Can you tell me the diffrence between pulsus bisferians and pulsus dicroticus....from basics in crsip
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed. Here is a crisp, from-basics comparison.
Pulsus Bisferiens vs Pulsus Dicrotic (Dicrotic Pulse)
1. The Normal Arterial Pulse — Start Here
Every normal arterial waveform has:
- A systolic upstroke → rapid rise as LV ejects blood
- A peak (percussion wave)
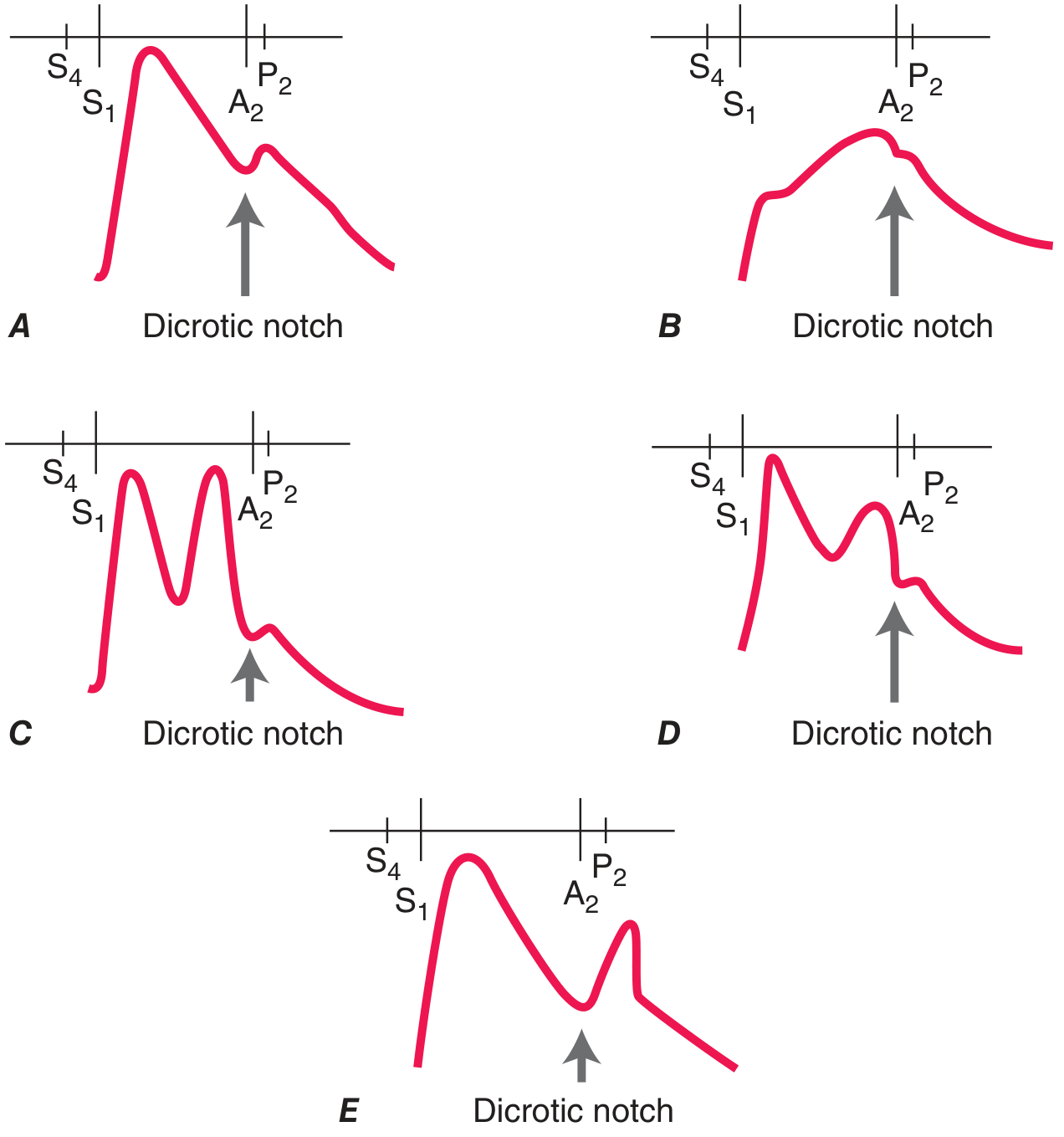
- A dicrotic notch — a small incisure caused by aortic valve closure (marks the end of systole / start of diastole)
- A dicrotic wave — a tiny secondary rise just after the notch, caused by elastic recoil of the aorta. Normally small and not palpable.
