Does Jogren's syndrome come under the classification of rheumatoid arthritis, or is it a separate entity?
Sjögren syndrome classification separate entity or rheumatoid arthritis
Sjögren's Syndrome: A Separate Entity (Not a Subtype of RA)
The Primary vs. Secondary Distinction
| Primary Sjögren's | Secondary Sjögren's | |
|---|---|---|
| Definition | Stands alone with no associated connective tissue disease | Occurs alongside another autoimmune disease |
| Associated conditions | None | RA, SLE, polymyositis, systemic sclerosis, biliary cirrhosis |
| Antibodies | Anti-Ro/SS-A and Anti-La/SS-B common | May share serologies with the underlying disease |
"Secondary Sjogren's syndrome… is defined by the presence of either keratoconjunctivitis sicca (dry eyes) or xerostomia (dry mouth) in association with another connective tissue disease, such as RA. Approximately 10% of patients with RA have secondary Sjogren's syndrome." — Harrison's Principles of Internal Medicine 22E, p. 2920
Where It Fits in Classification
Why the Confusion Arises
- Overlap: ~50% of Sjögren's patients have a co-existing rheumatic condition (often RA), and ~10% of RA patients develop secondary Sjögren's.
- Shared features: Both cause arthritis, fatigue, and positive RF/ANA; Sjögren's patients can develop non-erosive arthritis.
- Historical links: Before formal classification criteria, the two were often conflated.
Core Features That Distinguish Sjögren's from RA
| Feature | Sjögren's Disease | Rheumatoid Arthritis |
|---|---|---|
| Hallmark | Sicca (dry eyes + dry mouth) due to exocrine gland destruction | Symmetric erosive synovitis |
| Target tissue | Lacrimal & salivary glands (lymphocytic infiltration) | Synovial membrane |
| Key antibodies | Anti-Ro/SS-A, Anti-La/SS-B | Anti-CCP, RF |
| Joint damage | Non-erosive arthritis | Erosive, deforming arthritis |
| Pathology | T-cell mediated exocrine gland destruction | Pannus formation, cartilage erosion |
| Lymphoma risk | Elevated (~44× for B-cell NHL) | Not significantly elevated |
Bottom Line

Rf 302
ANA Profile Interpretation — Shameem M Thaha, 65F
Key Positive Results
| Antibody | Result | Significance |
|---|---|---|
| SS-A (Ro-52 kDa) | Strong positive +++ | Highly specific for Sjögren's disease |
| SS-B (La) | Strong positive +++ | Highly specific for Sjögren's disease |
| SS-A (60 kDa / native Ro) | Borderline positive | Additional Sjögren's marker |
| DFS70 | Strong positive +++ | See note below |
Clinical Interpretation
-
Anti-Ro/SS-A and anti-La/SS-B are the hallmark autoantibodies of Sjögren's syndrome. They are found in the majority of primary Sjögren's cases. A strong positive +++ for both is highly significant."Diagnosis is strongly supported by positive serologic testing for anti-Ro (SS-A) and anti-La (SS-B) antibodies." — Harrison's Principles of Internal Medicine 22E
-
Ro-52 specifically is a distinct antigen from Ro-60 (SS-A 60kDa). Ro-52 positivity is also associated with antisynthetase syndrome / inflammatory myopathies (dermatomyositis, polymyositis), so clinical correlation is essential. However, in combination with strong SS-B positivity, Sjögren's is the dominant diagnosis.
-
The absence of dsDNA, Sm, Scl-70, Jo-1, Centromere B effectively rules out SLE, scleroderma, and myositis as primary diagnoses.
Note on DFS70 Strong Positive +++
- Isolated high-titer anti-DFS70 (without other SARD antibodies) is actually considered a marker that argues against a systemic autoimmune rheumatic disease (SARD).
- However, in this patient, DFS70 is not isolated — it co-exists with strong SS-A and SS-B positivity. Therefore, the DFS70 positivity here is not reassuring and does not negate the Sjögren's pattern.
What to Do Next (Clinical Correlation)
- Sicca symptoms — dry eyes (keratoconjunctivitis sicca) and dry mouth (xerostomia)?
- Schirmer's test — tear flow measurement
- Rose Bengal / Lissamine Green staining — corneal/conjunctival damage
- Minor salivary gland biopsy — gold standard (focal lymphocytic infiltration, focus score ≥1)
- Parotid gland enlargement on examination
- RF and ESR — often elevated in Sjögren's
- Renal function — tubular acidosis is a known renal manifestation
The ACR/EULAR 2016 Classification Criteria score SS-A/Ro positivity as +3 points (out of a threshold of ≥4) — this patient already has a high pre-test probability based on serology alone.
