tough vivaquestionsand answersfor A SCAN in opthalmology for residency
A-scan biometry ophthalmology residency viva questions axial length IOL power calculation
https://eyewiki.org/Biometry_for_Intra-Ocular_Lens_(IOL)_Pow…
A-scan biometry viva questions ophthalmology immersion vs contact technique spike pattern errors
A-Scan Biometry - Tough Viva Questions & Answers (Ophthalmology Residency)
SECTION 1: PHYSICS & PRINCIPLES
Distance = Time × Velocity / 2
| Medium | Velocity |
|---|---|
| Cornea + Lens | 1641 m/s |
| Aqueous + Vitreous | 1532 m/s |
| Normal phakic eye (average) | 1550-1555 m/s |
| Aphakic eye | 1532 m/s |
| Pseudophakic eye | 1532 m/s + correction for IOL material |
- Combined probe tip + cornea (initial spike)
- Anterior lens capsule
- Posterior lens capsule
- Retina (steep, perpendicular rise - the most important spike)
- Sclera + orbital fat
- Probe tip
- Cornea (now separate from probe)
- Anterior lens
- Posterior lens
- Retina
- Sclera
SECTION 2: CONTACT vs IMMERSION TECHNIQUE
- Falsely shortened axial length measurement
- Shallower anterior chamber depth on the scan
- Leads to underpowered IOL (residual hyperopia postoperatively)
- Avoids corneal compression - more accurate axial length
- Less technician-dependent (reproducible between operators)
- Faster when proficient
- Preferred in soft eyes (low IOP), where compression artifact is worst
- Gold standard for pediatric biometry under anesthesia
SECTION 3: AXIAL LENGTH & NORMAL VALUES
- Each 1 mm change in axial length changes IOL power by approximately 2.5-3 diopters
- This effect is greater in short eyes than long eyes (inverse relationship with AL)
- Axial length is the single most important variable in IOL power calculation
| Condition | Axial Length |
|---|---|
| Nanophthalmos | < 20 mm |
| Microphthalmos (clinical) | < 21 mm |
| Short eye (prone to error) | < 22 mm |
| Emmetropia | ~24 mm |
| Long eye (myopia prone) | > 26 mm |
| High myopia (staphyloma risk) | > 26-28 mm |
SECTION 4: IOL POWER CALCULATION FORMULAE
- P = IOL power (D)
- A = A-constant (IOL-specific)
- K = Average keratometry (D)
- AL = Axial length (mm)
- First-generation empirical regression formula; least accurate
- Notoriously inaccurate for eyes outside the normal AL range (short or long eyes)
- Should only be used for manual calculations when no software is available
- Superseded by SRK II, then SRK/T
| Eye | Axial Length | Recommended Formulae |
|---|---|---|
| Short | < 22 mm | Hoffer Q, Haigis, Hill-RBF, Kane |
| Average | 22-26 mm | SRK/T, Holladay 1, any 3rd gen |
| Long | > 26 mm | Barrett Universal II, Holladay (with optimized constants), Haigis, Kane |
- IOL design (single-piece vs. 3-piece)
- IOL material (PMMA, acrylic, silicone)
- IOL position (in-the-bag vs. sulcus)
- Surgical technique (incision size, surgeon)
P = a0 + a1 × ACD (measured) + a2 × AL
SECTION 5: SPECIAL SITUATIONS
- Use optical biometry (IOL Master) - not affected by silicone oil
- If using A-scan: use a silicone-oil specific velocity setting
- Apply the Okulix or other silicone oil calculation method
- Correction factor formula: CT × (1 - 1532/vel of silicone)
- Keratometry underestimates corneal power (measures posterior curvature altered)
- Standard index of refraction assumptions are invalid
- ELP prediction errors (formulae assume normal corneal shape)
- Clinical history method: Uses pre-LASIK refraction and K values
- Contact lens method: Fitting of plano contact lens to derive true corneal power
- Haigis-L formula: Uses statistical regression, no historical data needed
- Barrett True K / Masket formula: Adjust for refractive history
- Always warn patient of likely refractive surprise
| IOL Material | Correction (add to aphakic measurement) |
|---|---|
| PMMA | +0.4 mm |
| Acrylic | +0.2 mm |
