Mechanism of action of clomifem
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a full answer:
Mechanism of Action of Clomifene (Clomiphene Citrate)
Drug Class and Chemistry
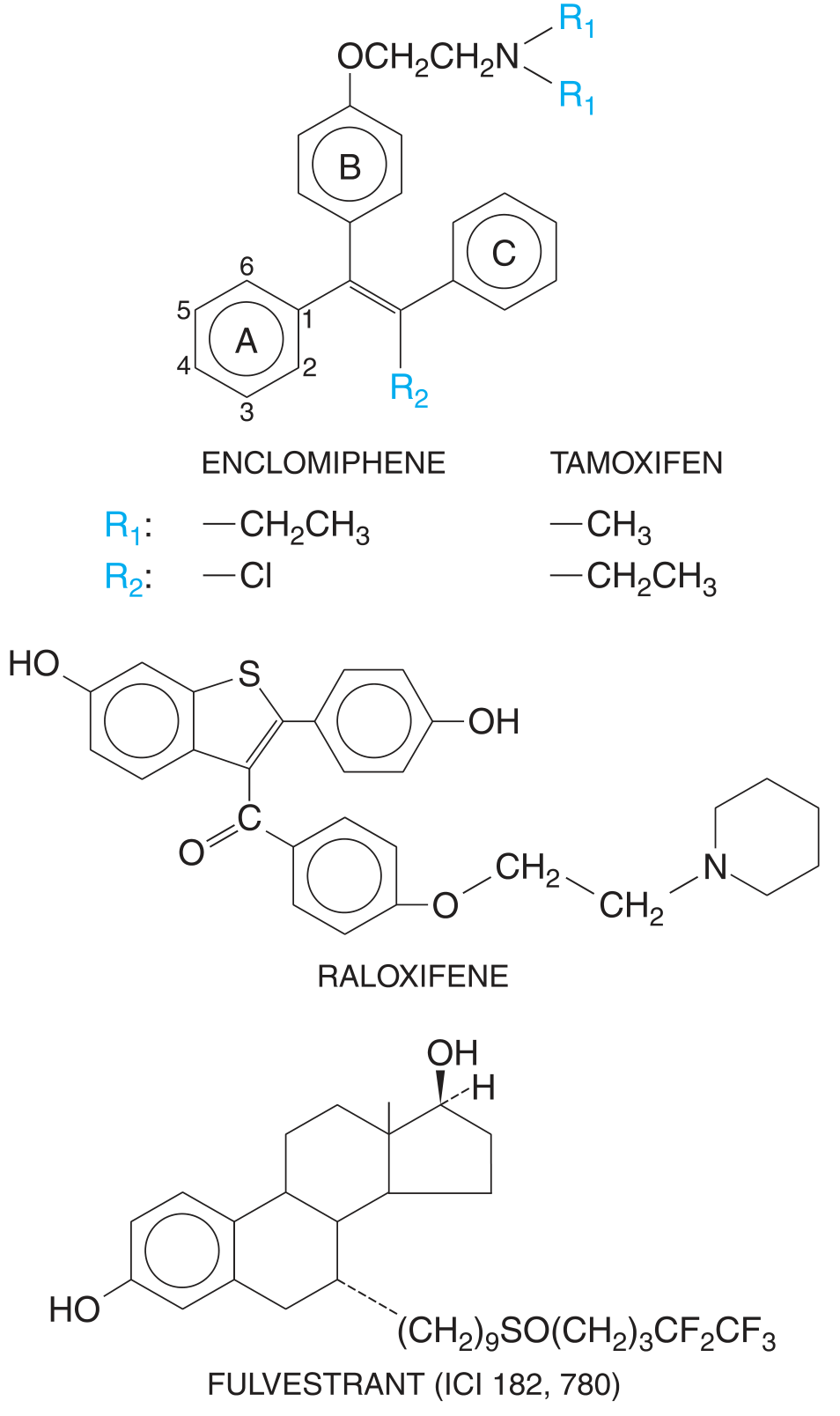
Clomifene citrate is a non-steroidal, synthetic selective estrogen receptor modulator (SERM) of the triphenylethylene class - structurally related to tamoxifen and diethylstilbestrol. It exists as two isomers with opposite activities:
| Isomer | Name | Activity |
|---|---|---|
| Trans-isomer | Enclomiphene | Potent estrogen antagonist |
| Cis-isomer | Zuclomiphene | Weak estrogen agonist |
Clomifene binds to both ERα and ERβ (estrogen receptor subtypes).
Core Mechanism
Clomifene acts primarily by blocking the negative feedback of estrogen on the hypothalamo-pituitary axis:
-
Estrogen receptor blockade: Clomifene occupies estrogen receptors in the hypothalamus and pituitary, preventing endogenous estradiol from binding and exerting its normal inhibitory (negative feedback) effect.
-
The brain "reads" low estrogen: Because the ER sites are occupied by clomifene (which recruits corepressors rather than coactivators in these tissues), the hypothalamus and pituitary perceive a hypo-estrogenic state.
-
Increased GnRH pulsatility: The hypothalamus responds by releasing more GnRH per pulse (pulse amplitude increases without a change in pulse frequency, suggesting the predominant site of action is the pituitary).
-
Gonadotropin surge (FSH + LH): The anterior pituitary responds with increased secretion of FSH and LH.
- FSH stimulates follicular growth and development
- The mid-cycle LH surge triggers ovulation
"Clomiphene increases the amplitude of LH and FSH pulses without changing pulse frequency... suggesting the drug is acting largely at the pituitary level to block inhibitory actions of estrogen on gonadotropin release."
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Step-by-Step Summary
Clomifene (oral)
↓
Binds ERα/ERβ at hypothalamus & pituitary
↓
Blocks estradiol's negative feedback
↓
Hypothalamus releases more GnRH per pulse
↓
↑ FSH + ↑ LH secretion from anterior pituitary
↓
FSH → Follicular recruitment & growth
↓
LH surge → Ovulation
SERM Paradox: Agonist vs. Antagonist
Clomifene's behavior is tissue-specific. Different ER-ligand conformations recruit different coactivators and corepressors depending on the cell type:
- Hypothalamus/pituitary: Acts as an antagonist (blocks estrogen feedback) → pro-gonadotropin
- Peripheral tissues (especially cervical mucus, endometrium): May act as an agonist or have mixed effects - this explains adverse effects such as thickened cervical mucus and a thin endometrial lining, which can reduce conception rates despite inducing ovulation
Male Use (Off-label)
In male hypogonadism/infertility, the same principle applies: clomifene blocks estrogen feedback on the hypothalamus, leading to increased GnRH → increased LH/FSH → stimulation of Leydig cells (testosterone production) and Sertoli cells (spermatogenesis). This is used for idiopathic oligospermia in the setting of low-normal gonadotropins and testosterone.
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Route | Oral |
| Half-life | 5-7 days |
| Elimination | Primarily feces (enterohepatic circulation); some urine |
| Distribution | High protein binding; accumulates in adipose tissue |
Clinical Use
- Primary indication: Ovulation induction in anovulatory/oligo-ovulatory infertility (especially PCOS)
- Dose: Typically 50-150 mg/day for 5 days (starting day 2-5 of cycle)
- Requires: Intact hypothalamo-pituitary-ovarian axis with adequate endogenous estrogen; not effective in ovarian or pituitary failure
Sources: Katzung's Basic & Clinical Pharmacology, 16th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics | Berek & Novak's Gynecology | Smith & Tanagho's General Urology, 19th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.