Can this be rheumatoid arthritis
Can This ANA Profile Be Rheumatoid Arthritis?
Why This Profile Does NOT Point to RA
| Marker | This Patient | Expected in RA |
|---|---|---|
| Anti-CCP | Negative | Positive (most specific for RA, ~95% specific) |
| Rheumatoid Factor (RF) | Not shown in this panel | Elevated in ~70–80% of RA |
| SS-B (La) | Strong positive +++ | Negative in RA |
| SS-A (Ro-52) | Strong positive +++ | Negative in RA |
| dsDNA, Sm, Scl-70 | Negative | Negative (as expected) |
"The distinction between primary Sjögren's syndrome and rheumatoid arthritis may be difficult; the absence of rheumatoid factor and anti-CCP antibodies, and the absence of erosions on radiographs would favour SS over rheumatoid arthritis." — Fitzpatrick's Dermatology
"A patient with morning stiffness, deforming arthritis, high-titer anti-CCP antibodies, and UIP will be given a diagnosis of rheumatoid arthritis." — Fishman's Pulmonary Diseases
The Overlap Scenario
- In RA, the primary serological markers are anti-CCP and RF — both absent here
- In secondary Sjögren's with RA, you would expect to see anti-CCP/RF positivity in addition to SS-A/SS-B
- This patient has only SS-A and SS-B positive — pointing to primary Sjögren's, not RA
What Would Help Distinguish
- Anti-CCP antibody — most specific test for RA (not included in this ANA panel)
- Serum Rheumatoid Factor (RF) — often positive in both RA and Sjögren's, so less discriminating
- Hand X-rays — erosive joint changes with periarticular osteopenia = RA; non-erosive = Sjögren's
- Clinical joint exam — symmetric small joint synovitis (MCP/PIP) favours RA; non-deforming arthralgia favours Sjögren's
Sjogrens syndrome clinical features
Sjögren's Syndrome — Clinical Features
A. Glandular (Sicca) Manifestations
1. Oral (Xerostomia) — most common
- Difficulty swallowing dry food
- Burning sensation in the mouth
- Increased dental caries (loss of protective saliva)
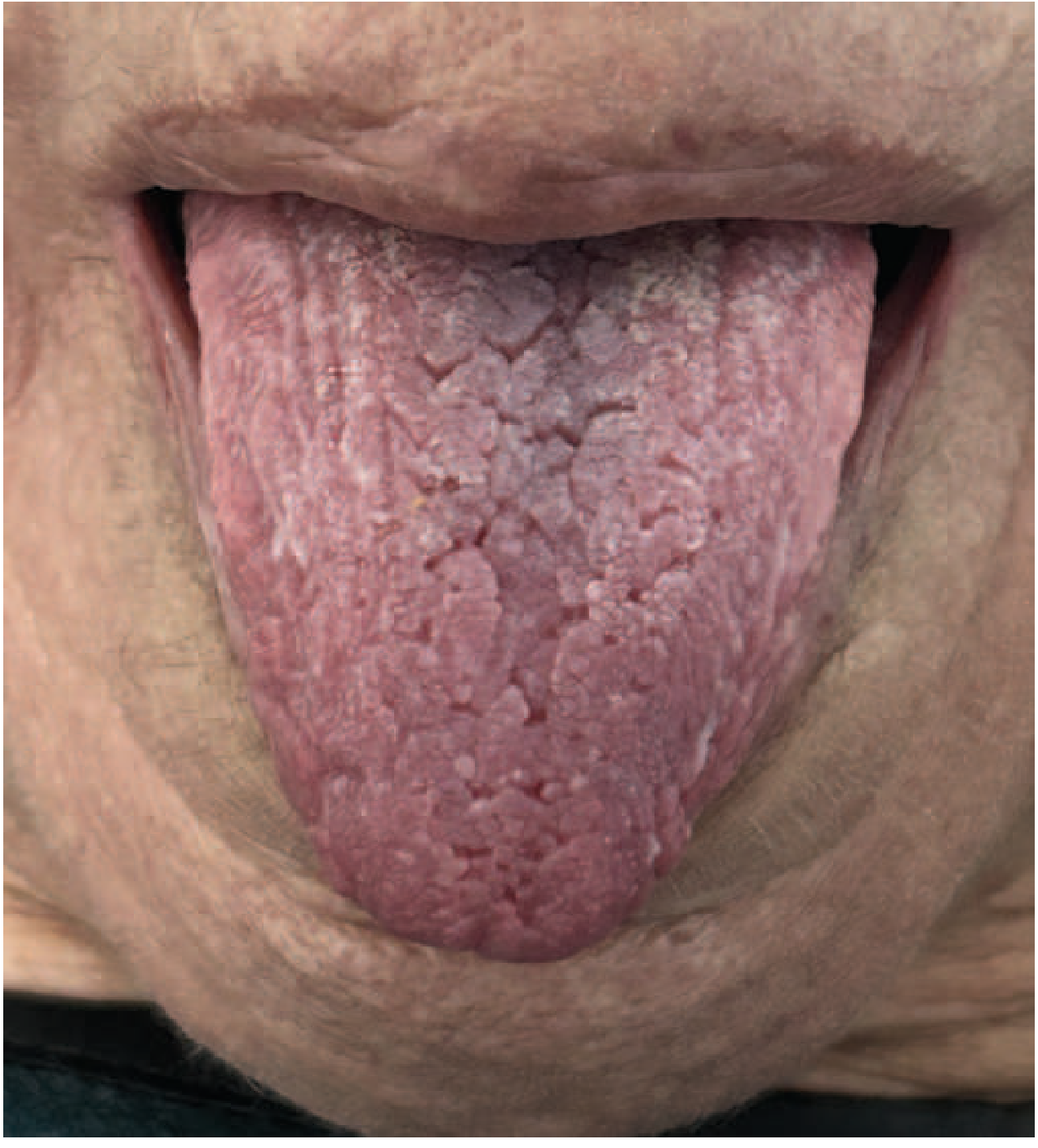
- Atrophic tongue with deep fissuring (see image above)
- Dry, sticky, erythematous oral mucosa
- Parotid/salivary gland enlargement in ~2/3 of patients (intermittent or persistent)
2. Ocular (Keratoconjunctivitis Sicca)
