
Interpret
Checking Date & Time
Reading File
Finding Sources
Searching PubMed
HbA1c 7% diabetes management glycemic target
Here is the interpretation of Mr. Sunil Malhotra's HbA1c report:
HbA1c Report Interpretation
Patient: Mr. Sunil Malhotra | 51 years, Male | Tested: 23 Apr 2026
Key Result
| Test | Value | Reference Range | Status |
|---|---|---|---|
| HbA1c (Glycosylated Hemoglobin) | 7.00% | 4.2 – 5.7% | 🔴 Above normal |
| Average Estimated Glucose (eAG) | 154.20 mg/dL | — | Elevated |
What This Means
HbA1c of 7.00% = Known/Diagnosed Diabetic on Treatment
According to ADA (American Diabetes Association) criteria:
| Category | HbA1c |
|---|---|
| Non-diabetic | < 5.7% |
| Prediabetes (At Risk) | 5.7 – 6.4% |
| Diabetes (Diagnostic threshold) | ≥ 6.5% |
| Mr. Malhotra's result | 7.00% |
At 7.00%, this result is above the diagnostic threshold for diabetes (≥6.5%) but is exactly at the ADA therapeutic goal of <7.0% for adults >19 years. This is a borderline/at-goal reading.
Clinical Interpretation
Two possible scenarios:
-
If he is already on diabetes treatment: His glycemic control is at the ADA target (<7.0%). This is considered good diabetic control. The ADA recommends that action be taken if HbA1c exceeds 8.0%.
-
If he has NOT been previously diagnosed or treated: An HbA1c of 7.0% confirms Type 2 Diabetes Mellitus (well above the 6.5% threshold), and treatment should be initiated promptly.
Average Estimated Glucose (eAG)
An eAG of 154.20 mg/dL represents the average blood sugar over the past 2–3 months. Normal fasting blood glucose is 70–100 mg/dL, so his average glucose is running significantly above normal, consistent with diabetes.
What Should Be Done Next
- Consult a physician/diabetologist to review current medications (if on treatment) or to initiate therapy (if newly diagnosed).
- Lifestyle modifications: Low-glycemic diet, regular aerobic exercise (150 min/week), weight management.
- Monitor for complications: Kidney function (eGFR, urine albumin), eye examination (retinopathy), foot examination, blood pressure, and lipid profile.
- Repeat HbA1c in 3 months to track trends — the ADA notes trends are a better indicator of diabetic control than a single value.
- Screen for vitamin B12 deficiency if on Metformin, as it can falsely lower HbA1c.
Important Cautions (from the lab report)
- HbA1c can be falsely low in hemolytic disease, recent blood transfusion, blood loss, or with drugs like dapsone, ribavirin, antiretrovirals, trimethoprim.
- HbA1c can be falsely high in iron deficiency, B12 deficiency, polycythemia, or high-dose aspirin use.
- If accuracy is in doubt, a plasma fructosamine test evaluates glycemic control over 15 days instead.
Summary
Mr. Malhotra's HbA1c of 7.0% indicates diabetes mellitus. If he is on treatment, his control is at the ADA therapeutic goal — commendable, but needs continued monitoring. If untreated, diabetes management should begin immediately. Regular follow-up and screening for complications are essential.
— Based on ADA Standards of Medical Care in Diabetes 2023; Tietz Textbook of Laboratory Medicine, 7th Ed.
