All about sle
Reading File
Finding Sources
Searching PubMed
"systemic lupus erythematosus"[MeSH Terms] AND management
Searching the Web
systemic lupus erythematosus SLE overview 2024 2025 clinical features diagnosis treatment
Reading File
Reading File
Finding Sources
Searching PubMed
"systemic lupus erythematosus"[MeSH Terms] AND treatment
Reading File
Finding Sources
Searching PubMed
"lupus erythematosus, systemic"[MeSH Terms] AND "drug therapy"[MeSH Terms]
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative textbooks plus recent PubMed trials. Let me compile the full response.
Systemic Lupus Erythematosus (SLE) - Complete Overview
Definition & Epidemiology
Systemic lupus erythematosus is a chronic autoimmune disease of unknown cause characterized by production of antibodies against numerous self-antigens - most prominently antinuclear antibodies (ANAs). These antibodies bind DNA, RNA, nuclear proteins, and protein-DNA/RNA complexes. Immune complex deposition drives inflammation and vasculitis, causing multiorgan pathology.
Key epidemiological facts:
-
Affects ~3.4 million people worldwide; ~400,000 new diagnoses per year
-
Most common in women of reproductive age (15-40 years)
-
Female:male ratio: 2:1 before puberty, rises to 4:1 after puberty
-
Significantly higher incidence in African American and Latino women (up to 1 in 250 African American women ages 18-65)
-
Poland, USA, Barbados, and China show the highest global incidence (2023 epidemiology study)
-
5-year survival: ~90% with modern treatment; >90% survive 15+ years
-
Textbook of Family Medicine 9e
Pathogenesis
SLE results from a complex interplay of genetic, epigenetic, hormonal, and environmental factors:
- Genetic factors: Strong HLA association with DR2, DR3, DR4, DR5; familial clustering evident
- Autoantibody production: ANA is the hallmark. Anti-double-stranded DNA (dsDNA) and anti-Sm antibodies are found almost exclusively in SLE and are diagnostically specific
- Three core mechanisms driving disease:
- Attenuated/dysregulated immune system (B cell, T cell, monocyte abnormalities)
- Cytokine microenvironment dysregulation
- Impaired apoptotic debris clearance - accumulation of nuclear material triggers autoimmunity
- Environmental triggers: Sunlight (UV), infections, stress (neuroendocrine changes), certain drugs, diet, toxins
- Hormonal influence: Estrogen drives female predominance; shifts in puberty affect sex ratio
The end result is immune complex deposition in tissues (kidneys, skin, joints, blood vessels, CNS), complement activation, and organ inflammation.
- Textbook of Family Medicine 9e, Andrews' Diseases of the Skin
Clinical Features
SLE is truly systemic - the classic triad of fever + joint pain + rash in a woman of childbearing age should always prompt investigation.
Constitutional
Fatigue, malaise, fever, weight loss - often the earliest and most persistent complaints
Mucocutaneous (>90% of patients eventually affected)
| Lesion | Description |
|---|---|
| Malar (butterfly) rash | Fixed erythema over malar eminences, bridges the nose, spares the nasolabial folds - only in ~1/3 of patients |
| Discoid lupus | Raised erythematous plaques with scaling, follicular plugging; causes scarring with hypopigmented atrophic center |
| SCLE | Annular or papulosquamous lesions in sun-exposed areas (upper torso); anti-Ro positive in ~70%; does NOT scar |
| Photosensitivity | 1/3 to 2/3 of patients; triggers flares |
| Oral ulcers | Usually painless; on hard palate, buccal mucosa; seen in ~21% |
| Alopecia | Diffuse, non-scarring; "lupus hairs" - short fragile frontal hairs |
| Bullous LE | Vesicles/bullae on sun-exposed skin; responds dramatically to dapsone |
| Vascular lesions | Periungual telangiectasia, erythema/edema of fingertips in ~50% |
The malar rash begins on the malar area and bridge of the nose, typically sparing the nasolabial crease (unlike dermatomyositis). It resolves without scarring.
