I now have excellent verified diagrams. Let me compile the full comprehensive answer with all images.
Core Embryology: Cloaca → Bladder → Urethra → Adrenal Gland (Q43-Q70)
SECTION 7: Cloaca and Bladder Development
Q43. What is the cloaca?
The cloaca is a dilated endodermal expansion of the terminal hindgut. It is a common chamber at the caudal end of the embryo (present ~4th week) that receives the hindgut, allantois, and mesonephric ducts before being partitioned.
Q44. What membrane closes its floor?
The cloacal membrane - a bilaminar plate (endoderm + ectoderm in direct apposition, no intervening mesoderm). It seals the floor of the cloaca until it ruptures once division is complete.
Q45. What tube connects cloaca to umbilicus ventrally?
The allantois - a ventral diverticulum arising from the cloaca, extending through the connecting stalk to the umbilicus. Key derivatives:
- Proximal allantois → apex of bladder
- Distal allantois → urachus → median umbilical ligament
Q46. What divides the cloaca and into what?
The urorectal septum (a wedge of mesoderm descending between allantois and hindgut, ~4th-6th weeks) divides the cloaca into:
| Compartment | Closes with | Adult fate |
|---|
| Anterior - Primitive urogenital sinus | Urogenital membrane | Bladder, urethra, etc. |
| Posterior - Anorectal canal/sinus | Anal membrane | Rectum, anal canal |
Diagram (a-c): Sequential development showing cloaca being divided by the urorectal septum - (a) intact cloaca with allantois and cloacal membrane; (b) urorectal septum descending, separating urogenital sinus from rectum; (c) final partition with urinary bladder and allantois above, rectum below, and separated urogenital vs. anal membranes.
Q47. What does entry of mesonephric ducts into the primitive urogenital sinus create?
The mesonephric ducts enter and divide the primitive urogenital sinus into two parts:
| Division | Location | Future structures |
|---|
| Vesico-urethral canal | Superior (above mesonephric duct entry) | Urinary bladder + most of urethra |
| Definitive urogenital sinus | Inferior (below mesonephric duct entry) | Subdivides further into pelvic & phallic parts |
SECTION 8: Urinary Bladder (Endoderm vs Mesoderm)
Q48. Main embryologic origin of urinary bladder?
Mainly from the vesical (superior) part of the urogenital sinus - endodermal origin.
Q49. What is the trigone and its embryologic origin?
The trigone is the smooth triangular region on the posterior bladder wall between:
- The two ureteric orifices (superolateral angles)
- The internal urethral orifice (inferior apex)
Embryologic origin: Mesoderm - derived from the absorbed caudal ends of the mesonephric ducts (Wolffian ducts) that are incorporated into the posterior bladder wall.
Q50. Is bladder epithelium endodermal or mesodermal?
Entire bladder epithelium (transitional/urothelium) is ENDODERMAL - even in the trigone region. This is the classic exam trap: although the trigone mesenchyme is mesodermal (from mesonephric ducts), the overlying epithelium is endodermal throughout.
Exam tip: "Trigone = mesodermal mesenchyme + endodermal epithelium"
Q51. Where do the other layers of bladder wall come from?
All non-epithelial layers (smooth muscle/detrusor, connective tissue) derive from adjacent splanchnic mesenchyme.
Q52. What happens to mesonephric ducts as bladder grows?
As the bladder expands:
- The caudal mesonephric ducts are absorbed into the dorsal bladder wall (creating the trigone mesenchyme)
- The ureteric buds (which arose from mesonephric ducts) get "carried" with this absorption
- Ureters migrate superolaterally to open at bladder angles
- Mesonephric ducts migrate inferiorly/caudally to open into the future urethra (ejaculatory ducts in males)
Q53. What does proximal allantois form?
The apex (dome) of the bladder. The allantois is the ventral connection between the early bladder and umbilicus.
Q54. What is the urachus and adult derivative?
