When patient neck down to see the mobile or other activities tear sensation from neck vertebra to fingers tell me which nerve can be involved and diagnosis and treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
cervical radiculopathy diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the information needed for a comprehensive, well-sourced answer. Here it is:
Cervical Radiculopathy - Neck Flexion Causing "Tearing Sensation" from Neck to Fingers
The symptom you describe - bending the neck (flexion, such as looking down at a phone) and feeling a tearing, shooting, or electric sensation radiating from the neck down to the fingers - is the hallmark of cervical radiculopathy. This is nerve root irritation or compression in the cervical spine. The act of neck flexion increases tension on the nerve roots and narrows the neural foramina, reproducing or worsening symptoms.
Which Nerves Are Involved
The symptoms radiate from neck to fingers, meaning the lower cervical nerve roots are involved. The most commonly affected levels are C5, C6, C7, and C8, since C5-C6 and C6-C7 are the most mobile segments with the greatest degenerative change.
| Nerve Root | Spinal Level | Pain / Sensory Area | Weakness | Reflex Lost |
|---|---|---|---|---|
| C5 | C4-C5 disc | Shoulder, lateral upper arm | Deltoid, biceps, brachioradialis | Biceps, supinator |
| C6 | C5-C6 disc | Thumb and index finger, lateral forearm | Brachioradialis, wrist extensors | Biceps, brachioradialis |
| C7 | C6-C7 disc | Index, middle, and/or ring fingers | Triceps, wrist flexors, pronators | Triceps |
| C8 | C7-T1 disc | Ring and little fingers, medial forearm | Finger flexors, intrinsic hand muscles | Finger flexors |
"Spondylosis, osteophytes, and disk herniations at the C4-C5 level can affect the C5 root... Pathology at the C5-C6 level can affect the C6 root and cause sensory changes in the first two digits and/or lateral distal forearm... Lesions at the C6-C7 level compressing the C7 root cause sensory changes in the index, middle, and/or ring fingers... The C5, C6, and C7 roots are the ones most commonly involved in cervical spondylosis."
- Bradley and Daroff's Neurology in Clinical Practice
C6 and C7 are the most common roots involved when the sensation reaches all the way to the fingers.
The "Phone Neck" Connection (Text Neck / Cervical Flexion)
When the head is tilted forward (neck flexion to look at a phone), several things happen simultaneously:
- The cervical neural foramina narrow further, increasing root compression
- The weight load on the cervical spine increases dramatically (from ~5 kg at neutral to ~27 kg at 45° flexion)
- Disc material is pushed posteriorly toward the nerve roots
- The dura and nerve roots are stretched, especially C6 and C7
The tearing/electric sensation you describe can also include Lhermitte's sign (electric shock radiating down the spine or into the arms on neck flexion), which suggests dorsal column or cord irritation in addition to root involvement - this warrants urgent evaluation.
Diagnosis
1. Clinical Examination
- Spurling's test - neck extension + rotation to the affected side + axial compression reproduces arm pain (opposite of your flexion trigger)
- Distraction test - lifting the head reduces pain (decompresses the foramen)
- Check for dermatomal sensory loss, muscle weakness, and reflex changes per the table above
2. Imaging
- MRI cervical spine - first-line; identifies disc herniation, foraminal stenosis, cord compression. Must be interpreted alongside clinical findings as degenerative changes are common even in asymptomatic spines
- CT myelography - used when MRI is contraindicated (pacemakers, prior fusion hardware) or when distinguishing osteophytes from soft disc herniation
3. Electrodiagnostics
- EMG / Nerve conduction studies (NCS) - the classic pattern in radiculopathy is reduced compound muscle action potential (CMAP) amplitude but preserved sensory nerve action potential (SNAP), because the compression is proximal to the dorsal root ganglion. This helps distinguish radiculopathy from brachial plexopathy or peripheral neuropathy
Differential Diagnoses to Consider
- Cervical myelopathy - cord compression; presents with Lhermitte's sign, upper motor neuron signs (hyperreflexia, clonus, Hoffman's sign), gait disturbance - more serious, requires urgent surgery
- Thoracic outlet syndrome - compression of brachial plexus or C8/T1 roots, causing numbness in 4th and 5th digits
- Carpal tunnel syndrome - median nerve compression at the wrist (mimics C6 distribution)
- Brachial neuritis (Parsonage-Turner syndrome) - sudden severe shoulder pain followed by weakness and wasting
- Ulnar neuropathy - causes ring and little finger symptoms (mimics C8)
Treatment
Conservative (First-Line, Most Cases Improve)
The natural history is favorable; most patients improve without surgery.