| Silicone (high-velocity) | -0.4 to -0.8 mm |
- Sound velocity in aphakic eye = 1532 m/s (same as aqueous/vitreous, no lens)
- The two lens spikes are absent
- A single spike appears from the anterior vitreous face / posterior capsule
- Immersion technique is strongly preferred for aphakic eyes
- Biometers must be set to aphakic mode
SECTION 6: ERRORS & QUALITY CONTROL
- Corneal compression (contact method) - underestimates AL
- Misalignment (off visual axis) - underestimates AL
- Incomplete retinal spike (steeply-rising retinal spike is mandatory)
- Beam directed at optic nerve instead of macula
- Poor fixation (dense cataract, nystagmus, macular disease)
- Staphyloma (posterior pole irregularity) - gives variable readings
- Silicone oil in vitreous
- Previous corneal refractive surgery
- Using wrong formula for extreme AL
- Not optimizing A-constants for the surgeon's own outcomes
- Rise steeply at 90 degrees to the baseline
- Be of maximum height
- Be clearly separated from the scleral spike
| Feature | Optical Biometry | A-scan Ultrasound |
|---|---|---|
| Method | Partial coherence interferometry (laser) | Ultrasound pulses |
| Contact | Non-contact | Contact or immersion |
| Accuracy | Higher (gold standard) | Slightly lower |
| Dense cataracts | May fail | Works (sound penetrates) |
| Posterior staphyloma | Handles better | Problematic |
| Silicone oil | Unaffected | Significant error |
| Technician skill needed | Less | More (contact) |
| Also measures | K, ACD, LT, WTW | Mainly AL |
SECTION 7: HIGH-YIELD CLINCHERS
- Repeat with immersion technique (Prager shell + saline bath)
- Measure the fellow eye - bilateral symmetry is expected (within 0.3 mm)
- If white cataract prevents optical biometry, ensure immersion A-scan is used
- Use Hoffer Q or Haigis formula (short eye)
- Target slight myopia (-0.5 D) to avoid aphakia from underpowered IOL
- Obtain pre-LASIK K values and refraction (clinical history method)
- Use Haigis-L or Barrett True K (no historical data needed)
- Target mild myopia (-0.5 to -1.0 D) as a safety buffer
- Warn patient of refractive uncertainty; discuss piggyback IOL option if needed
- A 1 mm error in axial length = ~2.5-3 D error in IOL power
- A 1 D error in keratometry = ~1 D error in IOL power
Create a study guide or flashcard PDF for A-scan viva review
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace not found"
mkdir -p /home/daytona/workspace/ascan-viva && python3 -c "from reportlab.lib.pa…
~/ascan-viva/build_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import mm, cm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.pdfgen import canvas
from reportlab.platypus import BaseDocTemplate, PageTemplate, Frame
OUTPUT = "/home/daytona/workspace/ascan-viva/AScan_Viva_StudyGuide.pdf"
# ── Colour palette ──────────────────────────────────────────────────────────
NAVY = colors.HexColor("#0D2B55")
TEAL = colors.HexColor("#1A7A8C")
GOLD = colors.HexColor("#E8A020")
LIGHT_BLUE = colors.HexColor("#D6EAF8")
LIGHT_TEAL = colors.HexColor("#D0EDE9")
LIGHT_GOLD = colors.HexColor("#FEF3DC")
WHITE = colors.white
DARK_GREY = colors.HexColor("#333333")
MID_GREY = colors.HexColor("#666666")
LIGHT_GREY = colors.HexColor("#F5F5F5")
RED_HL = colors.HexColor("#C0392B")
GREEN_HL = colors.HexColor("#1E8449")
W, H = A4
# ── Styles ───────────────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
def S(name, **kw):
return ParagraphStyle(name, **kw)
cover_title = S("CoverTitle",
fontSize=32, fontName="Helvetica-Bold", textColor=WHITE,
alignment=TA_CENTER, leading=40, spaceAfter=8)
cover_sub = S("CoverSub",
fontSize=16, fontName="Helvetica", textColor=LIGHT_BLUE,
alignment=TA_CENTER, leading=22, spaceAfter=4)
cover_badge = S("CoverBadge",
fontSize=12, fontName="Helvetica-Bold", textColor=GOLD,
