Bells palsy
Reading File
Finding Sources
Searching PubMed
"Bell palsy"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
Bell's palsy facial nerve paralysis clinical photo
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Bell's palsy.
Bell's Palsy (Idiopathic Facial Nerve Palsy)
Right lower motor neurone palsy (Bell's palsy) — note inability to close the right eye, drooping of the right nasolabial fold and mouth corner.

Definition & Diagnostic Criteria
Bell's palsy is a self-limited, idiopathic peripheral facial nerve (CN VII) palsy of acute or subacute onset. The term should only be used after excluding other causes. Taverner's minimum diagnostic criteria are:
- Paralysis or paresis of all muscle groups on one side of the face
- Sudden onset
- Absence of signs of CNS disease
- Absence of signs of ear or cerebellopontine angle disease
"All that palsies are not Bell" — approximately 30–40% of facial palsies have an identifiable alternative cause.
— Cummings Otolaryngology Head and Neck Surgery
Epidemiology
| Feature | Detail |
|---|---|
| Incidence | 23–37 per 100,000/year |
| Peak risk | >65 years (59/100,000); lower in children <13 (13/100,000) |
| Sex | Roughly equal; women predominate <20 yrs, men slightly >40 yrs |
| Bilateral | 0.3% of cases |
| Complete paralysis at onset | ~70% of patients |
| Family history | 8% |
| Recurrence | 9% have a history of previous paralysis |
Anatomy & Lesion Localization
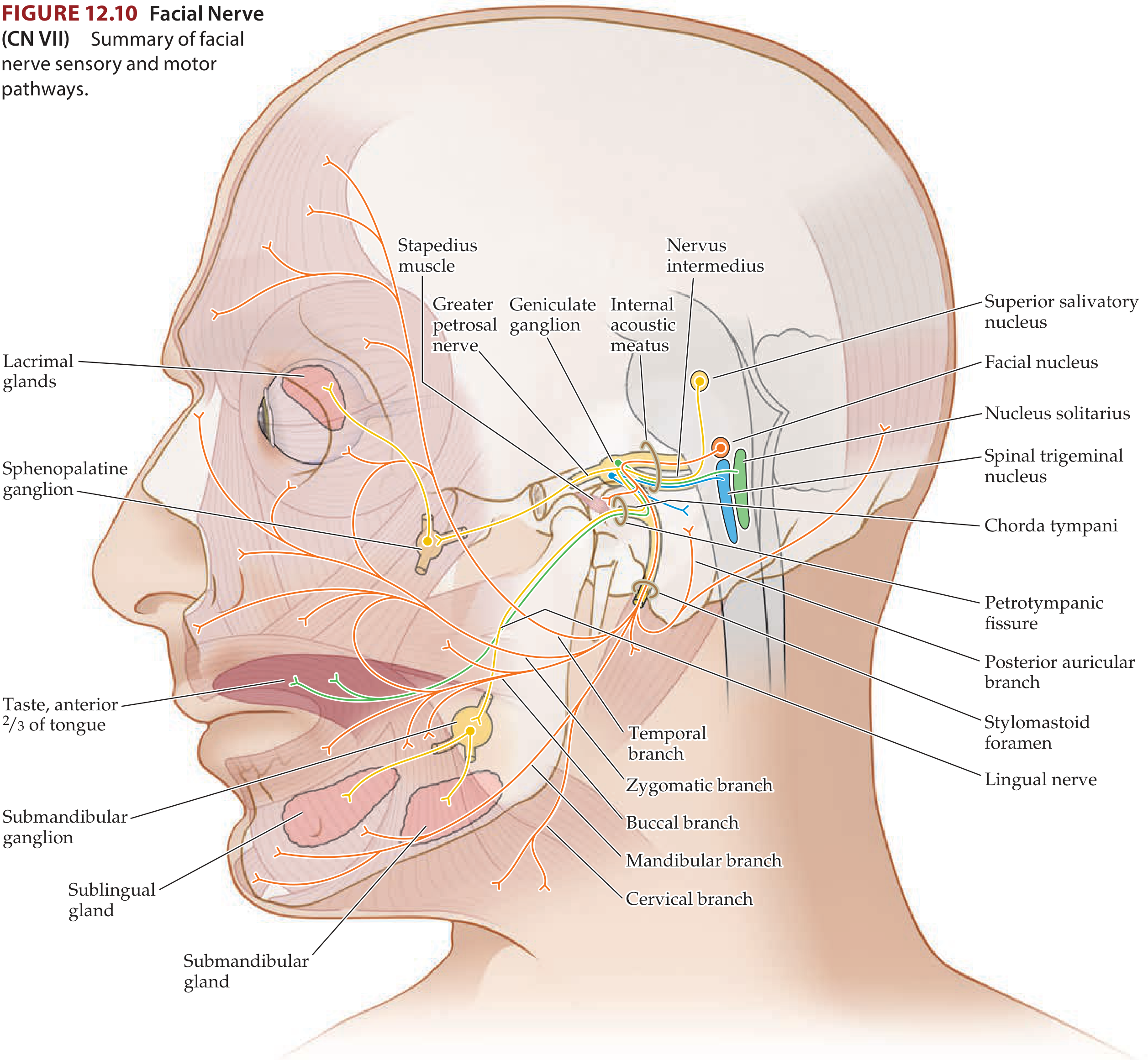
The facial nerve emerges at the ponto-medullary junction, traverses the internal acoustic meatus → geniculate ganglion → stylomastoid foramen → parotid gland → five terminal branches (temporal, zygomatic, buccal, marginal mandibular, cervical).
Key localization principles:
| Level of Lesion | Deficit |
|---|---|
| Above the nucleus (UMN) | Contralateral lower facial weakness only (forehead spared — bilateral cortical representation) |
