Paragonimus lung disease for md exams 10 marks answer from fishman and murray only
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from both Fishman's and Murray & Nadel's. Let me compile the full 10-mark answer.
Paragonimiasis (Lung Fluke Disease)
[Sources: Fishman's Pulmonary Diseases and Disorders, Chapter 136 | Murray & Nadel's Textbook of Respiratory Medicine, Chapter 58]
1. Etiology and Epidemiology
Paragonimiasis is caused by lung flukes (trematodes) of the genus Paragonimus, with more than 15 species implicated in human disease. Paragonimus westermani is the principal species found in humans and animals across Asia, Africa, and South America - more than 90% of cases occur in Asia. The disease accounts for over 20 million infections globally. P. kellicotti causes autochthonous disease in North America, linked to freshwater crayfish ingestion.
(Fishman's, p. 2427; Murray & Nadel's, p. 1347)
2. Life Cycle and Transmission
The parasite has a complex life cycle involving two intermediate hosts - freshwater snails and crustaceans - and mammalian definitive hosts (humans, felids, canids, rodents, pigs).
Transmission: Humans are infected by eating raw, undercooked, or pickled freshwater crustaceans (crabs, crayfish) containing encysted metacercariae. Infection from wild game meat (boar, deer) is also reported.
Lifecycle sequence:
- Metacercariae excyst in the duodenum and penetrate the intestinal wall
- Larvae migrate from the peritoneal cavity, through the diaphragm, into the pleural space
- They penetrate lung parenchyma, tunneling from the periphery toward the bronchioles
- Adult worms (reddish-brown, hermaphroditic) mature inside cystic cavities near bronchial passages, living in pairs
- They produce golden-brown, operculated eggs (~100 x 55 µm) that are coughed up in sputum or swallowed and shed in feces
- Eggs hatch in the environment and continue the cycle through snails and crustaceans
(Fishman's, p. 2427-2428; Murray & Nadel's, p. 1347)
3. Pathogenesis and Pathology
Pathology correlates with three disease stages:
Stage 1 - Migration: Worms tunnel through pleural cavity and lung, inducing inflammation, hemorrhage, and tissue necrosis. Surrounding neutrophilic and eosinophilic inflammation with Charcot-Leyden crystals is seen along the migration tracks.
Stage 2 - Encystation: Worms encyst in the lungs, forming clusters of encapsulated cysts that communicate with each other or the bronchi, forming fistulas that allow egg entry into the airways. Histopathology shows adult worms within fibrous cysts communicating with bronchi; granulomas may contain eggs at the center.
Stage 3 - Death: Cyst collapses on worm death, leading to fibrosis or calcification.
Ectopic migration: Flukes may spread outside the lungs - most commonly to the CNS (presenting as eosinophilic meningitis or ring-enhancing mass lesions), abdominal viscera, and skin.
(Fishman's, p. 2428; Murray & Nadel's, p. 1347-1348)
4. Clinical Manifestations
Acute Phase (weeks 2-16 post-ingestion):
Non-specific prodrome of fever, diarrhea, abdominal pain, cough, urticaria, and peripheral eosinophilia. Elevated IgE is seen. Most acute infections are asymptomatic.