| Treatment | Details |
|---|---|
| NSAIDs / Acetaminophen | First-line for pain and inflammation |
| Muscle relaxants | Cyclobenzaprine 5-10 mg at night for spasm and sleep |
| Activity modification | Avoid prolonged neck flexion (reduce phone/device use), ergonomic adjustment |
| Physiotherapy | Cervical traction, mobilization, supervised exercises (neck and shoulder range of motion, strengthening) |
| Soft cervical collar | Short-term only; reduces pain modestly, minimal risk |
| Oral corticosteroids | Short course (e.g., methylprednisolone dose pack) for acute radicular pain; rapid taper |
| Epidural steroid injections | Imaging-guided; effective for subacute/chronic radicular pain; higher risk in cervical region (vertebral artery injury, cord injury) than in lumbar region |
Surgical (Reserved for Specific Indications)
Indications per Harrison's Principles:
- Progressive motor deficit due to nerve root compression
- Functionally limiting pain that fails to respond to conservative management
- Spinal cord compression (myelopathy)
Surgical options include:
- Anterior cervical discectomy and fusion (ACDF) - most common; removes disc and fuses the level
- Cervical disc arthroplasty (artificial disc replacement) - preserves motion; alternative to fusion in selected patients
- Posterior cervical laminectomy / laminoplasty - for multilevel disease or myelopathy
Note: The risk of radiculopathy or myelopathy at adjacent levels after fusion is approximately 3% per year and 26% per decade.
- Harrison's Principles of Internal Medicine 22nd Ed.
Practical Advice for the Patient
- Reduce phone/tablet neck flexion - hold devices at eye level; use a stand or mount
- Ergonomic workstation - monitor at eye level, chair with neck support
- Avoid prolonged postures in neck flexion
- Seek urgent evaluation if you develop: weakness in the hands/arms, loss of bladder or bowel control, bilateral symptoms, or progressive neurological changes - these may indicate myelopathy
Sources:
- Bradley and Daroff's Neurology in Clinical Practice
- Harrison's Principles of Internal Medicine, 22nd Ed.
- Miller's Review of Orthopaedics, 9th Ed.
- Firestein & Kelley's Textbook of Rheumatology
Patient with radiating tear sensation from neck vertebra to index finger when neck down ,and pain is mild please tell me treatment in physiotherapy and how much time to take recovery and which nerve involves with photos
Finding Sources
Finding Sources
Searching PubMed
cervical radiculopathy physiotherapy exercise rehabilitation
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading Article
Finding Sources
I now have everything needed. Let me compose the full, detailed answer.
C6 Nerve Root Radiculopathy - Focused Answer: Physiotherapy, Recovery & Nerve Anatomy
The Specific Nerve Involved
Tearing/electric sensation radiating from the neck to the index finger (and thumb), triggered by neck flexion = C6 nerve root compression at the C5-C6 disc level. This is the single most common level of cervical disc disease.
