Renal angimyolipoma
Reading File
Finding Sources
Searching PubMed
renal angiomyolipoma management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Let me compile a detailed, well-organized answer.
Renal Angiomyolipoma (AML)
Definition and Classification
Angiomyolipoma is a benign mesenchymal neoplasm of the kidney composed of three elements: dysmorphic blood vessels, smooth muscle (spindle cells), and mature adipose tissue. It is classified as a PEComa (perivascular epithelioid cell tumor) and represents 1-2% of renal tumors. It can be:
-
Sporadic - most common form, predominantly in women, peak incidence 4th-5th decade
-
Syndrome-associated - tuberous sclerosis complex (TSC), lymphangioleiomyomatosis (LAM)
-
Campbell-Walsh-Wein Urology, p. 2294
Epidemiology
| Feature | Detail |
|---|---|
| General population prevalence | ~0.13% |
| Female:Male ratio | Strongly female predominant |
| Peak age (sporadic) | 4th-5th decade |
| TSC association | 55-90% of TSC patients have AML |
| TSC presentation | Earlier than sporadic cases |
Pathophysiology and Genetics
In TSC-associated AML:
- Mutations in TSC1 (hamartin, chromosome 9q34) or TSC2 (tuberin, chromosome 16p13)
- Inheritance: autosomal dominant, variable penetrance; sporadic mutations are common
- Hamartin-tuberin dimer normally inhibits mTOR - loss of function leads to unregulated mTOR activation
- Downstream: uncontrolled protein synthesis, cellular proliferation, and angiogenesis
This mTOR pathway activation is the rationale for mTOR inhibitor therapy.
In LAM (lymphangioleiomyomatosis): Also involves TSC1/TSC2 mutations; predominantly affects women; associated with cystic lung lesions, lymphangioleiomyomas, and chylous effusions.
Histopathology
- Tumors are well-circumscribed with a tan, pink, or yellow cut surface (depending on fat content)
- Composed of thick-walled eccentric blood vessels, smooth muscle spindle cells, and mature adipocytes (no atypia in classic form)
- Immunohistochemistry: Spindle cells have melanocytic features - positive for HMB-45 and Melan-A (key markers)
- AMLs also strongly express estrogen receptor-beta, progesterone receptor, and androgen receptor - explains the female preponderance postpuberty
Epithelioid AML - important variant:
-
Minimal fat, abundance of epithelioid cells
-
Frequent atypia, mitotic figures, and necrosis
-
Metastatic potential - reported in ~1/3 of cases (sporadic and TSC-associated)
-
Should be considered potentially malignant
-
Campbell-Walsh-Wein Urology, p. 2305-2307
Clinical Presentation
- Most are asymptomatic - incidentally detected on imaging
- Wunderlich syndrome (spontaneous retroperitoneal hemorrhage) - historically up to 15% of patients; AML is the most common cause of spontaneous retroperitoneal hemorrhage
- Flank/loin pain, flank mass, hematuria
- Pregnancy is a risk factor for hemorrhage (due to hormonal receptor positivity)
Diagnosis and Imaging
CT (Gold Standard)
- Intralesional fat density of -15 to -20 Hounsfield units (HU) on non-contrast series is diagnostic
- Cutoff of -10 HU gives a c-index of 0.83
- Fat on CT = definitive diagnosis - no biopsy needed
Ultrasound
- Hyperechoic (bright echogenic) mass - due to high fat content
- Less reliable; RCC can also appear hyperechoic
- Subcentimeter echogenic lesions are usually clinically insignificant
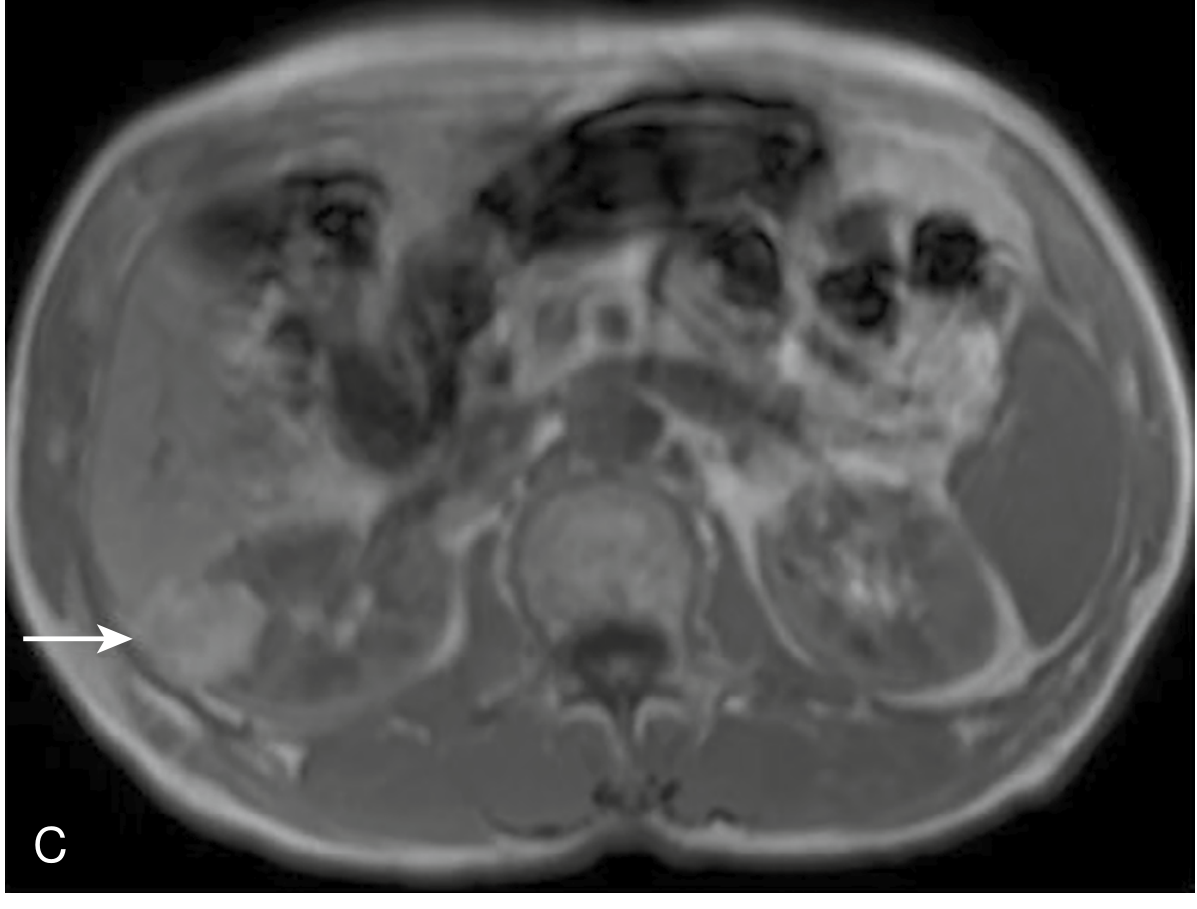
MRI
- AML follows signal intensity of intraabdominal fat on all sequences
- Loses signal on fat-saturated sequences
