Deep vein thrombosis with diagram according to vishram singh textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Let me compile a thorough, well-illustrated answer on DVT. Note: Vishram Singh's textbook is not available in this library, but I'll provide the content that aligns with what Vishram Singh covers (anatomy of lower limb veins, DVT pathophysiology - which is covered in his anatomy and clinical anatomy sections), drawing from Gray's Anatomy for Students, Robbins Pathology, Bailey & Love's Surgery, and Rosen's Emergency Medicine.
Deep Vein Thrombosis (DVT)
Note: Vishram Singh's textbook is not available in this library's collection. The content below is drawn from Gray's Anatomy for Students, Robbins & Kumar Basic Pathology, Bailey and Love's Surgery, and Rosen's Emergency Medicine - all authoritative sources that cover the same DVT topics found in Vishram Singh's clinical anatomy sections.
Definition
Deep vein thrombosis (DVT) is the formation of a blood clot (thrombus) within the deep veins, most commonly those of the lower limb - calf veins, popliteal vein, femoral vein, and iliac veins. It is a major clinical concern because thrombi can propagate and embolize to the pulmonary circulation, causing potentially fatal pulmonary embolism (PE).
Anatomy of the Lower Limb Venous System
The venous system of the lower limb is divided into:
Superficial system:
- Great saphenous vein (joins femoral vein at the saphenofemoral junction in the femoral triangle)
- Small saphenous vein (joins popliteal vein behind the knee)
- Perforating (communicating) veins - connect superficial to deep
Deep system (primary sites of DVT):
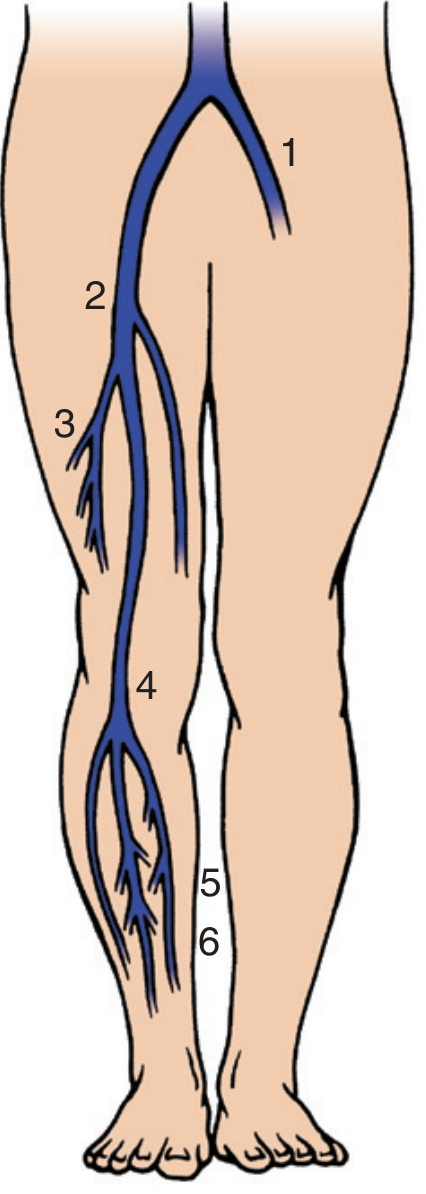
Fig. 1 - Six most common sites of DVT. 1 = Left iliac vein; 2 = Common femoral vein; 3 = Deep femoral vein (profunda femoris); 4 = Popliteal vein at adductor canal; 5 = Posterior tibial vein; 6 = Intramuscular veins of calf.
The calf veins (anterior tibial, posterior tibial, peroneal) unite at the knee to form the popliteal vein, which passes through the adductor (Hunter's) canal to become the femoral vein. The femoral vein is joined by the deep femoral vein and the great saphenous vein to form the common femoral vein, which becomes the external iliac vein at the inguinal ligament.