- Sandy/gritty sensation under eyelids
- Burning, itching, redness, photosensitivity
- Decreased tearing
- Thick secretions at inner canthi
- Corneal and conjunctival ulcerations on Rose Bengal/lissamine green staining
3. Other Exocrine Glands
- Respiratory tract: Dry nose, throat, trachea (xerotrachea) → dry cough
- GI tract: Esophageal dysmotility, atrophic gastritis
- Genitalia: Vaginal dryness → dyspareunia (in premenopausal women)
- Skin: Dry skin
B. Extraglandular (Systemic) Manifestations
| Category | Manifestation | Prevalence |
|---|---|---|
| Nonspecific | Fatigue, myalgias, fibromyalgia | 25% |
| Arthralgias/non-erosive arthritis | 60% | |
| Raynaud's phenomenon | 37% (precedes sicca in 1/3) | |
| Low-grade fever | — | |
| Periepithelial | Interstitial lung disease (dry cough, lymphocytic pneumonitis) | 14% |
| Interstitial nephritis (renal tubular acidosis, hyposthenuria) | 9% | |
| Liver involvement (primary biliary cholangitis stage I) | 6% | |
| Immune complex-mediated | Small vessel vasculitis → purpura, urticarial rash | 9% |
| Peripheral neuropathy (sensory or sensorimotor) | 2% | |
| Membranoproliferative glomerulonephritis | 2% | |
| Mononeuritis multiplex | Rare | |
| Lymphoma | MALT B-cell lymphoma (glandular) | 6% |
"Sjögren's disease is characterized by the highest risk for lymphoma development among all autoimmune diseases." — Harrison's Principles of Internal Medicine 22E
C. Key Points to Remember
| Feature | Detail |
|---|---|
| Arthritis | Non-erosive (never deforming/destructive — unlike RA) |
| Renal tubular acidosis | Type I (distal) → untreated may lead to nephrocalcinosis |
| CNS involvement | Rare; myelitis with anti-aquaporin-4 antibodies described |
| Lymphoma type | MALT marginal zone B-cell lymphoma — most common; arises in salivary/lacrimal glands |
| Lymphoma risk | ~44× increased risk for non-Hodgkin lymphoma vs. general population |
D. Red Flags Suggesting Lymphoma Transformation
- Rapid, persistent parotid enlargement
- Lymphadenopathy
- Splenomegaly
- Falling complement (C3/C4) levels
- Cryoglobulinemia
- Monoclonal immunoglobulin on serum protein electrophoresis
Does Sjogren's syndrome come under arthritis?