2. Pulsus Bisferiens
Etymology
Bis = twice, feriens = striking → "striking twice"
What it is
A double-peaked pulse where BOTH peaks occur within systole (before the dicrotic notch / before A₂).
The two peaks have names:
| Peak | Name | Cause |
|---|---|---|
| 1st | Percussion wave | Rapid early ejection of blood |
| 2nd | Tidal wave | Pressure wave reflected back from the periphery |
In a normal pulse the tidal wave is smaller and merges into the first peak. In bisferiens, the tidal wave is exaggerated and becomes a distinct second peak — still in systole.
Mechanisms (two main situations):
A. Aortic Regurgitation (AR) — especially severe AR or mixed AS+AR with dominant AR
- Large stroke volume is ejected rapidly → tall, fast percussion wave
- The volume then causes an exaggerated reflected wave = tidal wave
- Two distinct systolic peaks result
B. Hypertrophic Obstructive Cardiomyopathy (HOCM)
- In early systole, the hypertrophied LV contracts forcefully and unobstructed → rapid upstroke = 1st peak (percussion wave)
- Mid-systole: dynamic outflow obstruction develops (SAM of MV) → rapid fall in pressure = trough
- Late systole: obstruction partially relieves → pressure rises again = 2nd peak (tidal wave)
- This creates the classic "spike and dome" pattern on the aortic pressure tracing
Features:
- Pulse pressure is wide (in AR) or normal–brisk (in HOCM)
- Both peaks are in SYSTOLE (between S₁ and A₂)
- Palpable at the carotid artery — best felt there; harder to feel at radial
- Amplitude is increased or normal
- Seen also in patent ductus arteriosus, ventricular septal defect (rarely)
3. Pulsus Dicrotic (Dicrotic Pulse)
Etymology
Di = two, krotos = beat → "double beat"
What it is
A double-peaked pulse where the two peaks are on EITHER SIDE of the dicrotic notch — the 1st peak in systole, the 2nd in diastole. It results from an exaggeration of the normally imperceptible dicrotic wave.
Mechanism
- In states of low cardiac output / low systemic vascular resistance (SVR):
- The aorta is filled with reduced volume
- Peripheral resistance is low → the elastic aorta's recoil wave (normally small) becomes disproportionately prominent
- The dicrotic notch deepens and the dicrotic wave crosses over into palpable territory
- Net result: one peak in systole + one distinctly palpable peak in early diastole
Causes (low output + low SVR):
- Sepsis / septic shock
- Severe heart failure (decompensated)
- Hypovolemic shock
- Cardiac tamponade
- After aortic valve replacement (transiently)
Features:
- Pulse pressure is narrow
- Amplitude is low / feeble
- First peak in systole (before A₂), second peak in DIASTOLE (after A₂)
- The dicrotic notch is exaggerated and the dicrotic wave becomes palpable
4. The Core Difference — One Table
| Feature | Pulsus Bisferiens | Pulsus Dicrotic |
|---|---|---|
| Meaning | Twice-striking | Double-beat |
| Number of peaks | Two | Two |
| Location of 2nd peak | Systole (before A₂) | Diastole (after A₂) |
| Pulse pressure | Wide (AR) / brisk (HOCM) | Narrow |
| Amplitude | Increased / normal | Low, feeble |
| Underlying state | Volume overload / dynamic obstruction | Low output, low SVR |
| Key causes | AR, HOCM, mixed AS+AR | Sepsis, heart failure, tamponade, hypovolemia |
| Mechanism of 2nd peak | Exaggerated reflected (tidal) wave in systole | Exaggerated dicrotic (aortic recoil) wave in diastole |
| Palpability | Best at carotid | Best at carotid or femoral |
5. Memory Hook
Bisferiens = Both peaks Before (both in systole, before A₂) → think of the B–B rule. Dicrotic = second peak Delayed into Diastole → think D–D rule.