| Motor nucleus / below (LMN) | Ipsilateral whole face weakness (forehead involved) |
| Geniculate ganglion | Motor + loss of taste (ant. 2/3 tongue) + lacrimation + salivation |
| Stylomastoid foramen | Motor only (most common site in Bell's palsy); lacrimation/taste often preserved |
Bell's palsy lesion is classically at the meatal foramen / labyrinthine segment, with diffuse demyelination throughout the intratemporal course.
Etiology & Pathogenesis
The most widely accepted theory is reactivation of latent HSV-1 in the geniculate ganglion:
- HSV-1 DNA has been identified in geniculate ganglion tissue of autopsy specimens
- Murakami et al. detected HSV DNA by PCR in endoneurial fluid of Bell's palsy patients (not in controls)
- There is no seasonal clustering, supporting reactivation rather than new infection
- VZV reactivation is also implicated (and, when vesicles are present, defines Ramsay Hunt syndrome)
- Proposed mechanism: viral neuropathy → oedema → ischaemic compression within the bony facial canal
Pathologically: diffuse demyelination with wallerian degeneration, most severe at the labyrinthine segment and meatal foramen; lymphocytic infiltration of the greater petrosal nerve.
Clinical Features
Motor: Ipsilateral weakness of entire hemiface — inability to close the eye (lagophthalmos), flattening of the nasolabial fold, drooping of the mouth, loss of forehead wrinkling.
Sensory/autonomic associations (from polyneuropathy data):
- Hypesthesia/dysesthesia of CN V or IX — 80%
- Hyperacusis (stapedius dysfunction) — up to 30%
- Retroauricular or facial pain
- Taste disturbance (chorda tympani)
- Reduced lacrimation (greater petrosal nerve)
- Vagal motor weakness — 20%
Bell's phenomenon: On attempted eye closure, the eye rolls upward — protective reflex, visible as white sclera when eyelid closure is incomplete.