- Urachus = the distal portion of the allantois between the bladder apex and umbilicus
- After birth it obliterates (fibroses) to form the median umbilical ligament, running beneath the anterior abdominal wall from bladder to umbilicus
SECTION 9: Urachal Anomalies
All urachal anomalies result from incomplete obliteration of the urachus after birth.
| Anomaly | Patent segment | Clinical presentation |
|---|
| Patent urachus (Urachal fistula) | Entire urachus | Urine discharge from umbilicus |
| Urachal cyst | Middle segment only (both ends closed) | Abdominal mass, infection |
| Urachal sinus | Distal (umbilical) end only | Serous discharge from umbilicus |
| Vesicourachal diverticulum | Proximal (bladder) end only | Bladder diverticulum at dome |
Q55. Urachal fistula
Failure of the entire urachus to obliterate → urine discharged from umbilicus. The tract remains open from bladder to umbilical skin.
Q56. Urachal cyst
Middle portion remains patent while proximal and distal ends obliterate → localized cyst, typically in the midline infraumbilical region. Can become infected.
Q57. Urachal sinus
Proximal (bladder) end obliterates but distal (umbilical) end remains patent → serous/mucoid discharge from umbilicus (no urine because bladder end is closed).
(Note: Some texts reverse this terminology - your slides define it as proximal obliterated/distal patent → discharge from umbilicus)
Q58. Bladder exstrophy (Ectopia vesicae)
Mechanism: Failure of mesoderm to migrate into the anterior abdominal wall between the ectoderm and cloacal membrane. The cloacal membrane is abnormally large and when it ruptures, the posterior bladder wall is exposed through the anterior abdominal wall.
- Bladder mucosa is exposed and everted
- Associated with epispadias (in males)
SECTION 10: Urethra Development (Male vs Female)
Q59. Female urethra
Derived entirely from the vesico-urethral canal of the primitive urogenital sinus. The female urethra is short (~4 cm) and entirely of endodermal origin.
Q60-64. Male urethra - 3 parts and their origins
The male urethra has 3 main parts with distinct embryologic origins:
| Part | Embryologic Origin | Source |
|---|
| Prostatic urethra (upper, above utricle) | Vesico-urethral canal of primitive urogenital sinus | Endoderm |
| Prostatic urethra (lower) + Membranous urethra | Pelvic part of definitive urogenital sinus | Endoderm |
| Penile (spongy) urethra | Phallic part of definitive urogenital sinus | Endoderm |
| Navicular fossa (in glans) | Ectodermal ingrowth (solid cord that canalizes) | Ectoderm |
Memory tip: "Three parts of UGS (vesico-urethral + pelvic + phallic) + ectodermal glans cap = complete male urethra"
Q65. Female note: pelvic + phallic portions contribute to?
In females, the pelvic and phallic parts of the definitive urogenital sinus contribute to the vestibule and the lower 2/3 of the vagina.
SECTION 11: Suprarenal (Adrenal) Gland Development
Q66. Embryologic origins of adrenal cortex and medulla
| Part | Origin | Germ layer |
|---|
| Cortex | Coelomic epithelium (mesothelium) of posterior abdominal wall | Mesoderm |
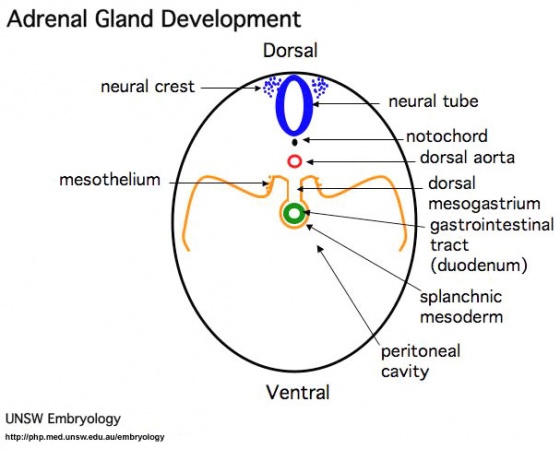
| Medulla | Neural crest cells (sympathochromaffin cells migrate from neural crest) | Ectoderm (neural crest) |
The medulla is essentially a modified sympathetic ganglion - neural crest cells that invaded the cortical primordium.
Cross-section of embryo showing neural crest (top, blue) as source of adrenal medulla chromaffin cells, and mesothelium (sides, orange) as source of adrenal cortex - both migrate toward the developing adrenal primordium.
