Basic cell carcinoma
Reading File
Finding Sources
Searching PubMed
"basal cell carcinoma"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have all the information needed to write a comprehensive answer. Here it is:
Basal Cell Carcinoma (BCC)
Overview
Basal cell carcinoma is the most common human malignancy, with more than 2 million cases diagnosed per year in the United States alone. It is a slow-growing cancer of the skin that rarely metastasizes but can be locally destructive, causing significant morbidity - especially on anatomically sensitive sites like the nose, ears, and periocular skin. - Fitzpatrick's Dermatology, p. 3795
Pathogenesis
The molecular hallmark of BCC is loss-of-function mutations in PTCH1 (Patched-1), a tumor suppressor gene that normally inhibits the Hedgehog (Hh) signaling pathway. When PTCH1 is mutated, it can no longer suppress Smoothened (SMO), resulting in constitutive Hedgehog pathway activation. This drives downstream transcription factors (GLI1, GLI2) that promote cell growth and survival.
- In sporadic BCC, PTCH1 mutations bear the signature of UV-induced DNA damage (C→T transitions at dipyrimidine sites).
- In Gorlin syndrome (Nevoid BCC Syndrome - NBCCS), germline PTCH1 mutations cause familial BCC along with odontogenic keratocystic tumors and medulloblastoma.
- Acquired TP53 mutations (also UV-induced) are common in both familial and sporadic forms.
The diagram below illustrates the Hh pathway in normal vs. mutated states:
-
Without SHH ligand: PTCH inhibits SMO → no tumor growth
-
With SHH binding or PTCH mutation: SMO is released → GLI activation → unregulated mitosis
-
Robbins & Kumar Basic Pathology, p. 3259; Fischer's Mastery of Surgery 8e, p. 1887
Clinical Subtypes
Here are clinical photos of the major BCC subtypes:
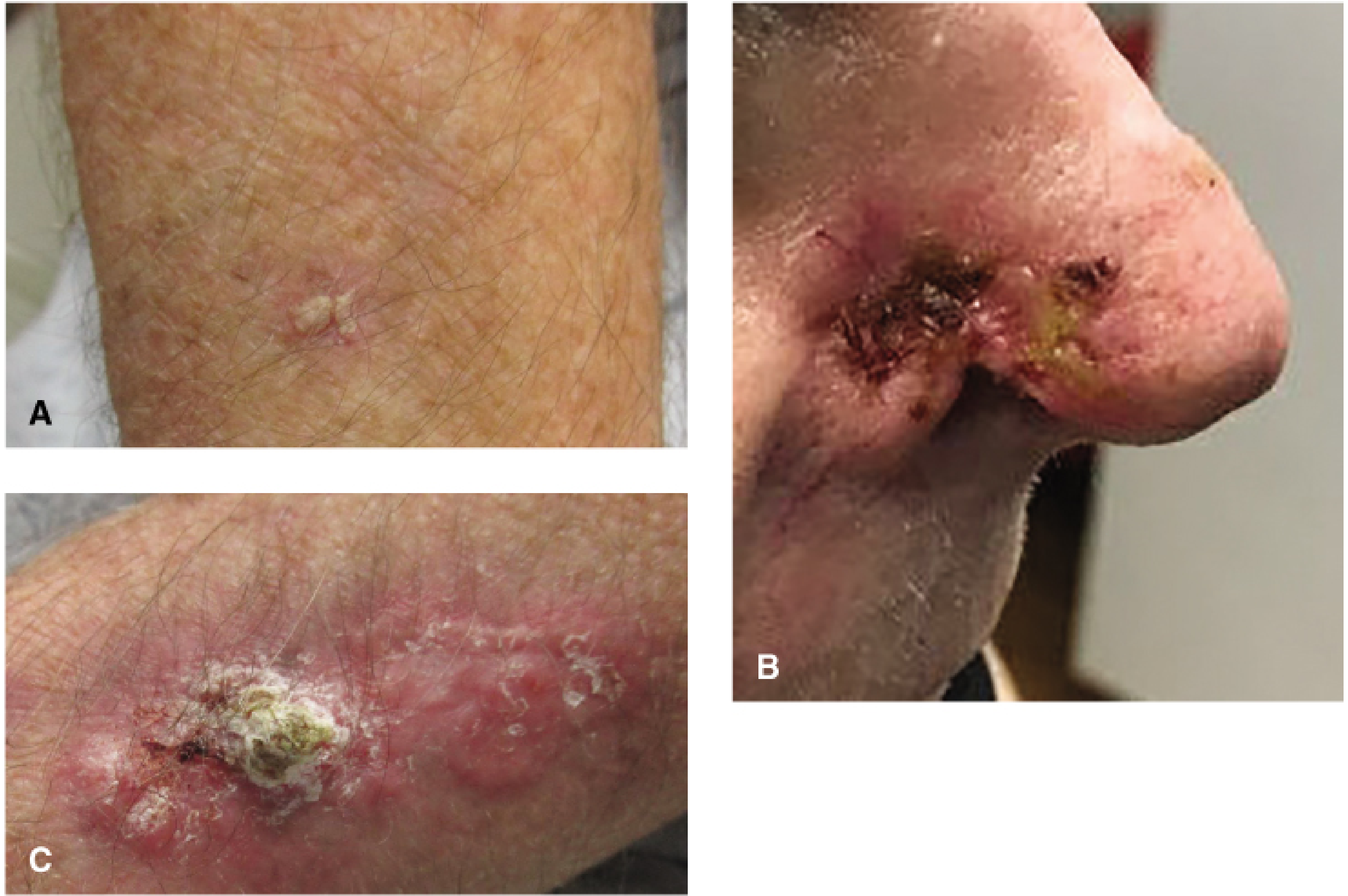
| Subtype | Clinical Features | Risk Level |
|---|---|---|
| Superficial | Erythematous, scaly, well-circumscribed plaque; trunk/extremities; may mimic eczema or psoriasis | Low risk |
| Nodular | Pearly papule, rolled/raised borders, central ulceration, telangiectasias; "rodent ulcer"; most common subtype | Low risk |