Established Pulmonary Infection (chronic):
- Cough productive of thick, rusty-colored or blood-tinged sputum containing parasite eggs, necrotic material, and Charcot-Leyden crystals
- Hemoptysis - can resemble tuberculosis (a key diagnostic mimic)
- Pleuritic chest pain
- Peripheral eosinophilia in 45-80% of cases - a key discriminating feature from TB and malignancy
- Clinical presentation may resemble chronic bronchitis or bronchiectasis
- After 5-10 years, fever and eosinophilia often absent; abnormal chest radiograph in an asymptomatic patient is a common finding
Extrapulmonary Disease (up to 25% of hospitalized patients):
- CNS paragonimiasis: headaches, vision changes, seizures, eosinophilic meningitis, ring-enhancing mass lesions
- Skin (migratory subcutaneous nodules)
- Abdominal viscera
(Fishman's, p. 2428; Murray & Nadel's, p. 1347-1348)
5. Radiological Features
Chest X-ray:
- Early: non-specific opacities or normal in up to 20% of cases
- Lobar consolidations
- Cavitary lesions up to 4 cm in diameter
- Small cysts, calcified or non-calcified nodules
- Pleural effusion, pneumothorax, and pleural thickening (minority of patients)
- Hilar enlargement
CT Chest - Classic finding:
- "Ring sign": subpleural nodule with central necrosis or surrounding ground-glass opacity
- Linear opacities extending to the pleural surface (worm migration tracks)
(Fishman's, p. 2428-2429; Murray & Nadel's, p. 1348)
6. Pleural Involvement
Pleural paragonimiasis presents as a chronic illness with a concomitant parenchymal opacity in ~50% of patients. The pleural fluid is highly characteristic:
- Exudative with elevated protein and LDH (LDH >3x upper limit of normal)
- Glucose < 10 mg/dL (strikingly low)
- pH < 7.10
- High percentage of eosinophils
- Cholesterol crystals or chyle may also be present
- Usually no ova in the pleural fluid
This combination of low pH + low glucose + eosinophilia in pleural fluid is seen in only two conditions: paragonimiasis and eosinophilic granulomatosis with polyangiitis (Churg-Strauss).