Q67. When does fetal cortex appear?
Around the 6th week of development.
Q68. What happens to fetal cortex after birth?
- Fetal cortex regresses rapidly in the postnatal period
- Replaced by the permanent cortex (adult cortex)
- Fetal cortex completely disappears by ~3rd year
- Permanent cortex then differentiates into its 3 definitive zones
Q69. Three zones of permanent adrenal cortex
| Zone | Location | Hormone |
|---|
| Zona Glomerulosa | Outermost | Aldosterone (mineralocorticoids) |
| Zona Fasciculata | Middle (largest) | Cortisol (glucocorticoids) |
| Zona Reticularis | Innermost | Androgens (DHEA) |
Mnemonic: "GFR" (like glomerular filtration rate) - Glomerulosa, Fasciculata, Reticularis (outer to inner)
Or: "Salt, Sugar, Sex" (outer to inner - Aldosterone/salt, Cortisol/sugar, Androgens/sex)
Full histological maturation of all 3 zones occurs at puberty per the slides.
Q70. Congenital anomalies of the suprarenal gland
| Anomaly | Description |
|---|
| Agenesis | Complete absence of one or both adrenal glands |
| Ectopic suprarenal tissue | Adrenal tissue found beneath the kidney capsule (or along gonadal descent path) |
| Accessory cortical tissue | Extra nodules of cortical tissue near normal gland |
| Adrenogenital syndrome (CAH) | Cortical hypertrophy + excess androgen production (21-hydroxylase deficiency most common) - causes virilization in females, precocious puberty in males |
Cloaca Partition - Classic Diagram