Classification of Sjögren's Syndrome
Where It Sits in the Disease Hierarchy
Autoimmune / Rheumatic Diseases
│
├── Inflammatory Arthritis
│ ├── Rheumatoid Arthritis
│ ├── Psoriatic Arthritis
│ └── Ankylosing Spondylitis
│
└── Systemic Connective Tissue Diseases ← Sjögren's is HERE
├── Systemic Lupus Erythematosus (SLE)
├── Sjögren's Syndrome / Disease ✓
├── Systemic Sclerosis (Scleroderma)
├── Polymyositis / Dermatomyositis
└── Mixed Connective Tissue Disease
Why the Confusion Exists
| Reason | Explanation |
|---|---|
| Both are managed by rheumatologists | Sjögren's falls under the rheumatology specialty, alongside arthritis |
| Arthritis occurs in Sjögren's | ~60% of patients develop arthralgias/non-erosive arthritis as an extraglandular feature |
| Secondary Sjögren's overlaps with RA | ~10% of RA patients develop Sjögren's as a co-existing condition |
| Both are autoimmune | Shared immunological mechanisms cause confusion |
The Critical Distinction
| Feature | Sjögren's Syndrome | Rheumatoid Arthritis |
|---|---|---|
| Primary target | Exocrine glands (salivary, lacrimal) | Synovium of joints |
| Hallmark | Dry eyes + dry mouth (sicca) | Erosive, symmetric synovitis |
| Arthritis type | Non-erosive, non-deforming | Erosive, deforming |
| Key antibodies | Anti-Ro/SS-A, Anti-La/SS-B | Anti-CCP, RF |
| Unique complication | B-cell lymphoma (MALT) | Joint destruction, subluxation |
Bottom Line
Will rheumatoid factor be elevated in Sjogren's syndrome?
RF in Sjögren's Syndrome
Prevalence
| Autoantibody | Prevalence in Primary Sjögren's |
|---|---|
| Anti-SS-A/Ro | 60–75% |
| Anti-SS-B/La | 25–50% |
| Rheumatoid Factor (RF) | ~70% |
| Anti-α-fodrin | 40–70% |
Why RF Is Elevated in Sjögren's
The Critical Clinical Point: RF Does NOT Diagnose RA
| Situation | Interpretation |
|---|---|
| RF positive + anti-CCP positive + erosive arthritis | Rheumatoid Arthritis |
| RF positive + SS-A/SS-B positive + sicca symptoms | Primary Sjögren's syndrome |
| RF positive alone | Non-specific — seen in RA, Sjögren's, SLE, chronic infections (TB, hepatitis C), healthy elderly |
RF positivity in Sjögren's is part of a picture of polyclonal B-cell hyperactivity, not a marker of joint disease.
What This Means for Your Patient (Shameem, 65F)
I Can a patient have anti-CCP positive, SSB and SSA strongly positive, and RA factor high all at the same time?
What This Combination Means: Secondary Sjögren's Syndrome with RA
"Secondary Sjögren syndrome refers to the disease in patients who have the characteristic signs and symptoms of primary Sjögren syndrome associated with another autoimmune disease such as rheumatoid arthritis." — Cummings Otolaryngology
"The most common eye manifestation of rheumatoid arthritis is keratoconjunctivitis sicca (dry eyes) from secondary Sjögren syndrome." — Goldman-Cecil Medicine
How to Interpret Each Marker in This Overlap
| Marker | In This Combination | What It Tells You |
|---|---|---|
| Anti-CCP positive | Confirms RA as the primary diagnosis | Most specific marker for RA (~95% specific) |
| RF high | Present in both RA (80%) and Sjögren's (70%) | Non-discriminating here; confirms seropositive disease |
| SS-A/SS-B strongly positive | Confirms Sjögren's co-existing | Not seen in RA alone — their presence means Sjögren's is also present |
"IgM RF is found in 80% of RA patients and may also be seen in other autoimmune diseases (SLE, Sjögren's syndrome). When considering RA, both serum RF and anti-CCP should be obtained as these are complementary." — Harrison's 22E
The Clinical Scenario
Anti-CCP +ve → RA is present
SS-A +++ / SS-B +++ → Sjögren's is also present
High RF → Seropositive disease (supports both)
Clinical Implication
- Joint features: Symmetric erosive synovitis of small joints (from RA)
- Sicca features: Dry eyes, dry mouth, parotid enlargement (from Sjögren's)
- Higher disease severity: Double positivity (anti-CCP + RF) in RA predicts more aggressive, erosive joint disease
- Lymphoma vigilance: Sjögren's component carries elevated B-cell lymphoma risk regardless of co-existing RA
What is the earliest sign or symptom or a feature of B-cell lymphoma which can be identified so that it can treatment can be started as soon as possible before it gets worse in a patient with Sjogren's syndrome?