| Pigmented BCC | Nodular BCC with melanin; can mimic melanoma | Low risk (variant) |
| Morpheaform / Infiltrative | Flat, scar-like, yellowish/whitish plaque; ill-defined borders; extends microscopically beyond visible margin | High risk |
| Micronodular | Microscopic nests; wider subclinical extension; not always distinct clinically | High risk |
| Basosquamous | Mixed BCC/SCC features; higher metastatic potential | High risk |
- Harrison's Principles of Internal Medicine 22e, p. 650; Fischer's Mastery of Surgery 8e, p. 1888
Histopathology
Microscopically, BCC tumor cells resemble the normal epidermal basal cell layer or germinative elements of hair follicles. Key histological features:
- Nests and cords of basaloid cells with hyperchromatic nuclei, scant cytoplasm, and high nuclear-to-cytoplasmic ratio
- Peripheral nuclear palisading - the outermost cells of the tumor nests align in a row
- Stromal clefting (retraction artifact) - characteristic gap between tumor cell nests and surrounding stroma (distinguishes BCC from trichoblastoma, where clefting occurs within the stroma)
- Mucinous or fibrotic stroma
- Absent on mucosal surfaces (only arises from epidermis or follicular epithelium)
The image below shows BCC from dermoscopy and confocal microscopy:
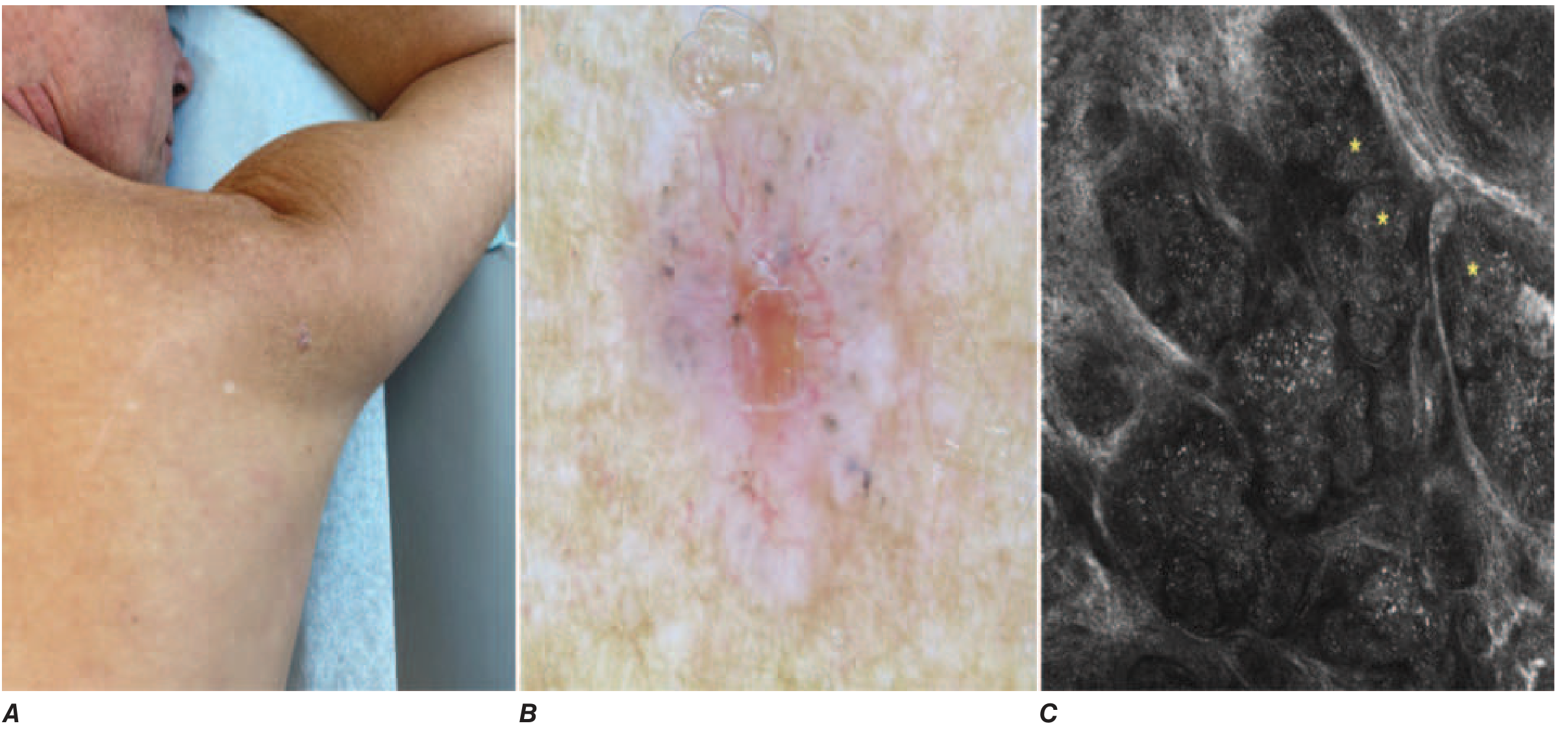
IHC tip: CK20+ Merkel cells are absent in BCC but present in trichoblastoma; CD10 stains tumor stroma in trichoblastoma but highlights the tumor cells in BCC. - Fitzpatrick's Dermatology, p. 3048
Risk Factors
- Cumulative UV/sun exposure (primary risk factor)
- Light skin (Fitzpatrick types I-II)
- Increasing age
- Male sex
- Immunosuppression (organ transplant recipients, HIV)
- History of prior radiation
- Genetic syndromes: Gorlin syndrome, xeroderma pigmentosum, Bazex syndrome
- Arsenic exposure
Incidence is 40-fold higher in sunny equatorial climates (e.g., Australia) vs. Northern Europe. - Robbins & Kumar, p. 3268
High-Risk Features (Predicting Recurrence)
| Category | High-Risk Features |
|---|---|
| Location | Head/face/scalp, nose, ears, periocular skin, lips, hands, feet, anogenital; trunk/extremities >2 cm |
| Size | >2 cm (trunk/extremities); any size on H-zone of face |