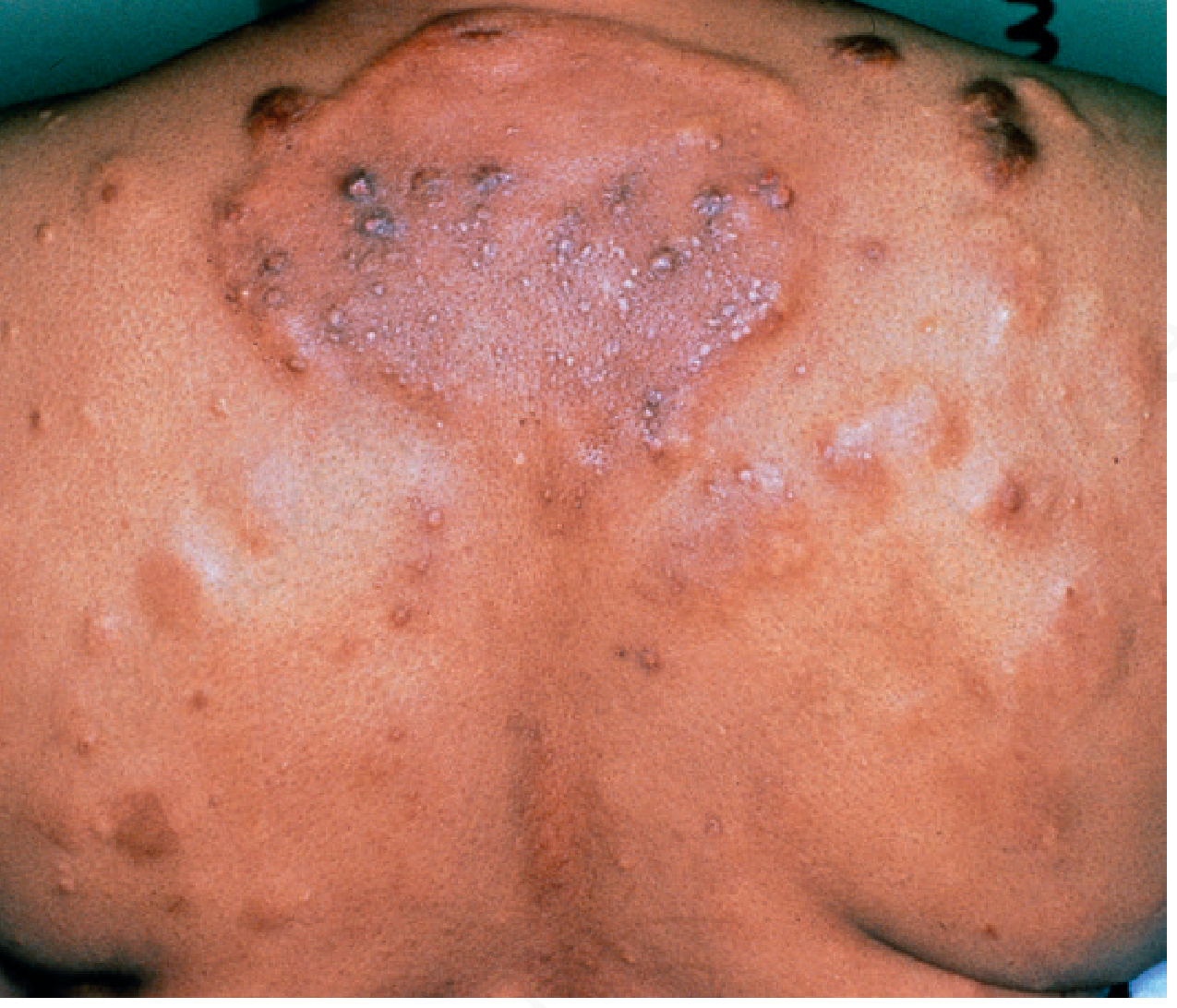
Clinical images from Andrews' Diseases of the Skin:
Papulonodular mucinosis in SLE (back):
Bullous lupus erythematosus (vesicles and bullae on the arm):

Musculoskeletal (~90%)
- Non-erosive arthritis involving 2+ peripheral joints (tenderness, swelling, effusion) - this is the most common complaint
- Arthralgia is even more prevalent
- Avascular necrosis (especially femoral head) can occur with steroid use
Renal (~50%)
Lupus nephritis is a major cause of morbidity. Features include:
- Proteinuria >0.5 g/day
- Cellular casts (red cell, hemoglobin, granular, tubular, or mixed)
- Can progress to nephrotic syndrome or RPGN
- WHO/ISN classes I-VI on biopsy guide treatment
- Higher incidence and severity in Asian and African American populations
Neuropsychiatric
- Seizures (in absence of metabolic causes)
- Psychosis
- Cognitive dysfunction, headaches, peripheral neuropathy, stroke
- Transverse myelitis (rare but severe)
Serositis
- Pleuritis: pleuritic chest pain, pleural effusion
- Pericarditis: ECG changes, pericardial effusion, rub - most common cardiac manifestation
- Libman-Sacks endocarditis (non-bacterial verrucous endocarditis) - pathognomonic but rare
Hematologic
- Hemolytic anemia with reticulocytosis
- Leukopenia (<4,000/mm³) or lymphopenia (<1,500/mm³)
- Thrombocytopenia (<100,000/mm³)
Pulmonary
- Pleuritis, pleural effusion
- Interstitial lung disease
- Pulmonary hypertension
- Rarely: "shrinking lung" syndrome
Antiphospholipid Antibody Syndrome (secondary)
- Found in ~30-40% of SLE patients
- Venous/arterial thrombosis, recurrent pregnancy loss
- False-positive VDRL/RPR (syphilis test) is a classic finding
Diagnosis & Classification Criteria
ACR 1982/1997 Criteria (need ≥4 of 11)
| # | Criterion | Detail |
|---|---|---|
| 1 | Malar rash | Fixed erythema over malar area, spares nasolabial folds |
| 2 | Discoid rash | Erythematous raised patches with scaling, follicular plugging |
| 3 | Photosensitivity | Rash from sunlight by history or physician observation |