Or visually: in bisferiens the trough between the two peaks sits above the dicrotic notch; in the dicrotic pulse the trough is the dicrotic notch.
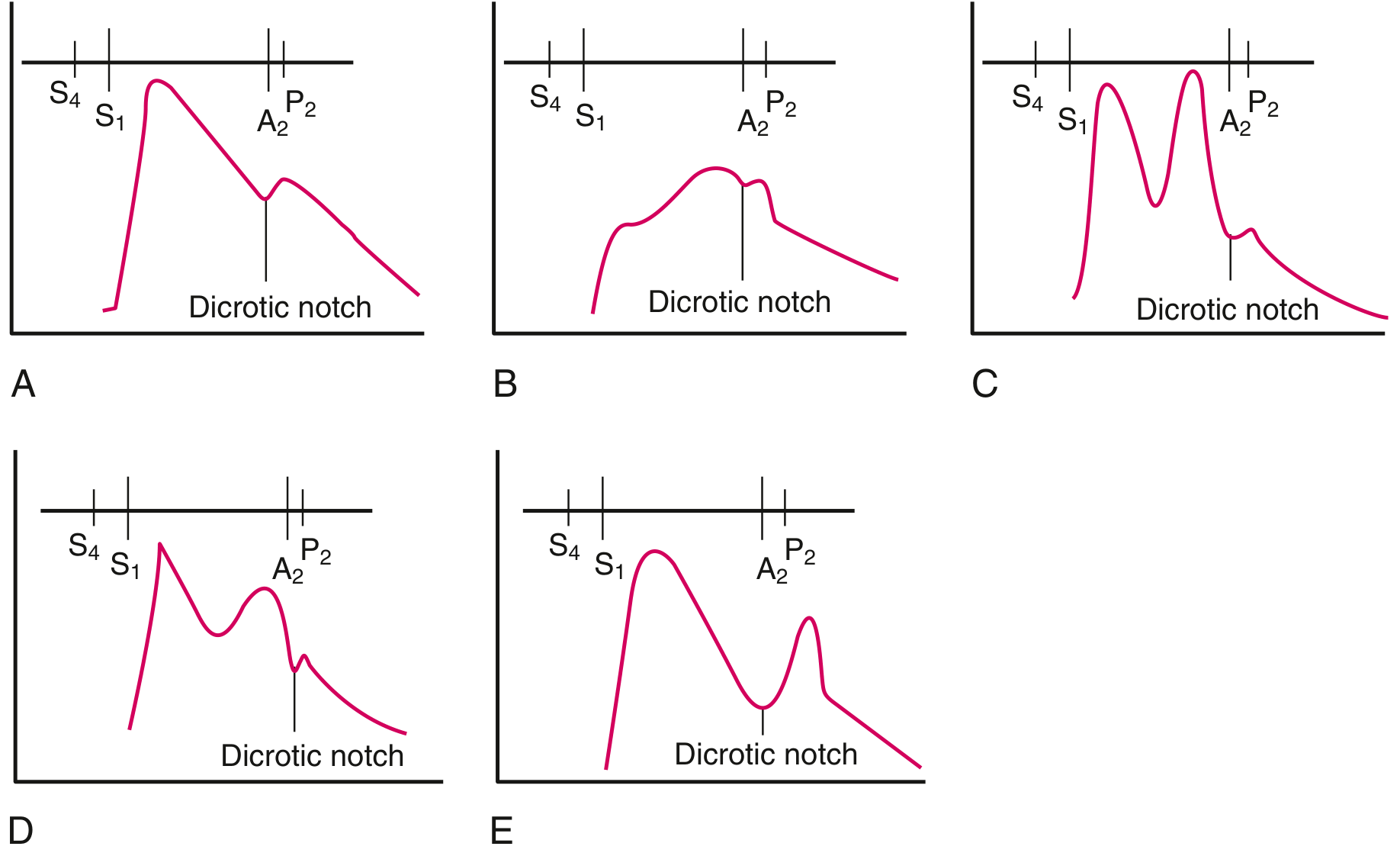
(C = pulsus bisferiens in AR; D = bisferiens in HOCM; E = dicrotic pulse — Goldman-Cecil Medicine)
Sources:
- Goldman-Cecil Medicine, Fig. 3-9
- Harrison's Principles of Internal Medicine 22e, Fig. 246-2
- Fuster & Hurst's The Heart, 15th ed., "Abnormalities of Arterial Pulse"
can you tell me why in case of Mitral valve prolapse , we see rapid increase in pressure of atrium in late diastole unlike classic mitral regurgitation resulting in cresendo decresendo type of murmur in MVP, but pansystolic murmur in MR....from std book in v short
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have everything needed. Here's the crisp answer.