- Distal DVT = thrombus confined to calf veins
- Proximal DVT = thrombus in popliteal or more proximal veins
- Iliofemoral DVT = thrombus in proximal femoral and iliac veins (highest risk of PE)
(Rosen's Emergency Medicine, p. anatomy section; Pfenninger's Procedures for Primary Care)
Pathophysiology - Virchow's Triad
The three primary factors predisposing to thrombosis constitute Virchow's Triad:
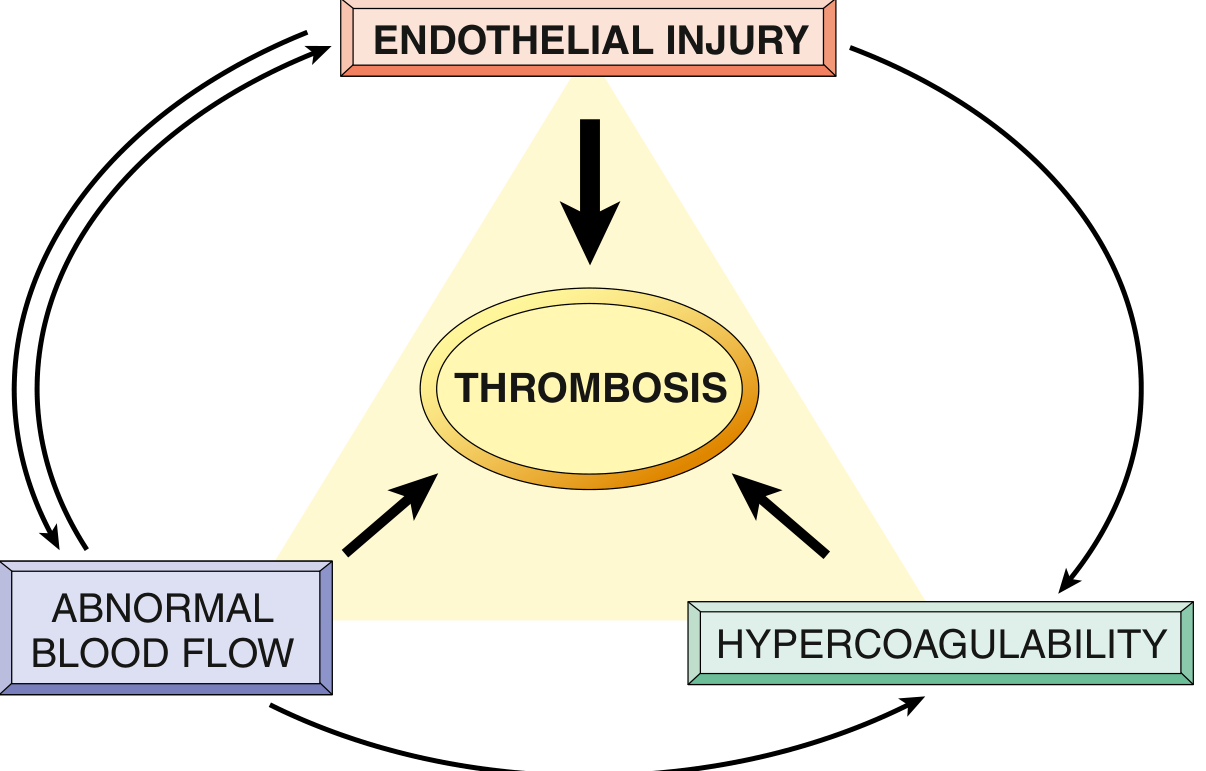
Fig. 2 - Virchow's Triad: the three interacting factors leading to thrombosis. (Robbins & Kumar Basic Pathology)
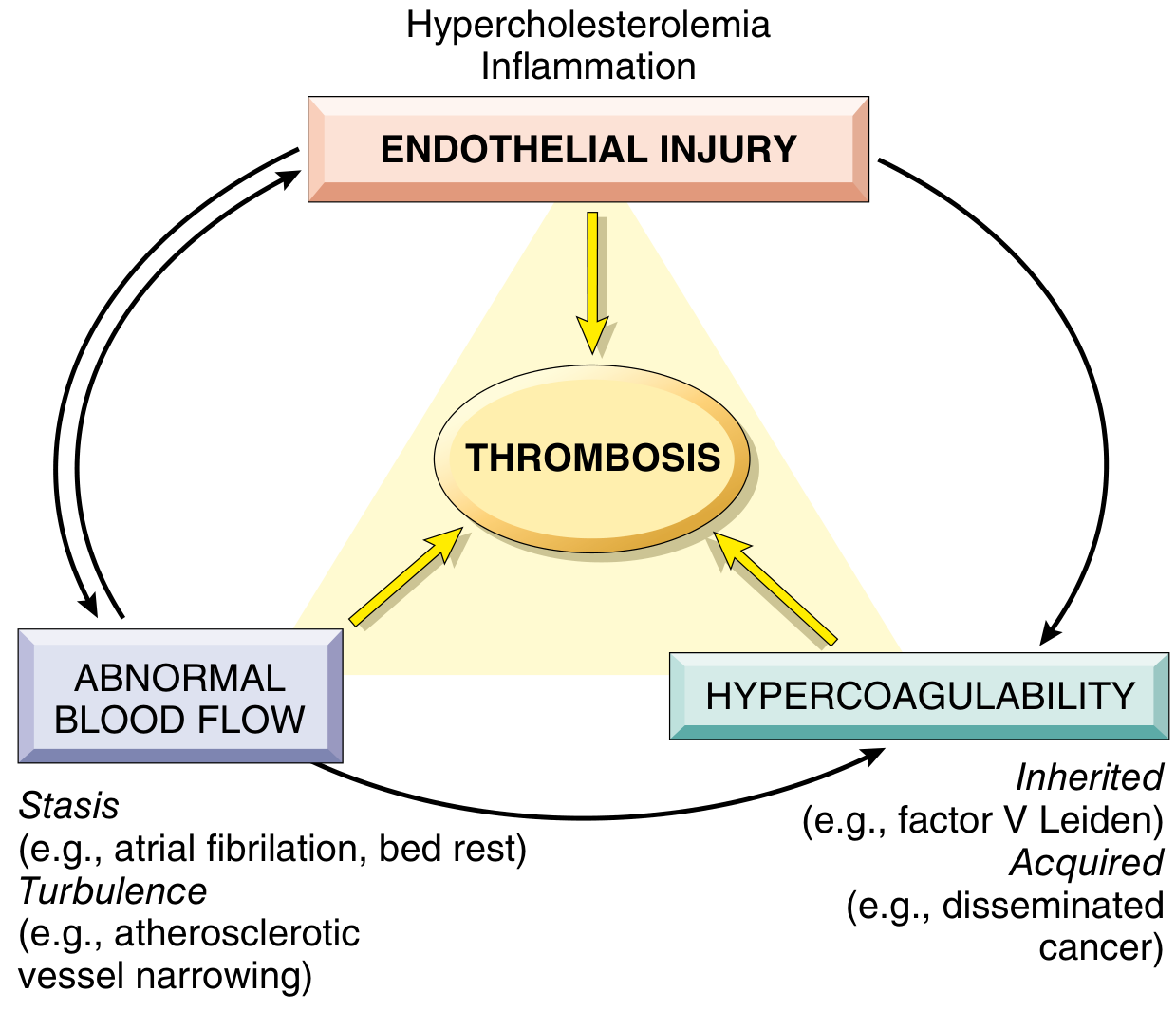
Fig. 3 - Virchow's Triad with clinical examples: Stasis (bed rest, atrial fibrillation), Endothelial injury (hypercholesterolemia, inflammation), Hypercoagulability - inherited (Factor V Leiden) and acquired (disseminated cancer). (Robbins Pathologic Basis of Disease)
1. Venous Stasis (Abnormal Blood Flow)
- Reduced muscular calf pump activity (immobility, bed rest, long travel)
- Obstruction to flow (e.g., gravid uterus compressing external iliac veins in pregnancy)
- Stasis allows platelets and leukocytes contact with endothelium, slows washout of activated clotting factors, and impedes inflow of clotting factor inhibitors