(Murray & Nadel's, p. 2538-2539)
7. Diagnosis
Direct microscopy (gold standard):
- Demonstrate characteristic operculated eggs in sputum, feces, BAL, or tissue biopsy
- Bloody sputum has the highest yield
- Multiple samples required - yield of a single sputum or stool specimen is <40%
- Gastric aspirates and pleural fluid can also be examined
Serology:
- ELISA and immunoblot (Western blot) assays detect antibodies to Paragonimus antigens - sensitivity >90% for P. westermani
- Complement fixation titer >1:8 for P. westermani is strongly suggestive of diagnosis
- A CDC-developed immunoblot specific for P. kellicotti antigens is preferred for North American cases
Molecular: PCR and multiplex protein microarrays are in development.
(Fishman's, p. 2429; Murray & Nadel's, p. 1348)
8. Treatment
| Drug | Dose | Duration |
|---|---|---|
| Praziquantel (drug of choice) | 25 mg/kg three times daily | 2-3 days |
| Triclabendazole (alternative) | 5 mg/kg/day OR 20 mg/kg divided in 2 doses | 3 days OR 1 day |
- Symptoms improve rapidly after treatment
- Clearance of eggs from sputum and radiographic resolution may take weeks to months
- Recurrent pleuropulmonary disease may require a second course
- CNS disease: add corticosteroids to blunt inflammatory response to dying worms
- Untreated pulmonary paragonimiasis may resolve within 5-10 years (life span of adult worms), but chronic infection may be accompanied by extensive fibrosis
- Prevention: avoid eating uncooked crabs and crayfish
(Fishman's, p. 2429; Murray & Nadel's, p. 1348)
Key Images
Figure 58.4 from Murray & Nadel's - P. westermani:
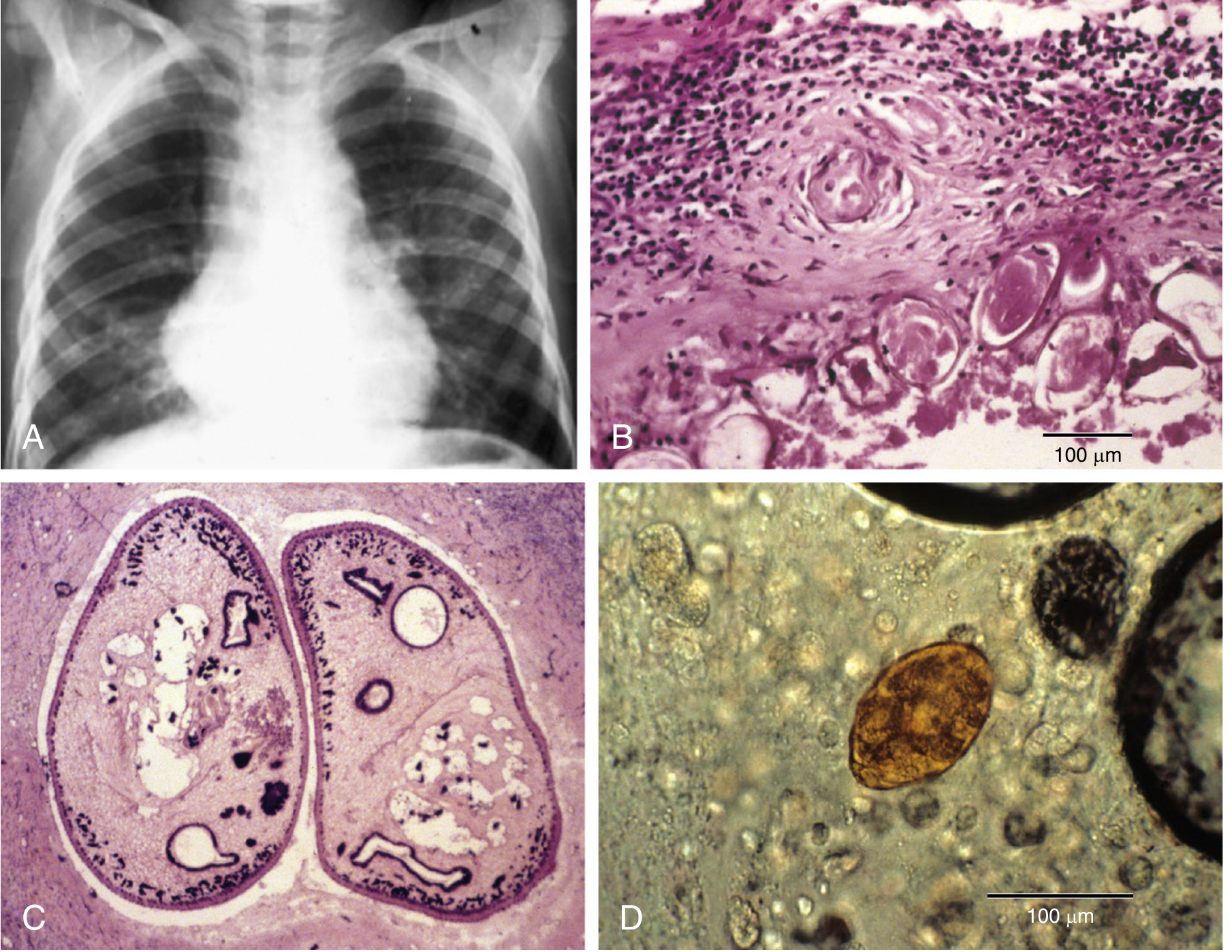
Figure 58.4: (A) Chest radiograph showing minimal perihilar left and right infrahilar linear and reticular opacities in a patient with hemoptysis. (B) Granuloma surrounding ova. (C) Cross section of a pair of adult worms in the lung. (D) Ovum in the sputum.