"Sjogren syndrome" AND lymphoma AND "early detection"
"Sjogren syndrome" AND lymphoma AND "predictors"
Early Warning Signs of B-Cell Lymphoma in Sjögren's Syndrome
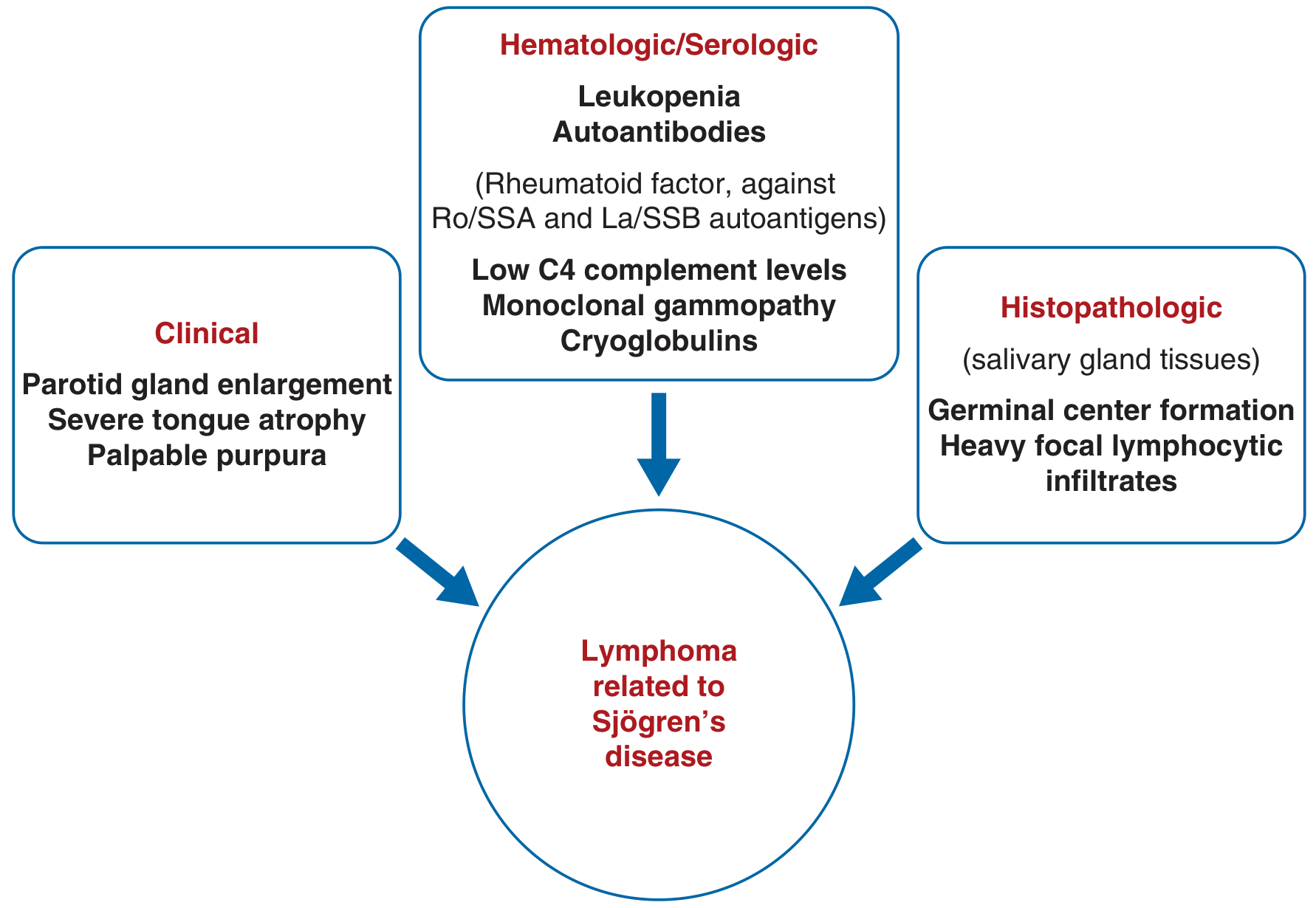
1. Clinical Red Flags (What You Can See/Feel)
⚠️ Persistent Parotid Gland Enlargement — THE Most Important Early Sign
- In Sjögren's, parotid enlargement is common and usually benign
- When it becomes persistent, unilateral, rapidly growing, or firm/hard, it signals possible MALT lymphoma arising within the parotid
- "Patients with persistent unilateral or bilateral parotid gland enlargement are at higher risk for the development of lymphoma." — Cummings Otolaryngology
- MRI is the most sensitive tool for detecting MALT lymphoma in Sjögren's patients (K.J. Lee's Otolaryngology)
- Biopsy should be performed on any solid mass in a Sjögren's patient
⚠️ Palpable Purpura
- Non-blanching, small vessel vasculitic lesions on the lower limbs
- Reflects immune complex deposition / cryoglobulinemia
- A very strong early predictor: "Patients with palpable purpura, low C4, and mixed monoclonal cryoglobulinemia are at higher risk for lymphoma." — Andrews' Diseases of the Skin
⚠️ Severe Tongue Atrophy
- Progressive, marked atrophy beyond typical xerostomia
🔴 B Symptoms (indicate established/advanced lymphoma)
- Fever, drenching night sweats, unexplained weight loss >10% in 6 months
- "Survival rates are decreased in patients with B symptoms, lymph node mass >7 cm in diameter, and high/intermediate histologic grade." — Harrison's 22E
2. Laboratory/Serological Red Flags (Earliest Detectable Changes)
| Lab Finding | Why It Matters |
|---|---|
| Falling C4 complement (low C4) | Earliest serological warning — reflects immune complex consumption; strongly associated with lymphoma risk |