| Borders | Poorly defined, irregular |
| Histology | Infiltrative, micronodular, morpheaform, basosquamous, carcinosarcomatous, perineural invasion |
| Patient factors | Immunosuppression, prior radiation site, recurrent tumor |
- Fischer's Mastery of Surgery 8e, p. 1888-1889
Treatment
Surgical (Preferred for High-Risk BCC)
1. Mohs Micrographic Surgery (MMS)
- Gold standard for high-risk BCC (H-zone, large, recurrent, poorly defined margins, high-risk histology)
- Serial intraoperative frozen section analysis of 100% of the surgical margin
- 5-year recurrence rate: ~1-4% for primary BCC, 4-8% for recurrent BCC
- 99.4% cure rate for primary eyelid BCC (Mohs' own series of 1,124 patients)
- Meta-analysis of >10,000 patients: 5-year recurrence 3% (Mohs) vs. 5% (standard excision)
2. Standard Surgical Excision
- Adequate for low-risk BCC with standard margins (4 mm for nodular BCC)
- Infiltrative/micronodular subtypes may need 5-10 mm margins for clearance
Non-Surgical Options (Generally for Low-Risk BCC)
| Treatment | Notes |
|---|---|
| Radiation therapy | For patients unfit for/refusing surgery; 64 Gy over 7 weeks (tumors <2 cm); 70 Gy for larger/deep tumors |
| Electrodesiccation & Curettage (EDC) | Simple, office-based; suitable for superficial/low-risk BCC |
| Imiquimod 5% cream | Toll-like receptor agonist; immune activation against tumor; 70-80% clearance in superficial BCC; lower recurrence than 5-FU at 5 years (HR 0.65) |
| 5-Fluorouracil cream | Topical chemotherapy (inhibits DNA synthesis); superficial BCC only |
| Photodynamic therapy (PDT) | Photosensitizer (aminolevulinic acid) + visible light → reactive oxygen species → tumor death; off-label in USA; inferior to excision but better cosmesis |
| Cryotherapy | Liquid nitrogen, two freeze-thaw cycles; up to 20% recurrence at 5 years |
| Electrochemotherapy | Intralesional bleomycin + electroporation; lower efficacy than excision |
- Fischer's Mastery of Surgery 8e, pp. 1889-1892
Systemic Therapy (For Locally Advanced or Metastatic BCC)
Hedgehog Pathway Inhibitors (first-line):
- Vismodegib (FDA-approved for locally advanced AND metastatic BCC) - small molecule SMO inhibitor
