Write a short note on microscopic hypochromic anaemia based upon robbins
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the material needed. Here is the complete note:
Microscopic Hypochromic Anaemia - Based on Robbins
(Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar - Basic Pathology)
Definition
Hypochromic (microcytic) anaemia is a group of anaemias characterised by red cells that are smaller than normal (microcytic) and pale due to reduced haemoglobin content (hypochromic). The underlying defect in all cases is a failure of adequate haemoglobin synthesis, which can result from deficiency of iron, impaired haem synthesis, or defective globin chain production.
The most important and common cause is iron deficiency anaemia - the most common nutritional disorder in the world.
Causes of Hypochromic Microcytic Anaemia
| Cause | Mechanism |
|---|---|
| Iron deficiency anaemia | Insufficient iron for haem synthesis |
| Anaemia of chronic inflammation | Hepcidin-mediated iron sequestration |
| Thalassaemias (alpha & beta) | Defective globin chain synthesis |
| Sideroblastic anaemia | Impaired haem synthesis despite adequate iron |
Iron Deficiency Anaemia - The Prototype
Etiology
Iron deficiency arises from four broad causes:
- Chronic blood loss - the most important cause in higher-resource countries. Sources include the gastrointestinal tract (peptic ulcers, colon cancer, hemorrhoids) and the female genital tract (menorrhagia, metrorrhagia).
- Dietary lack / low bioavailability - most common in lower-resource countries where diets are predominantly vegetarian. Heme iron (from meat) is ~20% absorbable vs. only 1-2% for non-heme iron. Even in high-resource settings, infants fed exclusively on milk, the impoverished, and the elderly are at risk.
- Increased demand - pregnancy and infancy are the key examples worldwide.
- Malabsorption - celiac disease, gastritis, or post-gastrectomy states.
Stages of Iron Depletion
Iron deficiency develops insidiously through sequential stages:
- Depletion of iron stores - serum ferritin falls; stainable iron disappears from bone marrow macrophages on Prussian blue stain. No anaemia yet.
- Iron-deficient erythropoiesis - serum iron falls; serum transferrin (total iron-binding capacity, TIBC) rises; transferrin saturation drops below 15%.
- Iron deficiency anaemia - haemoglobin synthesis is inadequate; microcytic, hypochromic anaemia appears on peripheral smear.
Morphology (Microscopic Features)
Peripheral blood smear - the hallmark findings are:
- Microcytosis - red cells are smaller than normal (MCV < 80 fL)
- Hypochromia - the zone of central pallor is enlarged; in established deficiency, haemoglobin is confined to a narrow peripheral rim (normal central pallor = ~1/3 of cell diameter; in IDA the pallor is > 1/3)
- Poikilocytosis - "pencil cells" (small, elongated red cells) are characteristically seen
- Anisocytosis - variation in red cell size

Fig. 14.22 - Iron deficiency anaemia. Peripheral blood smear showing hypochromic microcytic red cells with a narrow rim of peripheral haemoglobin. (Robbins, Cotran & Kumar - Pathologic Basis of Disease)
Bone marrow:
- Mild to moderate increase in erythroid progenitors (hyperplasia)
- Absent stainable iron in macrophages on Prussian blue stain - a diagnostically significant finding
Laboratory Findings
| Parameter | Finding in IDA |
|---|---|
| Haemoglobin / Haematocrit | Decreased |
| MCV, MCH, MCHC | Decreased (microcytic, hypochromic) |
| Serum iron | Low |
| Serum ferritin | Low (< 12 µg/L) |
| Total iron-binding capacity (TIBC) | Elevated |
| Transferrin saturation | Reduced (< 15%) |
| Serum hepcidin | Low (iron deficiency inhibits hepcidin synthesis) |
| Reticulocyte count | Low or normal (blunted marrow response) |
| Platelet count | Often elevated (for unclear reasons) |
| Erythropoietin | Elevated, but marrow response is blunted |
Clinical Features
In most cases, iron deficiency anaemia is mild and asymptomatic. When symptomatic:
- General: weakness, listlessness, pallor, fatigue
- Nails: koilonychia (spoon-shaped nails), thinning, flattening
- Neurological/behavioural: pica (craving for non-foodstuffs such as clay, dirt, ice - the latter called pagophagia)
- Tongue/mucosa: atrophic glossitis, alopecia, atrophic changes in gastric mucosa
- Rare triad - Plummer-Vinson syndrome: microcytic hypochromic anaemia + atrophic glossitis + oesophageal webs
Depletion of iron-containing enzymes (catalase, cytochromes) throughout the body accounts for many of these non-haematologic manifestations.
Key Concept
"In well-nourished persons, microcytic hypochromic anaemia is not a disease but rather a symptom of another underlying disorder - e.g., colon cancer leading to chronic blood loss." - Robbins & Kumar, Basic Pathology
This principle is clinically critical: every adult with iron deficiency anaemia must be investigated for an occult source of bleeding.