C6 Root - Complete Profile
| Feature | Details |
|---|---|
| Disc level | C5-C6 (most common cervical level) |
| Sensory area | Thumb, index finger, lateral forearm, radial side of hand |
| Pain distribution | Lateral forearm → thumb → index finger |
| Weakness | Biceps, brachioradialis, wrist extensors (ECRL/ECRB) |
| Reflex affected | Brachioradialis (and biceps) - may be diminished |
| Trigger | Neck flexion stretches/compresses C5-C6 neural foramen |
"C6 root: Reflex - Biceps; Sensory - Palmar thumb/index finger; Pain Distribution - Lateral forearm, thumb/index fingers."
- Harrison's Principles of Internal Medicine, 22nd Ed., Table 19-1
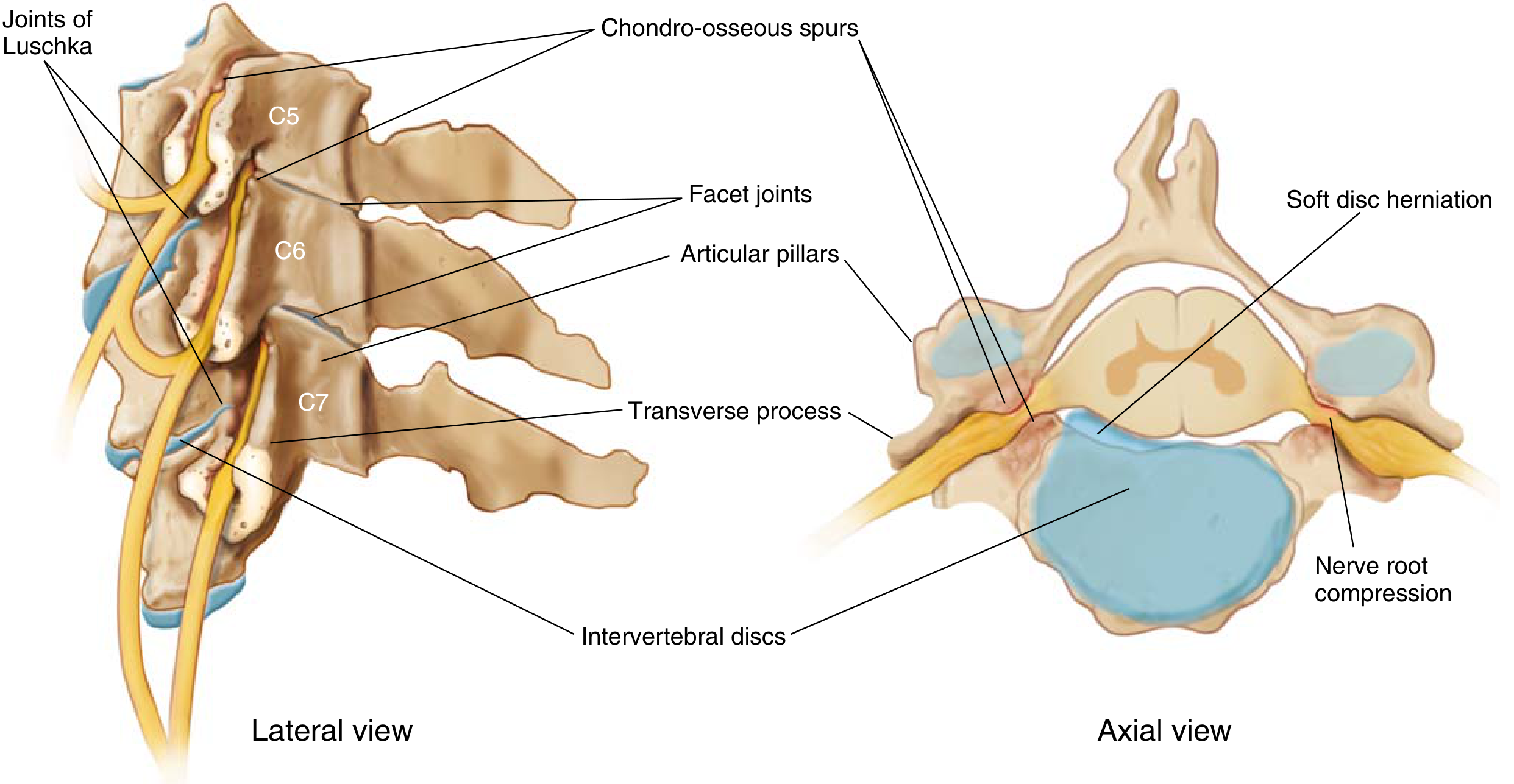
Anatomy - C6 Nerve Root Path
Lateral and axial views of cervical spine showing how disc herniation and spondylotic spurs compress the nerve root exiting at C5-C6 (C6 root) - Miller's Review of Orthopaedics, 9th Ed.