| 4 | Oral ulcers | Nasal/nasopharyngeal ulceration, usually painless |
| 5 | Arthritis | Non-erosive; ≥2 peripheral joints with tenderness/swelling/effusion |
| 6 | Serositis | Pleuritis OR pericarditis |
| 7 | Renal disorder | Proteinuria >0.5 g/day OR cellular casts |
| 8 | Neurologic disorder | Seizures OR psychosis (excluding metabolic causes) |
| 9 | Hematologic disorder | Hemolytic anemia OR leukopenia OR lymphopenia OR thrombocytopenia |
| 10 | Immunologic disorder | Anti-dsDNA, anti-Sm, antiphospholipid antibodies |
| 11 | Positive ANA |
SLICC 2012 Criteria
Greater sensitivity with equal specificity vs ACR criteria. Requires:
- At least 4 criteria (≥1 clinical + ≥1 immunologic), OR
- Biopsy-proven lupus nephritis + positive ANA or anti-dsDNA
2019 EULAR/ACR Criteria
Most current. Weighted scoring system with ANA as entry criterion, then domains scored by weight.
- Andrews' Diseases of the Skin, Textbook of Family Medicine 9e, Rheumatology 2-Vol Set
Laboratory Investigations
| Test | Significance |
|---|---|
| ANA | Positive in >95% of SLE; screening test; not specific |
| Anti-dsDNA | Specific for SLE (~70%); correlates with disease activity, especially nephritis |
| Anti-Sm | Highly specific for SLE (~25-30%); does NOT correlate with activity |
| Anti-Ro/SSA | Associated with SCLE, neonatal lupus, photosensitivity |
| Anti-La/SSB | Associated with neonatal lupus |
| Antiphospholipid Ab | Lupus anticoagulant, anticardiolipin - thrombosis risk |
| Complement (C3, C4, CH50) | Low in active disease (consumption by immune complexes) |
| CBC | Hemolytic anemia, leukopenia, thrombocytopenia |
| Urinalysis | Proteinuria, hematuria, casts |
| Anti-histone | Drug-induced lupus |
| Direct Coombs test | Positive in hemolytic anemia |
Note: HIV testing often false-positive in SLE.
Treatment
Management is individualized based on organ involvement and disease severity. Hydroxychloroquine is the backbone of long-term therapy for all SLE patients.
