doppler ultrasound — widely available, evaluates carotid bifurcation.
Cardiac Workup
- Echocardiography (TTE or TEE) — detects intracardiac thrombus, PFO, valvular disease, cardiomyopathy.
- Prolonged cardiac monitoring (Holter/event monitor/implantable loop recorder) — detects paroxysmal atrial fibrillation, especially in cryptogenic TIA.
7. Risk Stratification: The ABCD² Score
Used to estimate short-term stroke risk after TIA (2–7 day risk):
| Feature | Criteria | Points |
|---|---|---|
| Age | ≥ 60 years | 1 |
| Blood Pressure | Systolic ≥ 140 or Diastolic ≥ 90 mmHg | 1 |
| Clinical Features | Unilateral weakness | 2 |
| Speech disturbance without weakness | 1 | |
| Duration | ≥ 60 minutes | 2 |
| 10–59 minutes | 1 | |
| Diabetes | Present | 1 |
| Total | 0–7 |
| Score | Risk Category | 2-day stroke risk |
|---|---|---|
| 0–3 | Low | ~1% |
| 4–5 | Moderate | ~4% |
| 6–7 | High | ~8% |
Important caveat: Studies show the ABCD² score has modest discriminatory accuracy when used alone. The AHA/ACC recommends urgent neurovascular workup for ALL TIA patients, regardless of ABCD² score, given the risk that any patient may progress to stroke. (p. 5)
8. Management
Acute Phase (Emergency Department / Hospital)
Antiplatelet Therapy (non-cardioembolic TIA)
- Dual antiplatelet therapy (DAPT): Aspirin + Clopidogrel for 21 days, then transition to single antiplatelet (aspirin or clopidogrel alone).
- Evidence: POINT and CHANCE trials showed DAPT significantly reduced stroke risk at 90 days vs. aspirin alone in high-risk TIA/minor stroke.
- Aspirin 160–325 mg loading dose if clopidogrel not available.
Anticoagulation (cardioembolic TIA — e.g., AF)
- Direct oral anticoagulants (DOACs) — apixaban, rivaroxaban, or dabigatran preferred over warfarin for non-valvular AF.
- Warfarin — for valvular AF or mechanical heart valves.
- Timing depends on infarct size and bleeding risk.
Blood Pressure Management
- Do not aggressively lower BP acutely in the first 24–48 hours unless hypertensive emergency.
- Long-term target: < 130/80 mmHg (AHA 2019 guidelines).
Statin Therapy
- High-intensity statin (atorvastatin 40–80 mg or rosuvastatin 20–40 mg) started immediately regardless of baseline LDL.
- Evidence: SPARCL trial showed atorvastatin 80 mg reduced recurrent stroke/TIA.
Surgical/Interventional Management
| Indication | Intervention |
|---|---|
| Symptomatic carotid stenosis ≥ 70% | Carotid endarterectomy (CEA) — preferred within 2 weeks |
| Stenosis 50–69% | CEA may be beneficial depending on patient factors |
| < 50% stenosis | Medical management only |
| High surgical risk | Carotid artery stenting (CAS) |
Secondary Prevention (Long-term)
- Antiplatelet or anticoagulation (depending on mechanism)
- Aggressive BP control
- Statin therapy
- Glycemic control in diabetics
- Smoking cessation
- Weight loss, exercise, dietary modification
- Closure of PFO in selected patients (< 60 years, cryptogenic TIA/stroke, large shunt on echo)
9. Prognosis
- Short-term stroke risk is highest in the first 48 hours:
- ~3–10% risk of stroke within 2 days
- ~9–17% risk within 90 days
- TIA is a strong predictor of future stroke — it is sometimes called a "warning stroke."
- With rapid, aggressive management (urgent workup + secondary prevention), the 90-day stroke risk can be reduced by up to 80% (EXPRESS and SOS-TIA studies).
- Patients with DWI-positive TIA (i.e., small infarct on MRI) have a higher risk of early recurrent stroke than DWI-negative TIA.
10. Special Populations
Pediatric TIA
- Rare; causes differ — sickle cell disease, congenital heart disease, prothrombotic states, moyamoya disease.
- Workup is broader (including metabolic and genetic studies).
Pregnancy
- Increased risk due to hypercoagulable state, peripartum cardiomyopathy, eclampsia.
- MRI preferred (no radiation); anticoagulation with LMWH if needed (DOACs are contraindicated).
Elderly (> 80 years)
- Higher risk of AF as underlying etiology.
- Risk-benefit analysis of anticoagulation must account for fall risk and bleeding tendency.
Summary Table
| Aspect | Key Points |
|---|---|
| Definition | Transient focal neurological dysfunction from ischemia, no infarction on imaging |
| Duration | Usually < 1–2 hours; up to 24 hours by clinical definition |
| Mechanism | Thromboembolism, small vessel disease, hemodynamic, rare causes |
| Imaging | MRI DWI is gold standard; CT rules out hemorrhage |
| Risk Score | ABCD² (0–7); all patients need urgent workup |
| Treatment | DAPT (non-cardioembolic) or anticoagulation (AF), high-intensity statin, BP control |
| Surgery | CEA for symptomatic stenosis ≥ 70%, ideally within 2 weeks |
| Prognosis | 3–10% stroke risk at 2 days; treatable with rapid intervention |
Bottom line: TIA is a neurological emergency that requires immediate evaluation and treatment. It is the strongest predictor of imminent ischemic stroke, but also represents a critical therapeutic window — rapid workup and aggressive secondary prevention can dramatically reduce the risk of a disabling stroke.
This is a shared conversation. Sign in to Orris to start your own chat.