Brachial Plexus - C6 Downstream Pathway
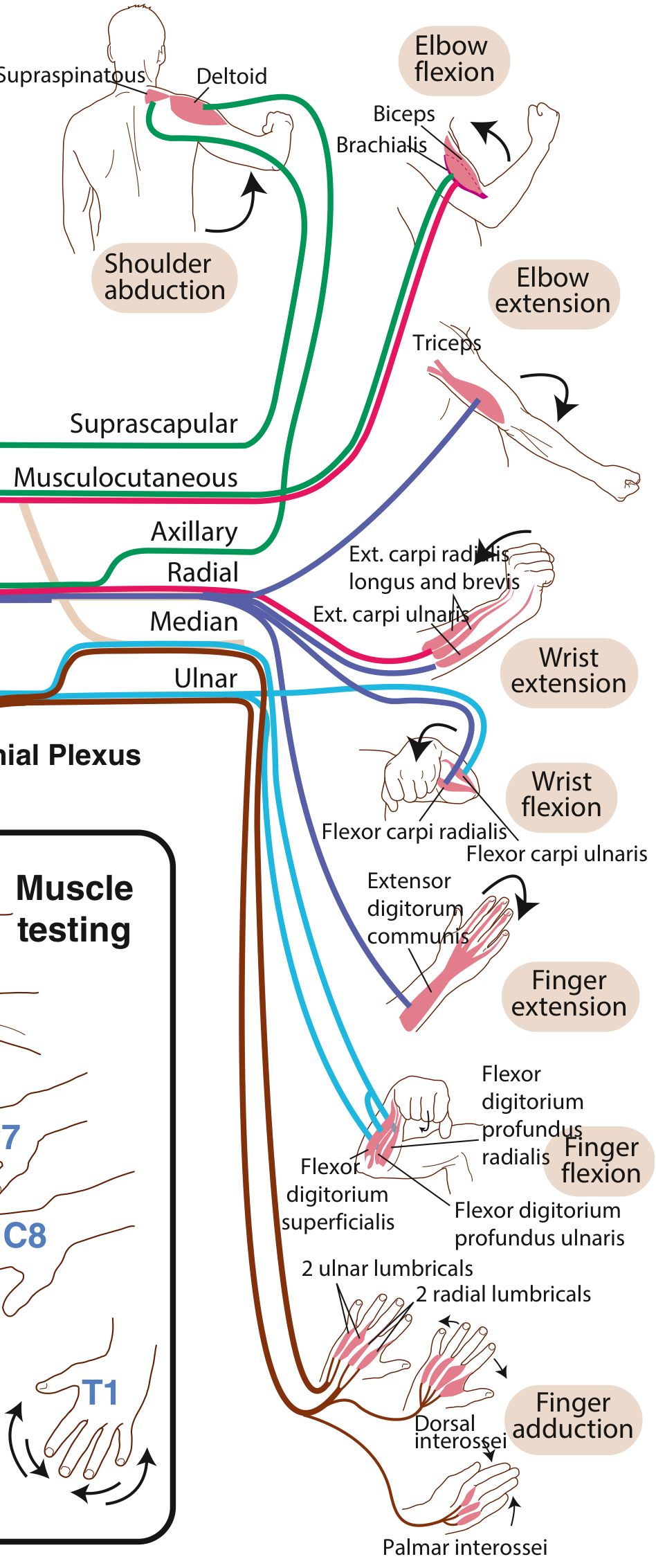
C6 root feeds into the musculocutaneous nerve (biceps, brachialis) and contributes to the radial nerve (wrist extensors, brachioradialis). These muscles and their sensory distribution to the thumb and index finger represent the C6 territory.