Differential Diagnosis
| Acute | Chronic/Progressive |
|---|---|
| Ramsay Hunt syndrome (VZV + vesicles) | Parotid malignancy |
| Lyme disease | Facial nerve schwannoma |
| Guillain-Barré syndrome | Glomus tumour |
| Otitis media / cholesteatoma | Metastatic tumour |
| Sarcoidosis (often bilateral) | Cholesteatoma |
| HIV infection | — |
| Melkersson-Rosenthal syndrome | — |
| Temporal bone fracture | — |
Red flags requiring urgent MRI: slow/insidious onset, progressive course, other neurological signs, hearing loss, bilateral palsy (check CXR + SACE for sarcoidosis).
Investigations
- Clinical diagnosis in typical cases; no routine imaging needed
- Electroneuronography (ENoG): predicts prognosis — >90% degeneration by days 3–14 is a poor prognostic sign
- Schirmer test (lacrimation), stapedial reflex, taste testing — topographic localization (limited accuracy)
- MRI with gadolinium if atypical, progressive, or recurrent — enhancing facial nerve can be seen
- If bilateral: CXR + serum ACE (sarcoidosis), Lyme serology
Treatment
1. Corticosteroids ✅ (First-line)
Prednisolone 60–80 mg/day for 1 week, then taper over 1 week, started within 48–72 hours of onset. Strong evidence reduces risk of unsatisfactory recovery.
2. Antivirals ⚠️ (Adjunct)
Acyclovir or valaciclovir combined with corticosteroids — evidence suggests benefit in reducing long-term sequelae (synkinesis, crocodile tears) even though antiviral alone is not sufficient. Most guidelines recommend adding antivirals to steroids, particularly in severe/complete palsy.
3. Eye Protection 👁️ (Essential)
- Lubricating eye drops (artificial tears) during the day
- Eye ointment and patching at night
- Critical if CN V sensation is also impaired (neurotrophic risk)
4. Physical Therapy
- Neuromuscular re-education, facial exercises, and mirror biofeedback
- Systematic reviews (Nakano et al., 2024 [PMID 37149416]; Varelas et al., 2025 [PMID 39647183]) suggest benefit for recovery and reduction of sequelae
5. Surgical Decompression ❌
Not recommended — does not improve outcomes in Bell's palsy. Reserved only for refractory cases with >90% ENoG degeneration in select specialist centres.
Prognosis
- ~70% of patients recover completely without treatment
- 30% have incomplete paralysis at onset → nearly all recover fully
- Of those with complete paralysis: ~70% still recover fully; ~15% have permanent sequelae
- Poor prognostic factors: complete paralysis, age >60, diabetes, hypertension, severe pain, >90% ENoG degeneration
- Sequelae of aberrant regeneration:
- Synkinesis (involuntary eye closure with mouth movement)
- Crocodile tears (lacrimation while eating — gustatory tearing)
- Contracture of facial muscles
Ramsay Hunt Syndrome (Distinguish!)
VZV reactivation with facial palsy + vesicular rash (ear canal, auricle, or palate) ± sensorineural hearing loss and vertigo. Worse prognosis than Bell's palsy — only ~50% recover fully. Treat with both corticosteroids + antivirals (acyclovir 800 mg 5×/day or valaciclovir).
Recent Evidence
- A 2023 meta-analysis (PMID 37103913, JAMA Otolaryngol) found a small but significant association between SARS-CoV-2 vaccination/infection and Bell's palsy
- Laser therapy has emerging evidence (PMID 39546047, 2024) but is not yet standard of care
- Physical therapy meta-analyses support facial exercises as adjuncts to pharmacotherapy
Sources: Cummings Otolaryngology Head and Neck Surgery · Bradley and Daroff's Neurology in Clinical Practice · Kanski's Clinical Ophthalmology · Gray's Anatomy for Students
) Facial nerve - coarse ,branches , levels of lesions with its features Feature of lmn and umn facial palsy and treatment of Bell’s palsy
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
facial nerve course branches anatomy diagram CN VII
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have everything needed for a comprehensive, well-structured answer.