How to initiate treatment for diabetes
Finding Sources
Searching PubMed
type 2 diabetes initial treatment guidelines
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
I now have comprehensive information. Here is a full evidence-based guide on initiating treatment for Type 2 Diabetes:
Initiating Treatment for Type 2 Diabetes Mellitus
(Relevant to Mr. Sunil Malhotra, HbA1c 7.0%)
Treatment Algorithm
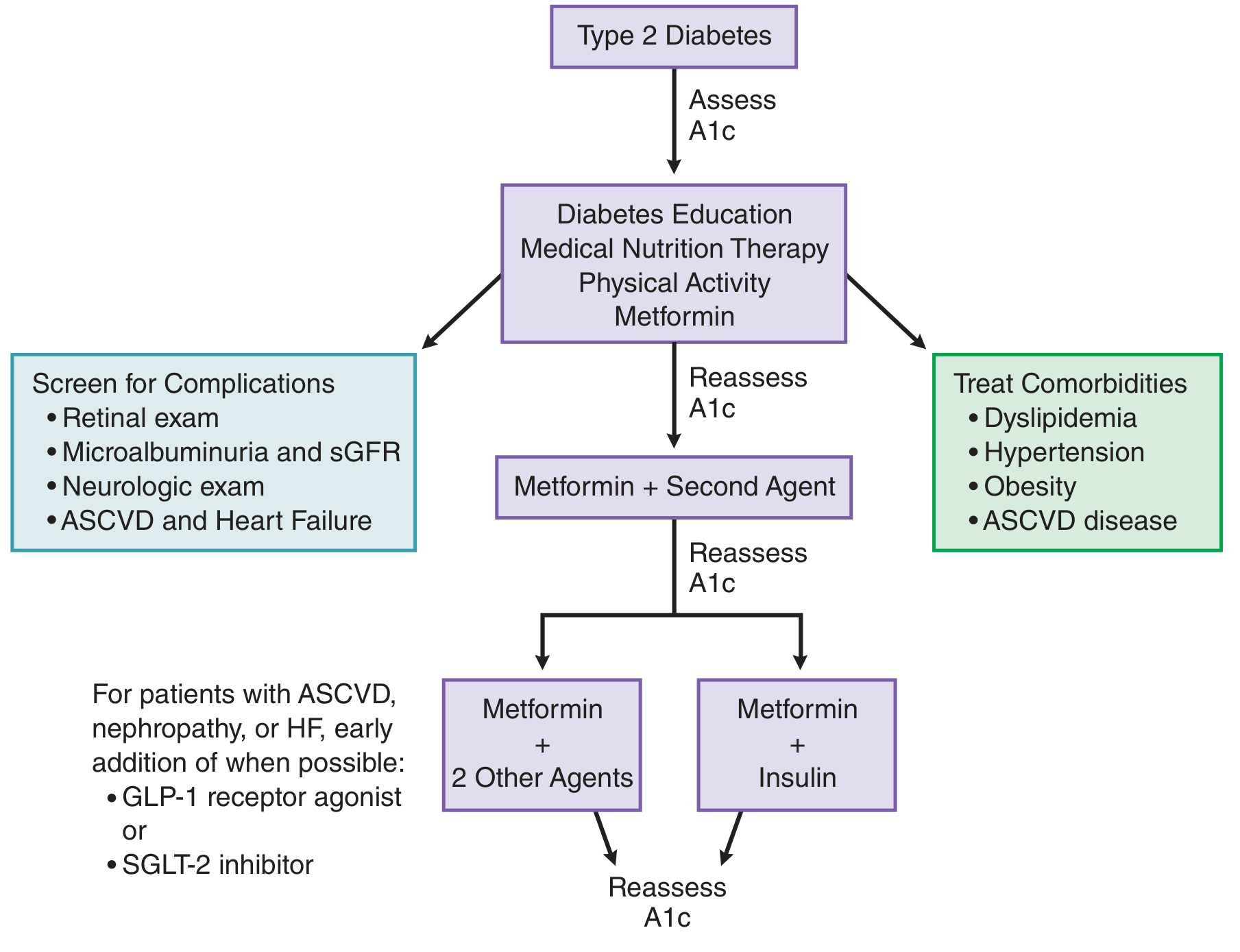
Step 1 — Diabetes Education + Lifestyle First
At the time of diagnosis, all patients should receive:
| Intervention | Details |
|---|---|
| Diabetes Education | Understanding of blood sugar monitoring, medications, hypoglycemia recognition |
| Medical Nutrition Therapy (Diet) | Low-glycemic index foods, reduced simple carbs/sugars, high fiber, portion control |
| Physical Activity | ≥150 min/week of moderate aerobic exercise (brisk walking, cycling, swimming) |
| Weight Management | Even 5–10% weight loss significantly improves glycemic control |
These lifestyle measures are initiated simultaneously with medication, not sequentially.