| Mixed monoclonal cryoglobulinemia | Monoclonal B-cell expansion — the direct precursor step to lymphomagenesis |
| Monoclonal gammopathy on serum protein electrophoresis (SPEP) | Shift from polyclonal → oligoclonal → monoclonal Ig = B-cell clonal transformation underway |
| Leukopenia / lymphopenia | Bone marrow infiltration by lymphoma cells |
| Rising RF with falling complement | Combined marker of immune complex disease + B-cell hyperactivation |
Goldman-Cecil explains the progression: "The evolution of lymphoma is initiated by a polyclonal B lymphocyte response, with expansion of oligoclonal and monoclonal B lymphocyte populations followed by clonal transformation."
3. Histopathological Warning Signs (On Salivary Gland Biopsy)
- Germinal centre formation within salivary gland tissue
- Heavy focal lymphocytic infiltrates (high focus score)
- These precede overt lymphoma — biopsy at regular intervals is recommended
Surveillance Protocol Summary
| When | What to Do |
|---|---|
| Every visit | Examine for parotid enlargement, purpura, lymphadenopathy, splenomegaly |
| Every 6–12 months | Serum C4, full blood count, serum protein electrophoresis (SPEP), cryoglobulins |
| Any new hard parotid mass | Urgent MRI parotid → biopsy |
| Falling C4 + monoclonal band | FDG-PET/CT scan to exclude/locate lymphoma |
Key Takeaway
- 🥇 Falling C4 complement — first laboratory signal, precedes symptoms
- 🥈 Monoclonal band on SPEP / cryoglobulinemia — clonal B-cell shift
- 🥉 Persistent, hard, enlarging parotid mass — first clinical sign
- Palpable purpura — strong clinical predictor of lymphoma risk
Patient is 90 percent of the time on bed due to fbss, how to detect early signs/ symptoms of heart failure ..... 69 yr old female , ht 154cm, wt 69 kg, any other dangerous complications due to this ?