Anaemia of Chronic Inflammation (Differential)
This condition resembles IDA on the smear (it can be normocytic or mildly hypochromic/microcytic) but has a distinct mechanism. IL-6 and other inflammatory mediators drive hepatic hepcidin overproduction, which:
- Inhibits ferroportin in macrophages - trapping iron in storage
- Starves erythroid precursors of iron despite high total body iron stores
- Also directly suppresses erythropoietin production
The key laboratory distinction: ferritin is elevated (an acute-phase reactant) and TIBC is low - the opposite of IDA.
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (pp. 612-615) | Robbins & Kumar - Basic Pathology (p. 393-394)
Prepare a flashcard for iron Deficiency anaemia according to the text above
Generating Image
??
Generating Image
Here is your flashcard for Iron Deficiency Anaemia based on the Robbins content:
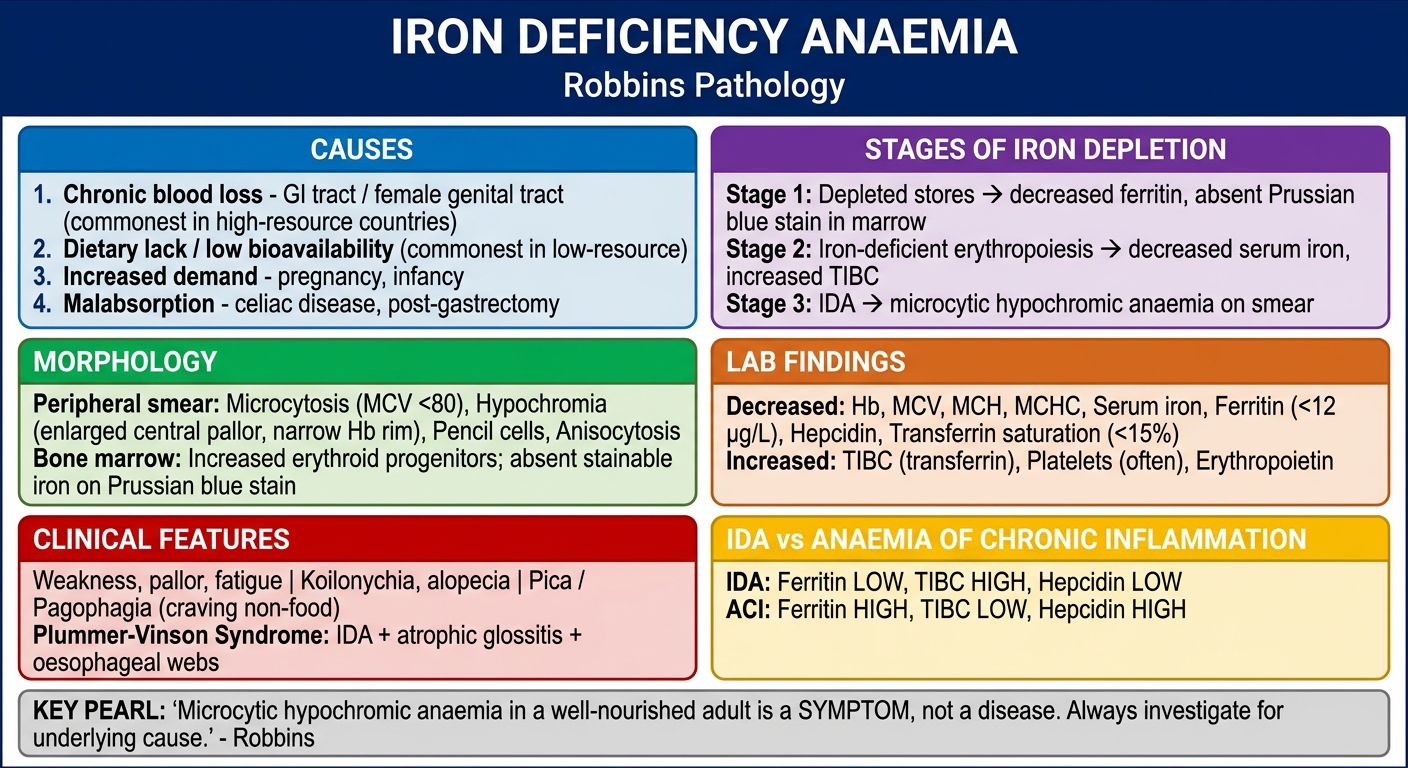
The card covers all the key points from the earlier note:
- Causes (4 categories)
- Stages of iron depletion (stores → erythropoiesis → anaemia)
- Morphology - peripheral smear and bone marrow findings
- Lab findings with the arrows for quick recall
- Clinical features including Plummer-Vinson syndrome
- IDA vs Anaemia of Chronic Inflammation comparison
- The Robbins key pearl at the bottom
This is a shared conversation. Sign in to Orris to start your own chat.