alignment=TA_CENTER, leading=18)
sec_header = S("SecHeader",
fontSize=14, fontName="Helvetica-Bold", textColor=WHITE,
alignment=TA_LEFT, leading=18, spaceBefore=4, spaceAfter=4)
q_style = S("Question",
fontSize=11, fontName="Helvetica-Bold", textColor=NAVY,
alignment=TA_LEFT, leading=15, spaceBefore=6, spaceAfter=3)
a_style = S("Answer",
fontSize=10, fontName="Helvetica", textColor=DARK_GREY,
alignment=TA_JUSTIFY, leading=14, spaceAfter=4,
leftIndent=12)
bullet_style = S("Bullet",
fontSize=10, fontName="Helvetica", textColor=DARK_GREY,
alignment=TA_LEFT, leading=14, leftIndent=20, spaceAfter=2,
bulletIndent=8)
highlight_style = S("Highlight",
fontSize=10, fontName="Helvetica-Bold", textColor=RED_HL,
alignment=TA_LEFT, leading=14, leftIndent=12, spaceAfter=3)
mnemo_style = S("Mnemo",
fontSize=10, fontName="Helvetica-Oblique", textColor=GREEN_HL,
alignment=TA_LEFT, leading=14, leftIndent=12, spaceAfter=3)
table_hdr = S("TableHdr",
fontSize=9, fontName="Helvetica-Bold", textColor=WHITE,
alignment=TA_CENTER, leading=12)
table_cell = S("TableCell",
fontSize=9, fontName="Helvetica", textColor=DARK_GREY,
alignment=TA_LEFT, leading=12)
table_cell_c = S("TableCellC",
fontSize=9, fontName="Helvetica", textColor=DARK_GREY,
alignment=TA_CENTER, leading=12)
note_style = S("Note",
fontSize=9, fontName="Helvetica-Oblique", textColor=MID_GREY,
alignment=TA_LEFT, leading=13, leftIndent=12)
def P(text, style=a_style): return Paragraph(text, style)
def Q(text): return Paragraph(f"Q: {text}", q_style)
def A(text): return Paragraph(text, a_style)
def B(text): return Paragraph(f"• {text}", bullet_style)
def HL(text): return Paragraph(f"⚠ {text}", highlight_style)
def MN(text): return Paragraph(f"💡 {text}", mnemo_style)
def SP(h=4): return Spacer(1, h*mm)
def HR(): return HRFlowable(width="100%", thickness=0.5, color=colors.HexColor("#CCCCCC"), spaceAfter=3)
def section_banner(title, color=NAVY):
tbl = Table([[Paragraph(title, sec_header)]], colWidths=[W - 2*cm])
tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), color),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
("ROUNDEDCORNERS", [4,4,4,4]),
]))
return tbl
def qa_box(question, answer_elements, bg=LIGHT_TEAL):
"""Wraps a Q+A block in a coloured box."""
inner = [P(f"<b>Q: {question}</b>", q_style)] + answer_elements
tbl = Table([[inner]], colWidths=[W - 2*cm])
tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("BOX", (0,0), (-1,-1), 0.5, TEAL),
("ROUNDEDCORNERS", [4,4,4,4]),
]))
return tbl
def make_table(headers, rows, col_widths=None):
data = [[Paragraph(h, table_hdr) for h in headers]]
for row in rows:
data.append([Paragraph(str(c), table_cell_c) for c in row])
if not col_widths:
col_widths = [(W - 2*cm) / len(headers)] * len(headers)
tbl = Table(data, colWidths=col_widths)
style = [
("BACKGROUND", (0,0), (-1,0), NAVY),
("ROWBACKGROUNDS", (0,1), (-1,-1), [WHITE, LIGHT_GREY]),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#BBBBBB")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
]
tbl.setStyle(TableStyle(style))
return tbl
# ── Page decorators ──────────────────────────────────────────────────────────
def draw_cover(c, doc):
c.saveState()
# Navy background
c.setFillColor(NAVY)
c.rect(0, 0, W, H, fill=1, stroke=0)
# Gold accent bar top
c.setFillColor(GOLD)
c.rect(0, H - 16*mm, W, 16*mm, fill=1, stroke=0)
# Teal accent bar bottom
c.setFillColor(TEAL)
c.rect(0, 0, W, 12*mm, fill=1, stroke=0)
# Decorative circles
c.setFillColor(colors.HexColor("#163A6E"))
c.circle(W - 50, H - 80, 110, fill=1, stroke=0)
c.circle(40, 100, 70, fill=1, stroke=0)
c.restoreState()
def draw_page(c, doc):
c.saveState()
# Top stripe
c.setFillColor(NAVY)
c.rect(0, H - 12*mm, W, 12*mm, fill=1, stroke=0)
# Bottom stripe
c.setFillColor(TEAL)
c.rect(0, 0, W, 8*mm, fill=1, stroke=0)
# Page number
c.setFillColor(WHITE)