Facial Nerve (CN VII) — Complete Overview
1. Fiber Components of CN VII
CN VII is a mixed nerve containing four fiber types:
| Fiber Type | Origin/Nucleus | Function |
|---|---|---|
| Branchial motor | Facial nucleus (pons) | Muscles of facial expression, stylohyoid, posterior digastric, stapedius |
| Parasympathetic (GVE) | Superior salivatory nucleus | Via greater petrosal nerve → lacrimal, nasal, palatine glands; via chorda tympani → submandibular & sublingual glands |
| Special sensory (SVA) | Geniculate ganglion | Taste — anterior 2/3 of tongue (via chorda tympani → lingual nerve → nucleus solitarius) |
| General somatic sensory | Geniculate ganglion | Sensation from concha, external auditory canal, earlobe |
2. Course of the Facial Nerve — Six Segments
| Segment | Length | Key Landmarks |
|---|---|---|
| 1. Intracranial | 17–24 mm | Pons (lower border) → internal auditory canal (IAC) |
| 2. Meatal | 8–10 mm | IAC fundus (anterosuperior quadrant) → meatal foramen |
| 3. Labyrinthine | 4 mm | Meatal foramen → geniculate ganglion; narrowest point — most susceptible to inflammation (Bell's palsy) |
| 4. Tympanic | 11 mm | Geniculate ganglion → 2nd genu |
| 5. Mastoid/Vertical | 13 mm | 2nd genu → stylomastoid foramen |
| 6. Extratemporal | — | Stylomastoid foramen → parotid gland → 5 terminal branches |
Key anatomical notes:
- The intrapontine fibers loop dorsally around the abducens nucleus → form the facial colliculus on the floor of the 4th ventricle (explains CN VI + VII palsy together in pontine lesions)
- Enters IAC together with CN VIII
- The geniculate ganglion (at the genu) carries sensory cell bodies and gives off the greater petrosal nerve
3. Branches and Their Functions
Intratemporal Branches
| Branch | Origin | Function |
|---|---|---|
| Greater (superficial) petrosal nerve | Geniculate ganglion | Parasympathetic → pterygopalatine ganglion → lacrimal gland, nasal & palatine glands |
| Nerve to stapedius | Mastoid segment | Motor → stapedius muscle (reflex tensor of ossicles; loss → hyperacusis) |
| Chorda tympani | Just above stylomastoid foramen | Taste (ant. 2/3 tongue) + parasympathetic → submandibular & sublingual glands |
Extratemporal Branches (mnemonic: To Zanzibar By Motor Car)
| Branch | Muscles Supplied |
|---|---|
| Temporal | Frontalis, corrugator, orbicularis oculi (upper) |
| Zygomatic | Orbicularis oculi (lower), zygomaticus |
| Buccal | Buccinator, orbicularis oris, muscles of the upper lip |
| Marginal mandibular | Depressor anguli oris, depressor labii inferioris, mentalis |
| Cervical | Platysma |
Also: Posterior auricular nerve (just after stylomastoid foramen) → occipitalis, auricular muscles, posterior scalp.