2. Endothelial Injury
- Direct trauma to vessel wall (surgery, fracture, catheter)
- Activates endothelial cells to shift toward a prothrombotic phenotype
- Exposes von Willebrand factor (vWF) and tissue factor
- Downregulates thrombomodulin, protein C, and tissue factor pathway inhibitor
- Increases secretion of plasminogen activator inhibitors (PAI), reducing fibrinolysis
3. Hypercoagulability
- Primary (genetic): Factor V Leiden mutation (most common inherited thrombophilia - 3-4x risk in heterozygotes, 25-50x in homozygotes; found in ~60% of recurrent DVT cases), Prothrombin gene mutation, Antithrombin III deficiency, Protein C or S deficiency
- Secondary (acquired): Malignancy, pregnancy, oral contraceptives, nephrotic syndrome, prolonged immobilization, postoperative state, myeloproliferative disorders, antiphospholipid syndrome
(Robbins & Kumar Basic Pathology, p. 88-90)
DVT Formation Mechanism
DVT typically begins when monocytes expose tissue factor on their surfaces to blood. This overwhelms natural anticoagulant and fibrinolytic mechanisms, leading to aggregation of red blood cells, platelets, and fibrin in the venous sinuses or cusps of the valve pockets of the lower extremity deep veins (areas of natural stasis).