c.setFont("Helvetica", 8)
c.drawCentredString(W/2, 2.5*mm, f"A-Scan Biometry Viva Guide | Page {doc.page}")
# Header text
c.setFont("Helvetica-Bold", 8)
c.setFillColor(GOLD)
c.drawString(1*cm, H - 8.5*mm, "A-SCAN BIOMETRY")
c.setFillColor(WHITE)
c.setFont("Helvetica", 8)
c.drawRightString(W - 1*cm, H - 8.5*mm, "Ophthalmology Residency Viva")
c.restoreState()
# ── Build document ────────────────────────────────────────────────────────────
doc = BaseDocTemplate(OUTPUT, pagesize=A4,
leftMargin=1*cm, rightMargin=1*cm,
topMargin=1.5*cm, bottomMargin=1.5*cm)
cover_frame = Frame(0, 0, W, H, id="cover", leftPadding=0, rightPadding=0,
topPadding=0, bottomPadding=0)
body_frame = Frame(1*cm, 1.5*cm, W - 2*cm, H - 3*cm, id="body")
cover_template = PageTemplate(id="Cover", frames=[cover_frame], onPage=draw_cover)
body_template = PageTemplate(id="Body", frames=[body_frame], onPage=draw_page)
doc.addPageTemplates([cover_template, body_template])
story = []
# ═══════════════════════════════════════════════════════════════════════════════
# COVER PAGE
# ═══════════════════════════════════════════════════════════════════════════════
story.append(Spacer(1, 55*mm))
story.append(Paragraph("A-SCAN BIOMETRY", cover_title))
story.append(Spacer(1, 4*mm))
story.append(Paragraph("Viva Study Guide", cover_sub))
story.append(Spacer(1, 8*mm))
story.append(Paragraph("Ophthalmology Residency Exam Preparation", cover_badge))
story.append(Spacer(1, 14*mm))
# Quick-reference box on cover
cover_qr_data = [
[Paragraph("KEY NUMBERS TO REMEMBER", ParagraphStyle("ch", fontSize=10, fontName="Helvetica-Bold", textColor=NAVY, alignment=TA_CENTER))],
[Paragraph(
"Normal AL: <b>24 mm</b> | Phakic velocity: <b>1555 m/s</b> | Aphakic velocity: <b>1532 m/s</b><br/>"
"AL error impact: <b>2.5–3 D / mm</b> | K error impact: <b>1 D / D</b><br/>"
"Contact spikes: <b>5</b> | Immersion spikes: <b>6</b> | Sulcus ACD reduction: <b>0.25 mm</b>",
ParagraphStyle("cv", fontSize=10, fontName="Helvetica", textColor=DARK_GREY,
alignment=TA_CENTER, leading=17))],
]
cover_tbl = Table(cover_qr_data, colWidths=[14*cm])
cover_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), GOLD),
("BACKGROUND", (0,1), (-1,1), WHITE),
("BOX", (0,0), (-1,-1), 1.5, GOLD),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 12),
("RIGHTPADDING", (0,0), (-1,-1), 12),
("ROUNDEDCORNERS", [6,6,6,6]),
]))
story.append(cover_tbl)
story.append(Spacer(1, 18*mm))
story.append(Paragraph("28 High-Yield Questions | 7 Topics | Clinical Pearls", cover_sub))
# Switch to body template
from reportlab.platypus import NextPageTemplate
story.append(NextPageTemplate("Body"))
story.append(PageBreak())
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 1: PHYSICS & PRINCIPLES
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_banner("SECTION 1 — Physics & Principles", NAVY))
story.append(SP(4))
# Q1
story.append(KeepTogether([
Q("What is the fundamental principle of A-scan ultrasonography?"),
A("A-scan uses <b>10 MHz</b> high-frequency sound waves. The probe emits a pulse that "
"reflects off each acoustic interface in the eye (cornea, anterior lens, posterior lens, retina). "
"Time-of-flight is converted to distance:"),
A("<b>Distance = Time × Velocity / 2</b>"),
A("Result is a 1-D amplitude display — reflecting surfaces appear as vertical spikes. "
"'A' = <i>Amplitude</i> modulation."),
SP(3),
]))
# Q2 - Velocity table
story.append(KeepTogether([
Q("What are the standard sound velocities used in A-scan biometry?"),
SP(2),
make_table(
["Medium", "Velocity (m/s)"],
[
["Cornea + Crystalline lens", "1641"],
["Aqueous humour + Vitreous", "1532"],
["Normal phakic eye (average)", "1555"],
["Aphakic eye", "1532"],
["Pseudophakic eye", "1532 + IOL correction"],
],
col_widths=[10*cm, 5.5*cm]
),
SP(2),