Patient Profile
PART 1: Early Signs & Symptoms of Heart Failure to Watch For
🔴 Earliest / Most Sensitive Symptoms (Ask Every Visit)
| Symptom | What to Ask / Look For | Why It Matters |
|---|---|---|
| Dyspnea at rest | "Do you feel breathless just lying in bed?" | Dyspnoea on exertion is 84% sensitive for HF — in bedridden patients, rest dyspnea takes its place |
| Orthopnoea | "How many pillows do you sleep with? Has it increased?" | Can't lie flat → fluid redistribution to lungs when supine; most specific symptom (84%) |
| Paroxysmal Nocturnal Dyspnoea (PND) | "Do you wake up suddenly at night gasping or feeling suffocated?" | Highly specific for HF — fluid re-distributes from legs to lungs during sleep |
| Ankle/leg swelling | Inspect both legs and ankles daily — press the shin for pitting oedema | Dependent oedema from fluid retention; in bedridden patients, check sacral area and lower back too (fluid pools posteriorly) |
| Weight gain | Weigh daily, same time, same clothing | >1 kg in 24 hrs or >2 kg in a week = fluid retention alarm |
| Fatigue, reduced alertness | More tired than usual? Less responsive? | Low cardiac output → reduced cerebral perfusion |
| Abdominal bloating, nausea, loss of appetite | Right-sided HF → hepatic congestion → GI symptoms | Often mistaken for other causes in elderly |
| Cough, especially at night | "Do you cough when lying flat?" | Pulmonary oedema causes nocturnal cough — easily missed in an FBSS patient already in pain |
| Reduced urine output | Is she passing less urine than usual? | Renal hypoperfusion — pre-renal component of HF |
🔴 Physical Signs (Caregiver/Nurse to Check)
| Sign | How to Check | Significance |
|---|---|---|
| Sacral oedema | Press firmly over sacrum — pitting = fluid | In bedridden patients, fluid settles posteriorly, NOT in ankles |
| Raised JVP | Look at neck veins — distension >4 cm above sternal angle while sitting at 45° | Elevated jugular venous pressure = right heart failure |
| S3 gallop | Auscultation — low-pitched sound after S2 | Highest positive likelihood ratio for HF (4.0) — Tintinalli's Emergency Medicine |
| Bi-basal lung crackles | Auscultate lung bases | Pulmonary oedema |
| Cold peripheries + low BP | Feel hands/feet; check BP | Low output state |
🔴 Simple Home Monitoring Tools
- Daily weight chart — the single most practical early warning tool
- Pulse oximetry (SpO₂) — if SpO₂ drops below 94% at rest → urgent review
- Blood pressure monitoring — sudden drop or rise, especially with new symptoms
- BNP/NT-proBNP blood test — if levels rise on serial testing, HF is developing even before symptoms appear
PART 2: Other Dangerous Complications of Near-Total Immobility in This Patient
1. 🩸 Deep Vein Thrombosis (DVT) → Pulmonary Embolism (PE) — MOST DANGEROUS
"Immobility (general, limb, or neurologic)" is listed as a primary risk factor for DVT — Rosen's Emergency Medicine
- Unilateral calf swelling, warmth, tenderness
- Pain in the calf on dorsiflexion of foot (Homan's sign — not reliable alone)
- Sudden breathlessness, pleuritic chest pain, coughing blood, rapid heart rate, oxygen desaturation
- Can be rapidly fatal — this is the #1 killer in immobile patients
2. 🛏️ Pressure Ulcers (Decubitus Ulcers)
- Sites to check daily: sacrum, heels, greater trochanters, occiput, shoulder blades
- Early sign: non-blanching redness (Stage I) → if missed → deep tissue necrosis, osteomyelitis, sepsis
- Prevention: 2-hourly repositioning, pressure-relieving mattress, adequate protein nutrition
3. 🫁 Hypostatic/Aspiration Pneumonia
"Prolonged bed rest and inactivity contribute to postoperative respiratory complications... FRC decreases by 500–1000 mL moving from upright to supine." — Fishman's Pulmonary Diseases
- Secretions pool in dependent lung zones → bacterial overgrowth
- Early signs: new cough, low-grade fever, increased sputum, reduced SpO₂
- Prevention: Deep breathing exercises, incentive spirometry, head-of-bed elevation 30°
4. 💪 Muscle Atrophy & Contractures
- Disuse atrophy begins within 48–72 hours of immobility
- Joint contractures (especially hips, knees) develop within weeks
- Once established, very difficult to reverse
- Prevention: Daily passive and active physiotherapy
5. 🧠 Delirium / Cognitive Decline
- Immobility + chronic pain + social isolation → accelerated cognitive decline in elderly
- Delirium is a medical emergency in elderly patients
- Watch for: sudden confusion, agitation, fluctuating alertness — especially at night