Figure 136-9 from Fishman's - Lung biopsy:
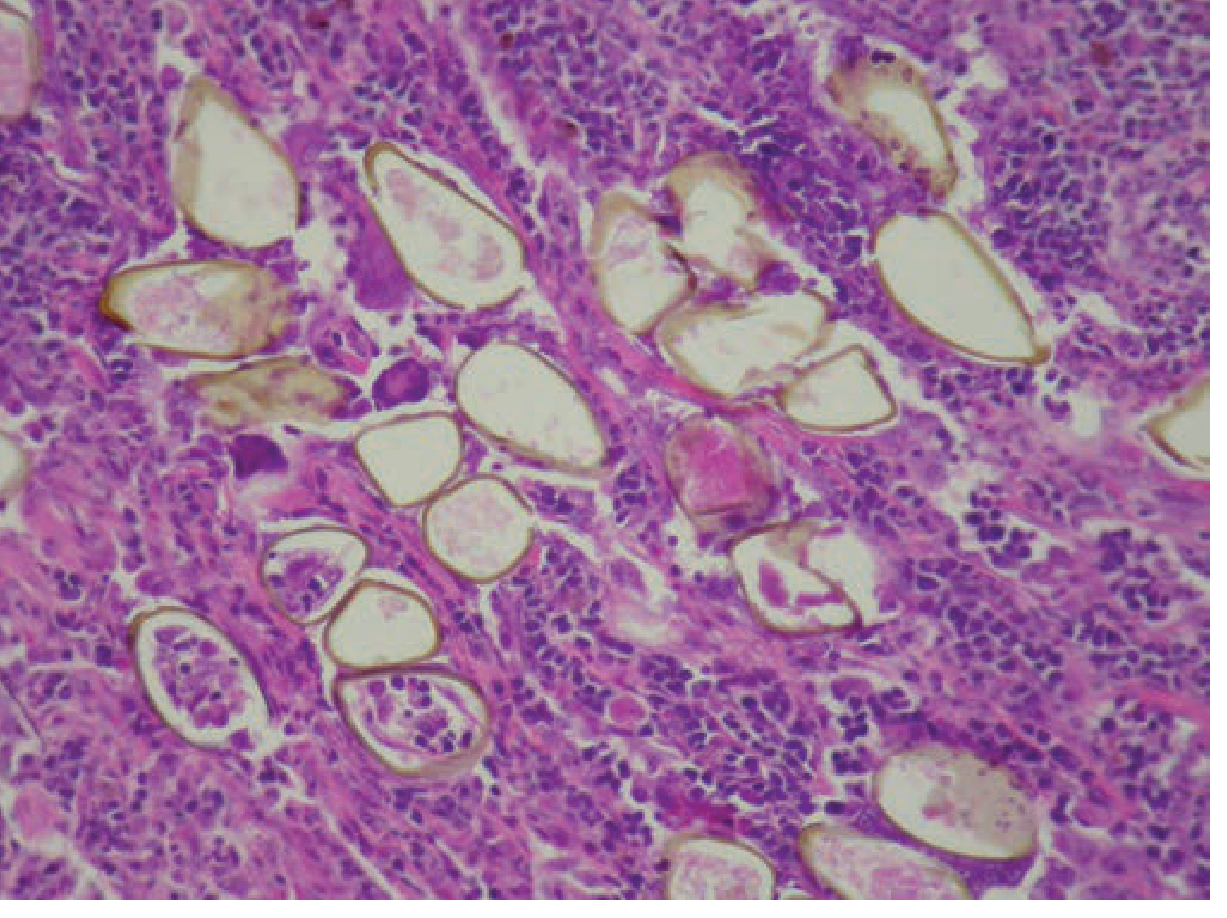
Figure 136-9: Lung biopsy demonstrating P. westermani operculated eggs on hematoxylin-eosin stain at 100x magnification. (Fishman's, p. 2428)
Summary Table for Rapid Revision
| Feature | Detail |
|---|---|
| Causative agent | P. westermani (Asia), P. kellicotti (North America) |
| Transmission | Raw/pickled freshwater crab or crayfish |
| Incubation | 2-16 weeks |
| Classic symptom | Hemoptysis + rust-brown sputum + eosinophilia |
| Key mimic | Tuberculosis |
| Characteristic eggs | Golden-brown, operculated, 100 x 55 µm |
| Pleural fluid finding | Low glucose (<10 mg/dL), low pH (<7.10), eosinophils + exudate |
| CT hallmark | "Ring sign" + linear tracks to pleura |
| Drug of choice | Praziquantel 25 mg/kg TID x 2-3 days |
| Alternative | Triclabendazole |
| Eosinophilia | 45-80% of cases |
| Extrapulmonary | CNS most common (up to 25% of hospitalized cases) |
This is a shared conversation. Sign in to Orris to start your own chat.