MN("Memory: 1641 (solid structures) → 1555 (phakic average) → 1532 (fluid/aphakic)"),
SP(3),
]))
# Q3
story.append(KeepTogether([
Q("Why does sound travel faster through the lens than vitreous?"),
A("The crystalline lens is a denser, more solid structure. Acoustic velocity increases "
"with the elasticity-to-density ratio of a medium. Greater molecular density and structural "
"rigidity → faster sound propagation. Aqueous and vitreous are watery liquids — lower density."),
SP(3),
]))
# Q4 - spike pattern
story.append(KeepTogether([
Q("Describe the A-scan spike pattern in a normal phakic eye (contact method)."),
A("<b>5 spikes</b> in the contact technique:"),
B("1. Probe tip + Cornea (combined — single spike)"),
B("2. Anterior lens capsule"),
B("3. Posterior lens capsule"),
B("4. Retina (steep 90° rise — most critical)"),
B("5. Sclera / Orbital fat"),
A("Ideal scan: all spikes at maximum amplitude, retinal spike steeply rising and "
"clearly separated from scleral spike."),
SP(3),
]))
# Q5 - immersion
story.append(KeepTogether([
Q("How does the immersion technique differ from contact in terms of spike count?"),
A("Immersion produces <b>6 spikes</b> because the probe does not touch the cornea — "
"probe tip and cornea are now separate acoustic interfaces:"),
B("1. Probe tip (in saline)"),
B("2. Cornea (separate spike)"),
B("3. Anterior lens"),
B("4. Posterior lens"),
B("5. Retina"),
B("6. Sclera"),
MN("Contact = 5 spikes. Immersion = 6 spikes. Extra spike = separate cornea."),
SP(3),
]))
story.append(PageBreak())
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 2: CONTACT vs IMMERSION
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_banner("SECTION 2 — Contact vs Immersion Technique", TEAL))
story.append(SP(4))
story.append(KeepTogether([
Q("What is the most common and most important error in contact A-scan biometry?"),
A("<b>Corneal compression (applanation artifact)</b>. Even minimal probe pressure "
"indents the soft cornea, causing:"),
B("Falsely <b>shortened</b> axial length"),
B("Shallower ACD on scan"),
B("Leads to underpowered IOL → residual <b>hyperopia</b> postoperatively"),
HL("Rule: Delete readings with unexpectedly shallow ACD even if spikes look good."),
SP(3),
]))
story.append(KeepTogether([
Q("By how much does immersion A-scan differ from contact A-scan for axial length?"),
A("Immersion eyes measure <b>0.1–0.3 mm longer</b> than contact eyes. This is NOT an "
"overestimation — it is the accurate value. Contact underestimates due to corneal indentation."),
SP(3),
]))
story.append(KeepTogether([
Q("What is the Prager shell and what does it do?"),
A("A small scleral cup placed between the lids over the anesthetized eye, filled with saline. "
"The A-scan probe is immersed in the fluid bath — avoids any corneal contact, eliminating "
"compression artifact. Enables the immersion technique of biometry."),
SP(3),
]))
# Comparison table
story.append(KeepTogether([
Q("Compare contact vs immersion A-scan vs optical biometry."),
SP(2),
make_table(
["Feature", "Contact A-scan", "Immersion A-scan", "Optical Biometry"],
[
["Corneal contact", "Yes", "No", "No"],
["Main error", "Compression", "None significant", "Dense cataract block"],
["Spikes", "5", "6", "N/A (laser)"],
["Technician skill", "High", "Moderate", "Low"],
["Accuracy", "Lowest", "Good", "Best"],
["Dense cataract", "Works", "Works", "May fail"],
["Silicone oil", "Error", "Error", "Unaffected"],
],
col_widths=[4.5*cm, 4*cm, 4*cm, 3.5*cm]
),
SP(3),
]))
story.append(KeepTogether([
Q("List advantages of immersion over contact A-scan."),
B("Avoids corneal compression → more accurate axial length"),
B("Less technician-dependent, reproducible between operators"),
B("Faster when proficient"),
B("Preferred in soft eyes (low IOP) where compression is worst"),