- Sonidegib (FDA-approved for locally advanced BCC only)
- Both block SMO, downstream of the PTCH1/Hh pathway
- Mutation testing NOT required (virtually all BCC have aberrant Hh signaling)
- ERIVANCE trial (vismodegib): Objective response rate 60% (locally advanced), 49% (metastatic); duration ~1.5-2 years
- Adverse effects: Muscle/joint pain, alopecia, taste disturbances, weight loss, fatigue, nausea; >50% grade 3+ toxicity; ~50% discontinue by 1 year
- A 2026 meta-analysis confirmed safety and efficacy of both agents in head/neck BCC (PMID: 41025405)
Immunotherapy (second-line, Hh inhibitor-refractory):
-
Cemiplimab (PD-1 inhibitor): 31% objective response rate in phase II trial; 85% of responses ongoing at 12 months; significant grade 3+ adverse events (~50%)
-
Fischer's Mastery of Surgery 8e, pp. 1892-1894
Prognosis & Follow-Up
- Local recurrence rate after appropriate treatment is low (1-5%), but ~40% of patients will develop a new BCC within 5 years
- Metastasis is rare (<0.1%) but can occur with neglected, deeply invasive tumors
- Locally neglected tumors can invade bone, orbit, or facial sinuses ("rodent ulcer")
- Lifelong annual skin surveillance is recommended
Key Differentials
| Condition | Distinguishing Features |
|---|---|
| Trichoblastoma | Benign; clefting within stroma (not between nests and stroma); CK20+ Merkel cells present |
| Squamous Cell Carcinoma | Keratinization, intercellular bridges, solar elastosis; higher metastatic risk |
| Melanoma (pigmented BCC) | Dermoscopy distinguishes; biopsy confirmatory |
| Sebaceous carcinoma | Lipid vacuoles, foam cells; commonly periocular |
| Actinic keratosis | Premalignant, not invasive; atypical keratinocytes only in lower epidermis |
Recent evidence: A 2026 systematic review/meta-analysis in Head & Neck confirmed the safety and efficacy of vismodegib and sonidegib for advanced head/neck BCC. A 2024 systematic review in Dermatologic Surgery assessed laser therapies as an emerging non-surgical option for non-melanoma skin cancer. Vismodegib in Gorlin-Goltz syndrome was also reviewed in a 2024 Australasian systematic review (PMID 38867459), confirming benefit with significant side-effect burden.