4. Levels of Lesions and Their Features
| Level | Lesion Site | Motor (Face) | Taste (Ant. 2/3) | Lacrimation | Salivation | Hyperacusis | Other |
|---|---|---|---|---|---|---|---|
| A | Stylomastoid foramen | Ipsilateral all face ✅ | ❌ Intact | ❌ Intact | ❌ Intact | ❌ Intact | Most common site (Bell's palsy) |
| B | Facial canal — above chorda tympani, below geniculate | All face ✅ | ✅ Lost | ❌ Intact | ✅ Lost | ❌ Intact | Also reduced salivation |
| B+ | Facial canal — above geniculate ganglion (but below stapedius) | All face ✅ | ✅ Lost | ❌ Intact | ✅ Lost | ✅ Present | Ramsay Hunt zone |
| C | Proximal to geniculate ganglion | All face ✅ | ✅ Lost | ✅ Lost | ✅ Lost | ✅ Present | Geniculate herpes (Ramsay Hunt); also loss of lacrimation |
| Pons (nucleus/fascicles) | Pontine lesion | All face ✅ (ipsilateral) | ❌ Intact | ❌ Intact | ❌ Intact | — | CN VI palsy also present (facial colliculus); Millard-Gubler syndrome |
| Cerebral cortex / corticobulbar | Above facial nucleus | Lower face only (contralateral) — forehead spared | ❌ | ❌ | ❌ | ❌ | Associated hemiparesis, aphasia |
Mnemonic for lesion levels ascending from stylomastoid foramen: "Some Lovers Go Home Crying" Stylomastoid → taste Loss → Hyperacusis → Greater petrosal (lacrimation) → Cortex
5. UMN vs. LMN Facial Palsy — Key Distinction
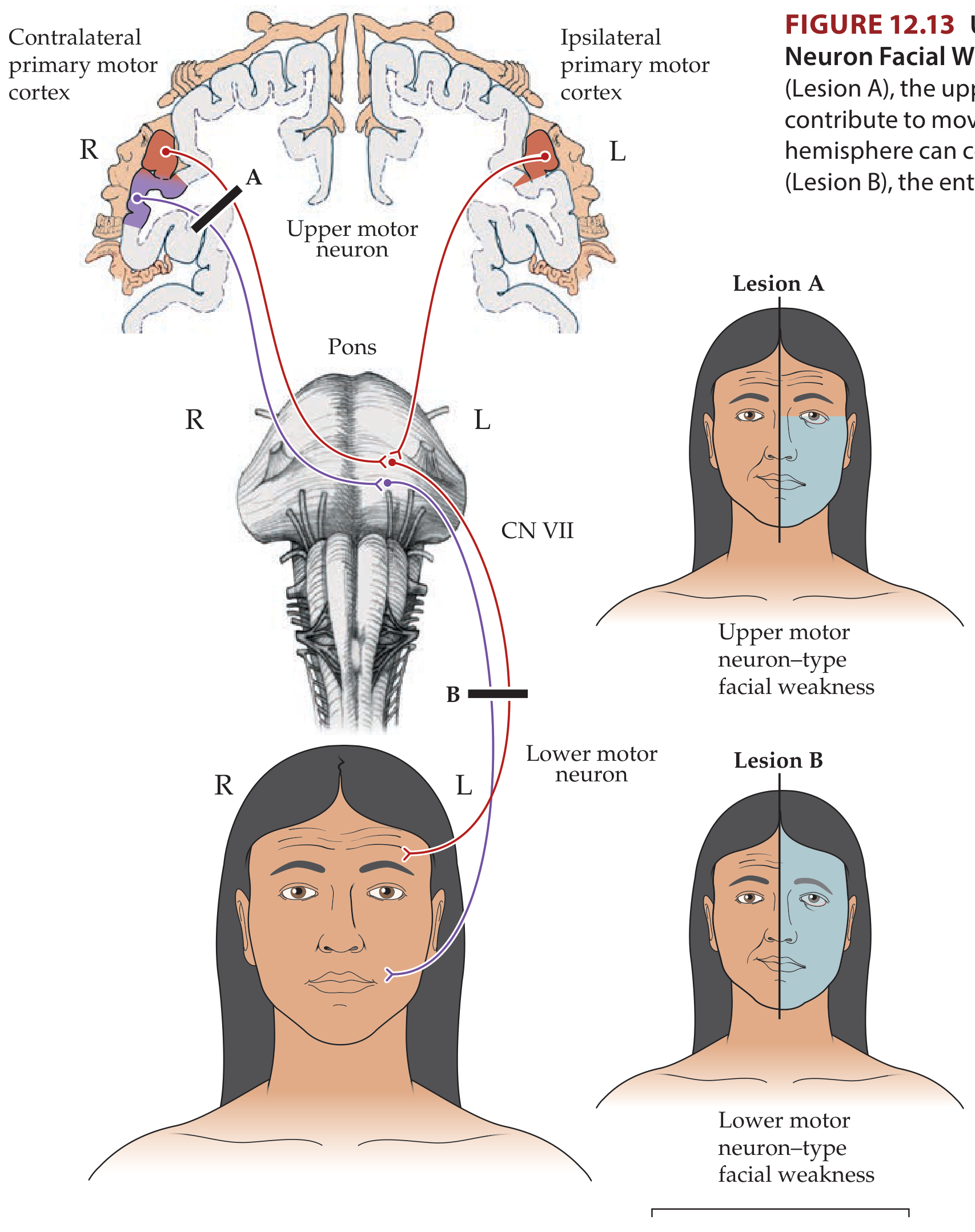
| Feature | UMN (Central) | LMN (Peripheral) |
|---|---|---|
| Side affected | Contralateral lower face | Ipsilateral entire face |
| Forehead | ✅ Spared (bilateral cortical input) | ❌ Involved — cannot wrinkle forehead |
| Eye closure | ✅ Preserved (mild weakness possible) | ❌ Lagophthalmos — incomplete eye closure |
| Bell's phenomenon | Not seen | ✅ Present (eye rolls upward on attempted closure) |
| Nasolabial fold | Effaced contralaterally (lower only) | Effaced on same side |
| Taste | Normal | Lost (if chorda tympani involved) |
| Hyperacusis | ❌ | ✅ Possible |
| Emotional movements | May be selectively impaired (volitional preserved) | Both volitional AND emotional affected |
| Associated signs | Hemiparesis, aphasia, hemisensory loss | None (Bell's = isolated CN VII) |
| Causes | Stroke, tumour, MS, abscess | Bell's palsy, Ramsay Hunt, parotid tumour, trauma, Lyme |
Why is the forehead spared in UMN lesions?