Physiotherapy Treatment Plan - Step by Step
Since symptoms are mild and triggered by posture/movement, conservative physiotherapy is the treatment of choice. The approach follows a structured progression:
Phase 1 - Acute/Pain Relief Phase (Weeks 1-2)
Goal: Reduce nerve root irritation, protect the segment, relieve pain.
1. Postural Education (Most Important Step)
- Phone hygiene - hold device at eye level, not looking down
- Avoid prolonged neck flexion beyond 15-20°
- Ergonomic setup: monitor at eye height, chair with headrest support
- "Chin tuck" awareness to maintain neutral cervical curve
2. Cervical Traction
- Mechanical or manual cervical traction - opens the C5-C6 neural foramen, directly decompresses the C6 root
- Home cervical traction devices can be prescribed (over-door traction or inflatable collar)
- Applied at ~10-15° of flexion for 15-20 minutes
- Evidence: neural mobilisation was found no more effective than cervical traction for pain and disability reduction (Lascurain-Aguirrebebeña et al., Pain, 2024 [PMID 37870223])
3. Electrophysical Modalities
- TENS (Transcutaneous Electrical Nerve Stimulation) over the cervical region - pain gate mechanism
- Ultrasound therapy over C5-C6 paravertebral area - reduces local inflammation
- Heat pack (moist heat) to cervical paraspinals before exercise - relaxes muscle guarding
- Ice pack after exercises if there is local soreness
4. Soft Cervical Collar
- Short-term use (1-2 weeks, not continuous) during activities that provoke symptoms
- Limits cervical flexion that compresses the C6 root
Phase 2 - Mobilization & Neural Gliding Phase (Weeks 2-4)
Goal: Restore nerve mobility, reduce neural tension, begin gentle movement.
5. Neural Mobilisation / Nerve Gliding (Median Nerve Bias - C6)
The C6 root feeds the median nerve. The Median Nerve Neurodynamic Test (ULNT1) performed gently as a treatment technique "glides" the nerve to reduce adhesions and neural tension.
Median nerve slider technique (C6/radial bias):
- Sit upright, arm at side
- Slowly depress shoulder + extend elbow + supinate forearm + extend wrist + extend fingers
- At first onset of sensation, stop and return
- Perform 10-15 gentle oscillations
- Do NOT push into pain - this is a slider, not a tensioner
Evidence: Neural mobilisation is more effective than standard physiotherapy alone for both pain and disability in cervicobrachial pain (pooled pain MD = -1.44; Pain, 2024, PMID 37870223).
6. Manual Therapy - Cervical Joint Mobilisation
- Maitland Grade I-II mobilisations at C5-C6 (oscillatory, gentle, below pain threshold)
- Reduces joint stiffness and reflex muscle guarding around the compressed foramen
- Manual physical therapy shows consistent benefit for neck disorders (Reynolds et al., J Man Manip Ther, 2025, PMID 39607420)
- Avoid high-velocity manipulation in the acute phase with radiculopathy
7. Soft Tissue / Myofascial Release
- Release of cervical paraspinals, upper trapezius, scalenes (which can secondarily compress the brachial plexus)
- Levator scapulae and suboccipital release
- RCT evidence supports myofascial release for reducing pain in unilateral cervical radiculopathy (Bali & Bayram, Explore, 2024, PMID 38296722)
Phase 3 - Strengthening & Stabilisation Phase (Weeks 4-8)
Goal: Restore neck and upper limb strength, prevent recurrence.