General Measures
- Sun protection (sunscreen, UV-protective clothing) - mandatory
- Lifestyle: avoid triggers (infections, stress, certain medications like hydralazine, procainamide, isoniazid)
- Monitoring: regular labs (CBC, urine, complement, anti-dsDNA), BP control, bone protection
Drug Therapy by Indication
| Indication | Drug(s) |
|---|---|
| All SLE | Hydroxychloroquine (Plaquenil) - reduces flares, organ damage, mortality |
| Mild disease (rash, arthralgia) | NSAIDs, topical corticosteroids, hydroxychloroquine |
| Moderate-severe systemic | Prednisone 0.5-1 mg/kg/day |
| Cutaneous LE | Topical/intralesional steroids, hydroxychloroquine, chloroquine, quinacrine |
| Discoid LE (refractory) | Dapsone, retinoids (etretinate, isotretinoin), thalidomide |
| Lupus nephritis | High-dose corticosteroids ± mycophenolate mofetil or cyclophosphamide |
| CNS/severe nephritis | Cyclophosphamide (IV pulse) - Mesna co-administration to prevent hemorrhagic cystitis |
| Steroid-sparing | Azathioprine, methotrexate, mycophenolate mofetil |
| Severe refractory | Belimumab (anti-BLyS/BAFF biologic - FDA approved 2011) |
| Antiphospholipid syndrome | Warfarin (INR 2-3), long-term anticoagulation |
| Severe hemolytic anemia/thrombocytopenia | IV methylprednisolone, danazol, immunosuppressives, splenectomy |
Steroid tapering: If daily prednisone >10 mg/day is required, add azathioprine or methotrexate as steroid-sparing agents.
- Textbook of Family Medicine 9e
Emerging & Recent Therapies (2024-2025)
Recent landmark trials have expanded the therapeutic arsenal:
- Obinutuzumab (anti-CD20): Phase III RCT in active lupus nephritis (NEJM, 2025) showed improved renal response vs placebo
- Telitacicept (TACI-Fc fusion protein, dual BLyS/APRIL inhibitor): Phase III trial in SLE (NEJM, 2025 Oct) demonstrated significant reduction in flares
- Teclistamab (BCMA-targeted biCAR-T approach): Case series showed induced remission in refractory SLE (NEJM, 2024) - early but promising
- CAR-T cell therapy for ultra-refractory SLE - small studies show complete remission
Prognosis & Monitoring
- 5-year survival: ~90%; 15-year survival: >90% with treatment
- Leading causes of death: renal failure, cardiovascular disease (accelerated atherosclerosis), infections (from immunosuppression), CNS lupus
- Disease follows a relapsing-remitting course - unpredictable, requiring lifelong monitoring
- Disease activity monitored with: SLEDAI score, complement levels (C3/C4), anti-dsDNA titers, urinalysis
- Co-morbidity management is critical: cardiovascular risk reduction, osteoporosis prevention (with chronic steroid use), infection prevention
Drug-Induced Lupus
A distinct entity caused by drugs (hydralazine, procainamide, isoniazid, minocycline, anti-TNF agents). Key features:
- Anti-histone antibodies are the hallmark (positive in >95%)
- Anti-dsDNA and complement usually normal
- Resolves on drug withdrawal
- Renal and CNS involvement rare (unlike idiopathic SLE)
Special Populations
Neonatal lupus: Caused by passive transfer of maternal anti-Ro/SSA and anti-La/SSB antibodies. Features: cutaneous lupus rash, congenital heart block (potentially life-threatening), thrombocytopenia. Usually resolves by 6 months as maternal antibodies clear.
Pregnancy in SLE: High-risk pregnancy requiring specialist co-management. Risk of flares, preeclampsia, fetal loss (especially with antiphospholipid antibodies). Hydroxychloroquine is safe and should be continued. Cyclophosphamide and methotrexate are teratogenic - avoid.
Pediatric SLE: Tends to be more severe than adult-onset; more frequent renal and hematologic involvement.
Summary Table
| Feature | Detail |
|---|---|
| Type | Systemic autoimmune disease |
| Hallmark antibody | ANA (>95%); anti-dsDNA and anti-Sm most specific |
| Classic sign | Malar butterfly rash (1/3 of patients) |
| Most common symptom | Arthralgia/arthritis (~90%) |
| Most serious complication | Lupus nephritis |
| Key treatment | Hydroxychloroquine (all patients) |
| Monitoring | SLEDAI, complement, anti-dsDNA, urinalysis |
| Prognosis | 5-year survival 90%; relapsing-remitting course |
Sources: Textbook of Family Medicine 9e | Andrews' Diseases of the Skin 5e | Braunwald's Heart Disease | Murray & Nadel's Respiratory Medicine | Rheumatology 2-Vol Set (Elsevier, 2022) | Recent RCTs: NEJM 2025 (Obinutuzumab PMID 39927615; Telitacicept PMID 41092329)
This is a shared conversation. Sign in to Orris to start your own chat.