The forming thrombus causes:
- Vascular congestion
- Venous dilation and valve incompetence
- Further venous stasis - promoting thrombus propagation (extending proximally)
- Risk of fragmentation and embolization
(Rosen's Emergency Medicine; Gray's Anatomy for Students)
Risk Factors (Summary Table from Bailey & Love)
| Risk Level | Examples |
|---|---|
| Low | Maxillofacial, neurosurgery, cardiothoracic surgery |
| Medium | Inguinal hernia repair, abdominal/gynaecological/urological surgery |
| High | Pelvic surgery (elective and trauma), total knee/hip replacement |
Additional risk factors: active cancer, paralysis/plaster immobilization, bed rest >3 days, previous DVT/PE, pregnancy, oral contraceptive use, age >40, malignancy, acute stroke with paresis.
(Bailey and Love's Surgery 28th Ed.)
Clinical Features
| Feature | Detail |
|---|---|
| Calf pain and tenderness | Often on palpation of the calf muscle mass |
| Swelling | Unilateral leg edema (most common presentation) |
| Warmth and redness | Due to local inflammation |
| Engorged superficial veins | Collateral drainage |
| Homans' sign | Calf pain on dorsiflexion of foot - NOT sensitive or specific |
Most DVT are clinically silent - no physical signs are present in the majority of cases.
(Bailey and Love's Surgery 28th Ed.; Gray's Anatomy for Students)
Complications
- Pulmonary Embolism (PE) - the most feared complication. Thrombus fragments break from the leading edge, travel through the right heart into the pulmonary arterial circulation.
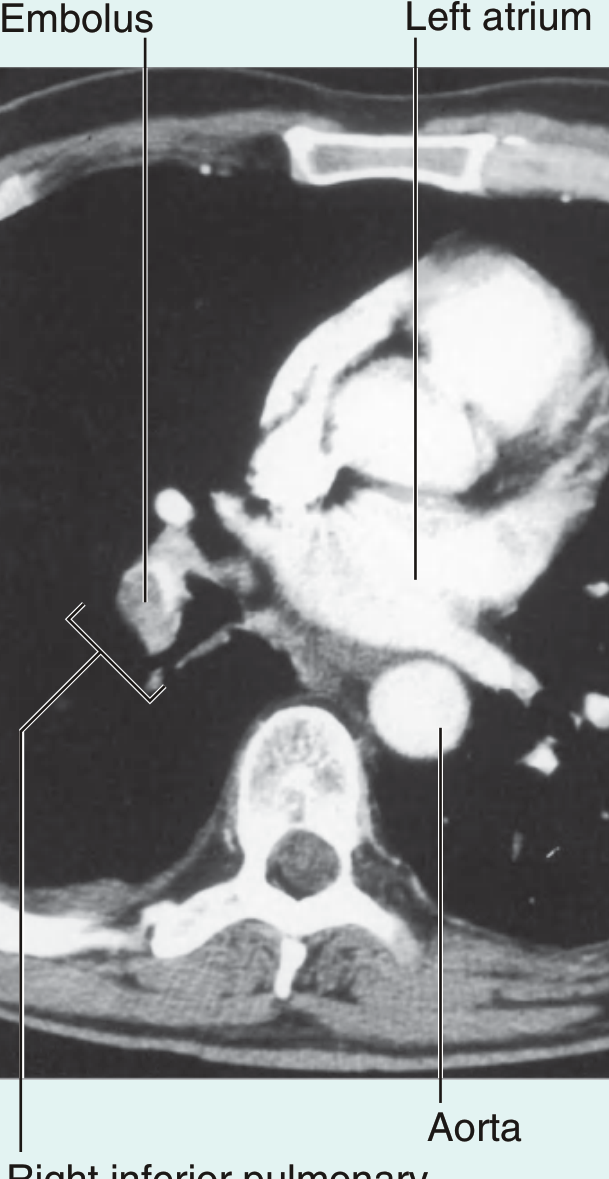
Fig. 4 - Axial CT pulmonary angiogram showing an embolus in the right inferior pulmonary artery. (Gray's Anatomy for Students)
- Small emboli cause pleuritic chest pain (sharp, worsened by breathing) and dyspnoea
- Large saddle emboli cause sudden cardiovascular collapse and death
- 50% of untreated proximal DVT cases result in PE
- 3% of PE remain as "clot-in-transit" in the right atrium/ventricle
- Post-thrombotic syndrome - chronic venous insufficiency, leg swelling, venous ulceration due to damaged valves
- Phlegmasia cerulea dolens - massive venous occlusion causing limb-threatening ischemia (rare but serious)
Diagnosis
Clinical probability scoring - Wells DVT Score:
| Clinical Feature | Points |
|---|---|
| Active cancer | 1 |
| Paralysis/paresis/plaster immobilization of lower limbs | 1 |