8. Deep Cervical Flexor Strengthening
- Chin tuck exercise (craniocervical flexion) - the most evidence-based exercise for cervical radiculopathy
- Activates longus colli and longus capitis (deep stabilisers)
- 10-second holds × 10 repetitions, 2-3 sets daily
- Reduces mechanical load on posterior elements including C5-C6 foramen
9. Cervical Range-of-Motion Exercises
- Gentle active rotation, lateral flexion, extension - within pain-free range
- Avoid sustained neck flexion as an exercise
- Progress to resisted rotation with Thera-Band
10. Scapular Stabilisation
- Scapular retraction exercises (rows, shoulder blade squeezes)
- Lower trapezius activation: "Y" and "T" exercises in prone position
- Strengthens the periscapular muscles that support the cervicothoracic junction and reduce upper-extremity strain
11. Upper Limb / Biceps-Focused Strengthening (C6 targets)
- Light resistance bicep curls (C6 motor = biceps, brachioradialis)
- Wrist extension with Thera-Band (ECRL/ECRB = C6)
- Start with low load to avoid Valsalva-type pressure that worsens radicular pain
12. McKenzie Method
- Cervical retraction (chin tucks) and extension exercises
- Particularly useful when symptoms have a directional preference (less pain in extension than flexion)
Phase 4 - Functional Return & Maintenance (Weeks 8-12+)
- Progressive strengthening with full range of motion
- Sport/work-specific movements
- Ergonomic reassessment
- Home exercise program for long-term maintenance
- Education on avoiding repetitive/sustained neck flexion
Recovery Timeline
| Phase | Duration | Expected Progress |
|---|---|---|
| Acute relief | 1-2 weeks | 20-30% reduction in pain |
| Mobilisation | 2-4 weeks | Nerve symptoms start to reduce, range improves |
| Strengthening | 4-8 weeks | Most patients with mild symptoms see 50-70% improvement |
| Functional return | 8-12 weeks | Near-complete recovery |
| Full recovery | 3-6 months | Resolution of residual tingling |
For mild cervical radiculopathy (your case), the natural history is very favorable. Most patients improve significantly within 4-8 weeks of physiotherapy. Complete symptom resolution (especially the finger tingling) may take 3-6 months as the nerve heals.
- Harrison's Principles of Internal Medicine, 22nd Ed.
Factors that speed up recovery:
- Starting physiotherapy early
- Correcting the posture trigger (phone use) immediately
- No motor weakness (mild = better prognosis)
- Younger age
- Soft disc herniation (vs. hard osteophyte)
Red Flags - Seek Urgent Medical Attention
Stop physiotherapy and see a doctor immediately if:
- Weakness develops in the hand or arm
- Symptoms spread to both arms or legs
- Bladder or bowel changes appear
- Symptoms worsen significantly with physiotherapy
- You develop balance problems or walking difficulty (suggests myelopathy)
Summary: The Key Points
- Nerve involved: C6 root (C5-C6 disc level) - travels to thumb and index finger
- Cause: Disc herniation or foraminal narrowing at C5-C6, aggravated by neck flexion
- First physiotherapy priority: Stop the trigger - raise phone/device to eye level TODAY
- Most effective physiotherapy: Cervical traction + neural mobilisation (median nerve gliding) + deep cervical flexor strengthening
- Recovery: 4-8 weeks for significant improvement; full nerve recovery 3-6 months
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Miller's Review of Orthopaedics, 9th Ed.
- Lascurain-Aguirrebebeña et al. Neural mobilisation for cervicobrachial pain. Pain, 2024 [PMID 37870223]
- Reynolds et al. Manual physical therapy for neck disorders. J Man Manip Ther, 2025 [PMID 39607420]
- Bali & Bayram. Myofascial release in cervical radiculopathy RCT. Explore, 2024 [PMID 38296722]
This is a shared conversation. Sign in to Orris to start your own chat.