Classic Anat/Embryology illustration: Cloaca being divided by the septum, with the Wolffian duct and kidney bud entering superiorly, bladder forming from the allantois/superior urogenital sinus, and rectum dorsal to the septum.
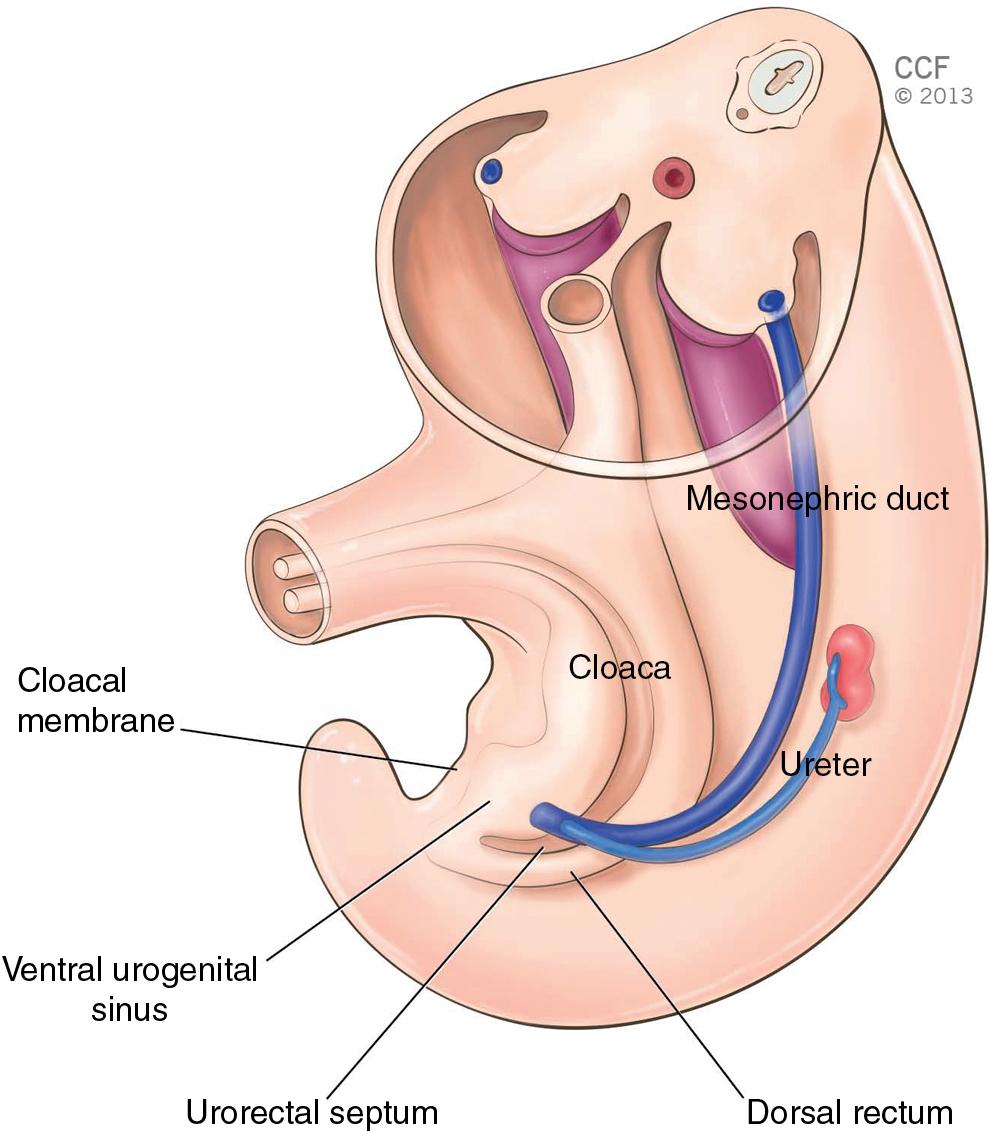
Modern Labeled Embryo Diagram
Comprehensive labeled diagram: Note cloaca (central chamber), mesonephric duct (blue, entering laterally with ureter budding off), urorectal septum descending, urogenital sinus ventral, rectum dorsal, and cloacal membrane at the floor.
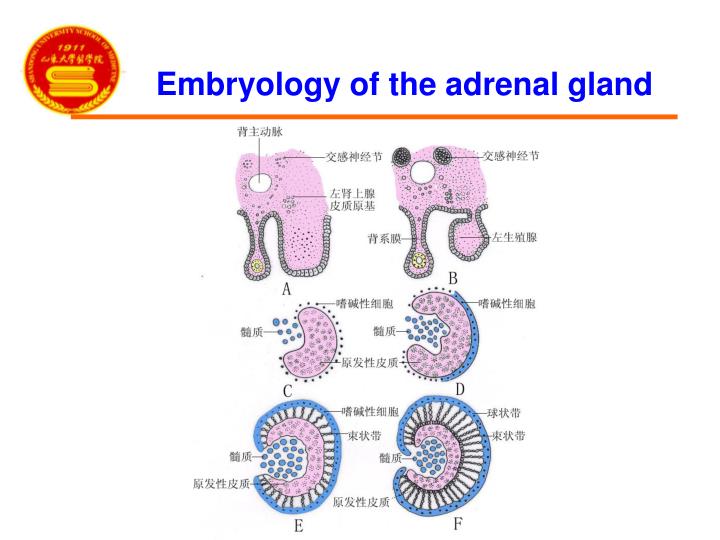
Adrenal Gland Sequential Development
Sequential cross-sections (A→F) of adrenal development: (A-B) mesothelial cortical primordium forming with sympathetic ganglia nearby; (C-D) chromaffin cells (medullary precursors) migrating inward; (E-F) permanent cortex differentiating with zona fasciculata visible (striped) surrounding the medulla.
Quick Summary Table - All Key Derivations
| Structure | Origin | Germ Layer |
|---|
| Bladder epithelium (ALL) | Vesico-urethral canal (UGS) | Endoderm |
| Trigone mesenchyme | Mesonephric duct absorption | Mesoderm |
| Bladder musculature | Splanchnic mesenchyme | Mesoderm |
| Bladder apex | Proximal allantois | Endoderm |
| Median umbilical ligament | Distal allantois (urachus) | Endoderm |
| Male prostatic urethra (upper) | Vesico-urethral canal | Endoderm |
| Male membranous urethra | Pelvic UGS | Endoderm |
| Male penile urethra | Phallic UGS | Endoderm |
| Navicular fossa (glans) | Ectodermal ingrowth | Ectoderm |
| Adrenal cortex | Coelomic mesothelium | Mesoderm |
| Adrenal medulla | Neural crest | Ectoderm |