| Bedridden ≥3 days or surgery in previous 12 weeks | 1 |
| Localized tenderness along the deep vein | 1 |
| Entire leg swollen | 1 |
| Calf swelling >3 cm vs opposite side | 1 |
| Pitting edema confined to symptomatic leg | 1 |
| Collateral superficial veins (non-varicose) | 1 |
| Alternative diagnosis at least as likely | -2 |
- Score ≥2: DVT likely
- Score <2: DVT unlikely (proceed to D-dimer)
Investigations:
- Duplex Doppler ultrasound - primary imaging modality. Demonstrates: absent flow, non-compressibility of vein, absence of respiratory flow variation, absent augmentation with calf compression
- D-dimer - sensitive but not specific; negative D-dimer rules out DVT in low-probability cases
- Ascending venography - gold standard but rarely used (invasive)
(Bailey and Love's Surgery 28th Ed.; Gray's Anatomy for Students)
Management
Prophylaxis (prevention):
- Low-molecular-weight heparin (LMWH) injections
- Graduated compression stockings (contraindicated in peripheral arterial disease, severe leg oedema, neuropathy)
- Intermittent pneumatic compression (calf pumps)
- Early mobilization after surgery
Treatment:
- Initial anticoagulation: LMWH or unfractionated heparin (parenteral)
- Long-term anticoagulation: Direct oral anticoagulants (DOACs - rivaroxaban, apixaban) or warfarin
- Vena cava filter if anticoagulation contraindicated or recurrent PE despite anticoagulation
- Thrombolysis for massive PE with cardiovascular collapse (senior clinical decision)
DVT in Special Clinical Contexts
Pregnancy (as described in Gray's Anatomy for Students): The gravid uterus compresses the left external iliac vein, causing left-sided DVT more commonly than right. Anticoagulation (LMWH - safe in pregnancy) is the treatment; warfarin is teratogenic and DOACs are contraindicated.
Post-surgical: Risk assessment must occur within 24 hours of admission and be reviewed if the clinical condition changes.
Sources:
- Gray's Anatomy for Students, pp. 672, 785
- Robbins & Kumar Basic Pathology, pp. 87-90
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 126
- Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 345-346
- Rosen's Emergency Medicine, DVT anatomy & pathophysiology section
- Pfenninger and Fowler's Procedures for Primary Care, p. 596
This is a shared conversation. Sign in to Orris to start your own chat.