Why MVP gives a Late Systolic Crescendo Murmur, not Pansystolic
First, understand the pressure gradient that drives a murmur
A murmur is produced only when LV pressure > LA pressure AND there is a structural incompetence allowing flow back into the LA. The gradient determines when in systole the murmur begins and ends.
Classic MR (rheumatic / annular dilatation / flail leaflet)
The mitral valve is incompetent from the very start of systole (from S₁ onward):
- The moment isovolumetric contraction begins, LV pressure immediately exceeds LA pressure
- The faulty valve allows regurgitation from S₁ all the way to S₂ / A₂
- LV–LA gradient is large and relatively constant throughout systole
- Result: plateau-shaped, holosystolic (pansystolic) murmur, filling the entire systole uniformly
Mitral Valve Prolapse — the key difference
The valve is structurally normal at the start of systole. The leaflets coapt well in early systole. Regurgitation only begins after prolapse occurs:
What happens beat by beat:
| Phase | LV volume | What happens at the MV |
|---|---|---|
| Early systole | Large | Leaflets coapt normally, no regurgitation, no murmur |
| Mid-systole | LV begins to shrink | Leaflets have slack, start to bow into LA |
| Mid-to-late systole | LV smaller | Chordae suddenly become taut → CLICK (sudden tensing) |
| Late systole | LV at its smallest | Leaflets prolapse past coaptation point → regurgitation begins |
As soon as the leaflets prolapse past coaptation, the LV–LA gradient is created and regurgitant flow begins. From that moment until A₂, the gradient is increasing (LV is still generating pressure while the LA is receiving regurgitant volume and its pressure is rising). This progressive increase in gradient produces a crescendo quality. The murmur reaches its peak at S₂ → crescendo murmur ending at S₂.
Because the regurgitant orifice starts small (partial prolapse) and enlarges progressively as the leaflets bow further, the murmur goes crescendo-decrescendo in shape — peaking just before or at A₂.
Net result: Mid-to-late systolic crescendo (±decrescendo) murmur, with a preceding midsystolic click.
Your question about LA pressure rising in "late diastole"
A small clarification: the relevant pressure event in MVP is not a late diastolic LA pressure rise — it is a late systolic phenomenon. The regurgitation (and murmur) begins in late systole when the prolapse occurs. The LA pressure rises because of the regurgitant jet entering the LA in late systole — that's when the v-wave in the LA pressure tracing peaks. In contrast, in chronic MR the v-wave builds throughout the whole of systole.
One-line summary
In MVP, the valve is competent in early systole and only fails when prolapse occurs in mid-to-late systole — so regurgitation (and therefore the murmur) only starts then, giving a late systolic crescendo murmur. In classic MR, the valve is incompetent from S₁, so the murmur is pansystolic.
Sources:
- Harrison's Principles of Internal Medicine 22e, MVP — Auscultation section
- Fuster & Hurst's The Heart 15e, "AV Valve Regurgitation: Holosystolic Murmurs"
- Goldman-Cecil Medicine, Physical Examination — MVP
This is a shared conversation. Sign in to Orris to start your own chat.