a short answer
Basal Cell Carcinoma (BCC) — Summary
Most common human malignancy. Arises from epidermal basal cells / hair follicle germinative cells. Rarely metastasizes but can be locally destructive.
Pathogenesis: PTCH1 mutation → uncontrolled Hedgehog (Hh) signaling → unregulated cell proliferation. UV damage is the main cause of sporadic mutations.
Risk factors: UV exposure, fair skin, immunosuppression, Gorlin syndrome.
Subtypes:
- Nodular - pearly papule, rolled edges, telangiectasias, central ulceration (most common)
- Superficial - erythematous scaly plaque on trunk/limbs
- Morpheaform/Infiltrative - scar-like, ill-defined borders; highest risk
Histology: Basaloid cell nests, peripheral palisading, stromal clefting (retraction artifact).
Treatment:
- Mohs surgery - gold standard for high-risk/facial BCC (~1-4% recurrence)
- Surgical excision - standard for low-risk BCC
- Topical (imiquimod, 5-FU), cryotherapy, PDT - low-risk only
- Vismodegib / Sonidegib (SMO inhibitors) - locally advanced or metastatic BCC
- Cemiplimab (PD-1 blocker) - second-line after Hh inhibitor failure
Prognosis: Excellent if treated early. ~40% of patients develop a new BCC within 5 years.
Mbbs exam oriented for 5 marks
Basal Cell Carcinoma (BCC) — 5 Marks MBBS Answer
Definition
A malignant tumor arising from the basal layer of the epidermis or hair follicle germinative cells. It is the most common skin cancer (and most common human malignancy). Rarely metastasizes but is locally invasive.
Etiology & Risk Factors
- Chronic UV/sun exposure (most important)
- Fair skin, elderly, male
- Immunosuppression
- Gorlin syndrome (autosomal dominant; germline PTCH1 mutation)
- Ionizing radiation, arsenic exposure
Pathogenesis
PTCH1 mutation → loss of inhibition of Smoothened (SMO) → constitutive Hedgehog pathway activation → uncontrolled cell proliferation
Clinical Features
- Occurs on sun-exposed areas (face, especially nose, eyelids, cheeks)
- Classic lesion: Pearly/translucent papule with:
- Rolled/raised edges
- Central ulceration → "Rodent ulcer"
- Surface telangiectasias
Types (High-yield)
| Type | Key Feature |
|---|---|
| Nodular | Most common; pearly nodule, telangiectasias |
| Superficial | Scaly plaque on trunk/limbs |
| Morpheaform | Scar-like, ill-defined — most aggressive |
| Pigmented | Contains melanin; mimics melanoma |
Histology
- Nests of basaloid cells with hyperchromatic nuclei
- Peripheral nuclear palisading
- Stromal clefting (retraction artifact between tumor nests and stroma)
- No keratin pearls (differentiates from SCC)
Treatment
- Mohs micrographic surgery — gold standard (high-risk/facial)
- Surgical excision — 4 mm margins for nodular type
- Radiotherapy — for inoperable cases
- Topical imiquimod / 5-FU — superficial BCC
- Vismodegib (Hh inhibitor) — locally advanced / metastatic BCC
Prognosis
- Excellent with early treatment
- Metastasis rare (<0.1%)
- 40% develop a new BCC within 5 years — lifelong follow-up needed
This is a shared conversation. Sign in to Orris to start your own chat.