The upper facial nucleus (forehead, orbicularis oculi) receives bilateral corticobulbar input. A unilateral UMN lesion leaves the intact contralateral cortex still driving the upper face — hence the forehead is spared. The lower facial nucleus receives only contralateral input, so it is fully paralysed.
6. Treatment of Bell's Palsy
A. Corticosteroids (First-line — Grade A evidence)
- Prednisolone 60–80 mg/day × 7 days, then taper over 7 days (alternative: 25 mg twice daily × 10 days)
- Must start within 48–72 hours of onset
- Increases complete recovery from ~63% → ~83% at 3 months
- Mechanism: reduces inflammatory oedema within the bony facial canal
B. Antivirals (Adjunct to steroids)
- Acyclovir 400 mg 5× daily × 7–10 days, or valaciclovir 1g TDS × 7 days
- Antiviral alone = no benefit
- Steroids + antivirals = added benefit in reducing long-term sequelae (synkinesis, crocodile tears)
- Especially indicated in severe/complete palsy and Ramsay Hunt syndrome
C. Eye (Corneal) Protection — Essential
- Artificial tear drops during the day
- Lubricating ointment + eye patch at night
- Critical to prevent exposure keratopathy (risk is greatest when CN V sensation is also reduced)
D. Physical Therapy
- Facial neuromuscular re-education, exercises, mirror biofeedback
- Useful as adjunct; recent meta-analyses support benefit in recovery and synkinesis prevention
E. Surgical Decompression
- Not recommended in routine Bell's palsy
- No RCT evidence of benefit
- May be considered by specialists in selected cases with >90% degeneration on ENoG within 14 days
Summary Algorithm
Onset ≤72 hrs?
├── YES → Prednisolone + Acyclovir + Eye care
└── Severe/Complete palsy → definitely add antivirals
├── ENoG at day 3–14 if no recovery
└── >90% degeneration → specialist referral
Prognosis
- ~70% recover completely without treatment
- Treatment improves this to ~83%
- ~10% have permanent sequelae
- Sequelae of aberrant regeneration: synkinesis (jaw winking), crocodile tears (gustatory tearing), facial contracture
Sources: K.J. Lee's Essential Otolaryngology · Adams & Victor's Principles of Neurology · Neuroanatomy through Clinical Cases (Blumenfeld) · Goldman-Cecil Medicine · Cummings Otolaryngology · Kanski's Clinical Ophthalmology
This is a shared conversation. Sign in to Orris to start your own chat.