Step 2 — First-Line Drug: Metformin
Metformin is the universal first-line pharmacological therapy for Type 2 Diabetes — endorsed by the ADA, WHO, and all major guidelines.
Why Metformin?
- Reduces HbA1c by ~1–2%
- Does not cause weight gain (may cause mild weight loss)
- Does not cause hypoglycemia as monotherapy
- Low cost
- Decades of safety data
- Reduces microvascular complications
Dosing (Start Low, Go Slow)
| Phase | Dose |
|---|---|
| Week 1–2 | 500 mg once daily with dinner |
| Week 3–4 | 500 mg twice daily (with meals) |
| Target | 1000 mg twice daily (2000 mg/day total) |
| Maximum | 2550 mg/day |
Always take with food to minimise GI side effects.
Common Side Effects
- Nausea, bloating, diarrhea, abdominal cramps (10–25% of patients, usually transient)
- Reduced vitamin B12 absorption — monitor B12 annually
- Rare: lactic acidosis (mainly in renal failure)
When NOT to use Metformin (Contraindications)
- eGFR < 30 mL/min (severe kidney disease)
- Decompensated heart failure
- Severe liver disease / chronic alcohol abuse
- Severe pulmonary disease
- Hold before contrast dye procedures (CT scan with contrast, angiography)
Step 3 — Reassess HbA1c in 2–3 Months
- Target: HbA1c < 7.0% (for most adults)
- If target is not reached, add a second agent
Step 4 — Adding a Second Agent (if needed)
Choose based on the patient's comorbidities:
| Patient Profile | Preferred Add-on Drug |
|---|---|
| Established cardiovascular disease (ASCVD) | GLP-1 receptor agonist (liraglutide, semaglutide, dulaglutide) |
| Heart failure or diabetic kidney disease | SGLT-2 inhibitor (empagliflozin, dapagliflozin, canagliflozin) |
| Obesity / weight loss needed | GLP-1 agonist or SGLT-2 inhibitor |
| Cost-sensitive patients | Sulfonylurea (glimepiride, glipizide) or thiazolidinedione (pioglitazone) |
| Minimizing hypoglycemia risk | DPP-4 inhibitor (sitagliptin, vildagliptin) or GLP-1 agonist |
Step 5 — Further Escalation
If dual therapy still doesn't achieve target:
- Metformin + 2 other oral agents, OR
- Metformin + Basal insulin (e.g., Glargine/Degludec at bedtime)
What Else to Start at Diagnosis
| Action | Why |
|---|---|
| Screen for retinopathy | Retinal exam at diagnosis |
| Check urine albumin/creatinine ratio | Early nephropathy |
| Check blood pressure | Target <130/80 mmHg in diabetics |
| Check lipid profile | Most T2DM patients benefit from a statin |
| Check kidney function (eGFR, creatinine) | Before starting metformin |
| Foot examination | Neuropathy and vascular disease |
| Vaccinations | Flu, pneumococcal, hepatitis B |
For Mr. Malhotra Specifically (HbA1c 7.0%)
His HbA1c is exactly at the therapeutic target of <7.0%. This means:
- If newly diagnosed and untreated: Start metformin + lifestyle changes — his HbA1c is already borderline, so the response to these measures should bring him below 7%.
- If already on treatment: Current regimen is working; continue and recheck in 3 months.
- Escalation to a second drug is not immediately needed unless HbA1c climbs above 7%.
— Goodman & Gilman's Pharmacological Basis of Therapeutics; Swanson's Family Medicine Review; Tietz Textbook of Laboratory Medicine, 7th Ed.
Recent evidence note: A 2025 network meta-analysis (PMID 40300775) confirms metformin monotherapy as preferred initial therapy in early T2DM, consistent with the above recommendations.
This is a shared conversation. Sign in to Orris to start your own chat.