- India ink artifact on out-of-phase sequences at fat-water interface is diagnostic
- Non-fat components enhance avidly
Fat-poor AML (~4%) - cannot be distinguished from RCC on imaging; requires biopsy or surgery.
- National Kidney Foundation Primer on Kidney Diseases, p. 77; Bailey and Love's Surgery, p. 1503
Management
Management is guided by tumor size, symptoms, hemorrhage risk, and pregnancy status, with the overarching goal of renal function preservation.
Observation (Watchful Waiting)
- Tumors < 4 cm in asymptomatic patients can be followed with surveillance CT or MRI
- The traditional 4 cm cutoff for intervention has recently been questioned - some advocate individualized assessment
Selective Renal Angioembolization (SAE)
- Treatment of choice for acute hemorrhage
- Also used prophylactically for high-risk lesions (classically >4 cm)
- Technique: transfemoral/transradial approach, superselective catheterization of feeding vessels
- Embolics: ethanol + ethiodized oil (7:3 ratio) - ethanol provides permanent occlusion; ethiodized oil is radiopaque for monitoring
- Freedom from surgical intervention at 5 years: 94% after SAE
- Recurrence of hemorrhage: ~10-15%, managed by repeat embolization
- A short-term tapered prednisone course may reduce post-embolization syndrome (PES)
- A 2025 systematic review (PMID: 40165158) confirms safety and efficacy of SAE
Nephron-Sparing Surgery (Partial Nephrectomy)
- Preferred surgical option when intervention is needed
- Preferred over radical nephrectomy to preserve renal function
- Robot-assisted approaches are increasingly used; a 2025 meta-analysis (PMID: 41372556) compared robot-assisted vs. laparoscopic partial nephrectomy
mTOR Inhibitors
- Everolimus and sirolimus - indicated for larger, multifocal AMLs in TSC and LAM patients
- Target the dysregulated mTOR pathway
- Shown to reduce tumor size; excellent response rates in TSC-associated AML
- Everolimus is FDA-approved specifically for this indication
Summary Decision Framework
| Scenario | Management |
|---|---|
| AML < 4 cm, asymptomatic | Observation + surveillance imaging |
| AML > 4 cm, asymptomatic | Consider prophylactic SAE or surgery |
| Acute hemorrhage | Selective angioembolization |
| TSC/LAM with multiple/large AMLs | Everolimus (mTOR inhibitor) |
| Pregnancy with AML | Higher hemorrhage risk; individualize management |
- Campbell-Walsh-Wein Urology, p. 2378-2382; Bailey and Love's Surgery, p. 1503
Key Points Summary
- Benign PEComa - composed of blood vessels, smooth muscle, and fat; sporadic or TSC/LAM-associated
- TSC link - TSC1/TSC2 mutations -> loss of mTOR inhibition -> uncontrolled cell growth
- Diagnosis by imaging - macroscopic fat on CT (-15 to -20 HU) is pathognomonic
- Fat-poor AML (~4%) mimics RCC - requires biopsy
- Epithelioid AML - aggressive variant with malignant potential; HMB-45 positive
- Hemorrhage risk increases with size; AML is the leading cause of spontaneous retroperitoneal hemorrhage (Wunderlich syndrome)
- Angioembolization for acute bleeding; everolimus for TSC-associated multifocal disease
- 4 cm threshold has traditionally guided intervention, though now subject to individualized assessment
Recent evidence note: Two 2025 systematic reviews confirm the role of SAE in AML management [PMID: 40165158] and support robot-assisted partial nephrectomy as a viable surgical option [PMID: 41372556]. Neither appears to fundamentally alter established guidelines from textbook evidence.
This is a shared conversation. Sign in to Orris to start your own chat.