6. 🦴 Osteoporosis & Fragility Fractures
- Weight-bearing is essential for bone density
- BMI 29 is protective to some extent, but prolonged immobility overrides this
- Hip fractures in bedridden elderly carry 30% 1-year mortality
- Monitor: DEXA scan, calcium and vitamin D supplementation
7. 🍽️ Malnutrition & Sarcopenic Obesity
- BMI 29 does not mean well-nourished — she may have "sarcopenic obesity" (high fat, low muscle)
- Chronic pain reduces appetite; NSAIDs/opioids used in FBSS cause GI side effects
- Assess: serum albumin, prealbumin, MUST score
8. 🚽 Urinary Tract Infections & Urinary Retention
- Recumbent position impairs bladder emptying
- Very common in elderly immobile females
- Watch for: cloudy urine, dysuria, new onset confusion (UTI presents as delirium in elderly)
Summary: Priority Action Plan for This Patient
| Priority | Action |
|---|---|
| 1 (Urgent) | DVT prophylaxis — LMWH, compression stockings |
| 2 (Daily) | Weight monitoring, SpO₂, sacral/heel skin checks |
| 3 (Weekly) | BP, pulse, lung auscultation for early HF |
| 4 (Regular) | BNP/NT-proBNP, D-dimer if DVT suspected |
| 5 (Ongoing) | Physiotherapy — even passive range-of-motion exercises |
| 6 (Nutrition) | High-protein diet, Vitamin D + Calcium supplementation |
Create an Anki card for [Chronic inflammation, Morphology of cells involved in chronic inflammation, tissue resident macrophage, macrophage activation, the classical and alternatively activated macrophage, functions of these cells, granulomatous inflammation, which includes granuloma, the components of granuloma, pathogenesis, granulomatous disorders that include infective and non-infective etiology, tuberculosis, its clinical presentation, signs, lab findings, non-infective causes which include sarcoidosis, the granuloma formed here, its clinical presentation, lab findings, the systemic effects of inflammation and acute phase reactants, the positive ones and the negative ones. Positive means the ones that have increased during inflammation, negative means the ones that decrease during inflammation. Just the name, no need of explanation. ] for NEET PG 2027 exam (pathology focus). Output a downloadable .txt file with exactly one line in this format: Front[TAB]Back. The Front should contain only the topic name. The Back should contain a comprehensive summary covering 100% of exam-relevant content, formatted using HTML bold tags for section headings and <br><br> between sections for spacing and readability. Do not use any newlines, pipes, or semicolons in the file — only commas, colons, dashes, and HTML tags. Confirm the file is exactly 1 line using wc -l before delivering it.
chronic inflammation anki
Text File · TXT
How to Import into Anki
- Open Anki → File → Import
- Select the downloaded
.txtfile - Set: Field separator: Tab, Allow HTML in fields: Yes
- Map Field 1 → Front, Field 2 → Back
- Click Import
What's covered in the card (all 18 sections):
| Section | Content |
|---|---|
| Chronic Inflammation - Definition | Duration, coexistence of injury and repair |
| Causes | Persistent infection, hypersensitivity, toxic agents |
| Morphologic Features | Mononuclear infiltrate, tissue destruction, fibrosis |
| Cells Involved | Macrophages, lymphocytes, plasma cells, eosinophils |
| Tissue Resident Macrophages | Embryonic vs. BM origin, Kupffer, microglia, osteoclasts etc. |
| M1 - Classical Activation | IFN-gamma, TNF, NF-kB, iNOS, ROS, killing functions |
| M2 - Alternative Activation | IL-4/IL-13, TGF-beta, repair, fibrosis |
| Macrophage General Functions | 5 key functions |
| Lymphocytes in Chronic Inflammation | Th1, Th2, Th17 subsets and cytokines |
| Granuloma - Definition and Components | Epithelioid cells, Langhans/foreign body giant cells, caseous necrosis |
| Granuloma Pathogenesis | Step-by-step T cell - macrophage cascade |
| Infective Causes of Granuloma | TB, leprosy, syphilis, fungi, parasites |
| TB - Granuloma, Ghon complex, Ranke complex | Caseating granuloma details |
| TB - Clinical, Signs, Labs | Full coverage including ZN stain, Mantoux, IGRA, ADA |
| Non-infective Granulomatous Disorders | Sarcoidosis, Crohn, berylliosis, Wegener etc. |
| Sarcoidosis - Granuloma, Clinical, Syndromes | Lofgren, Heerfordt, lupus pernio, ACE, Kveim, BHL staging |
| Sarcoidosis - Labs | ACE, hypercalcemia, CD4:CD8 ratio, Panda/Lambda signs |
| Acute Phase Reactants | Positive (CRP, fibrinogen, ferritin, haptoglobin etc.) and Negative (albumin, transferrin, prealbumin etc.) |