B("Gold standard for paediatric biometry under anaesthesia"),
SP(3),
]))
story.append(PageBreak())
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 3: AXIAL LENGTH
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_banner("SECTION 3 — Axial Length & Normal Values", NAVY))
story.append(SP(4))
story.append(KeepTogether([
Q("What is the average axial length of a normal adult phakic eye?"),
A("Average: <b>24 mm</b> (range ~22–26 mm in emmetropia)."),
A("Clinical significance: <b>Each 1 mm change in AL = ~2.5–3 D change in IOL power</b>. "
"Effect is greater in short eyes than long eyes. AL is the single most important variable "
"in IOL power calculation."),
SP(3),
]))
story.append(KeepTogether([
Q("What axial lengths define microphthalmos and high myopia?"),
SP(2),
make_table(
["Condition", "Axial Length"],
[
["Nanophthalmos", "< 20 mm"],
["Microphthalmos (clinical)", "< 21 mm"],
["Short eye (formula caution)", "< 22 mm"],
["Emmetropia", "~24 mm"],
["Long eye (myopia prone)", "> 26 mm"],
["High myopia / staphyloma risk", "> 26–28 mm"],
],
col_widths=[10*cm, 5.5*cm]
),
SP(3),
]))
story.append(KeepTogether([
Q("From where to where is axial length measured?"),
A("From the <b>anterior corneal epithelial surface</b> to the "
"<b>retinal pigment epithelium (RPE) at the macula (fovea)</b>. "
"Alignment must be along the <b>visual axis</b>, not the optic nerve axis. "
"Beam hitting the optic nerve → absent scleral spike (recognisable error pattern)."),
SP(3),
]))
story.append(PageBreak())
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 4: IOL POWER CALCULATION FORMULAE
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_banner("SECTION 4 — IOL Power Calculation Formulae", TEAL))
story.append(SP(4))
story.append(KeepTogether([
Q("Write the basic SRK formula. State its limitations."),
A("<b>P = A − 0.9K − 2.5(AL)</b>"),
A("Where: P = IOL power (D), A = A-constant, K = average keratometry (D), AL = axial length (mm)"),
A("<b>Limitations:</b>"),
B("1st-generation empirical regression formula — least accurate"),
B("Inaccurate for extreme axial lengths (short/long eyes)"),
B("Superseded by SRK II → SRK/T"),
B("Use only for manual calculation when no software is available"),
SP(3),
]))
story.append(KeepTogether([
Q("Which IOL formula to use for short vs long eyes?"),
SP(2),
make_table(
["Eye Type", "Axial Length", "Recommended Formulae"],
[
["Short", "< 22 mm", "Hoffer Q, Haigis, Hill-RBF, Kane"],
["Average", "22–26 mm", "SRK/T, Holladay 1, Haigis, any 3rd gen"],
["Long", "> 26 mm", "Barrett Universal II, Holladay, Haigis (optimised), Kane"],
],
col_widths=[3.5*cm, 4*cm, 8*cm]
),
SP(2),
HL("Short eyes are MOST prone to unexpected mean spherical error after surgery."),
SP(3),
]))
story.append(KeepTogether([
Q("What is ELP and why is it the most critical variable in modern formulae?"),
A("<b>Effective Lens Position (ELP)</b> = predicted distance from the anterior corneal surface "
"to the principal plane of the implanted IOL."),
A("All formulae try to optimize ELP prediction:"),
B("3rd gen (SRK/T, Holladay 1, Hoffer Q): predict ELP from K + AL"),
B("4th gen (Haigis, Holladay 2): add ACD, lens thickness, white-to-white"),
B("5th gen (Barrett, Kane): AI/regression-enhanced ELP prediction"),
SP(3),
]))
story.append(KeepTogether([
Q("What makes the Haigis formula unique?"),
A("<b>Three IOL constants (a0, a1, a2)</b> instead of a single A-constant:"),
A("<b>P = a0 + a1 × ACD (measured) + a2 × AL</b>"),
A("Separates contribution of ACD from AL → superior for abnormal eyes. "
"Allows personalised optimisation per surgeon per IOL."),
SP(3),
]))
story.append(KeepTogether([
Q("What is the A-constant? What factors affect it?"),
A("IOL-specific empirical constant representing predicted IOL position (ELP). "
"Provided by the manufacturer."),
A("<b>Factors affecting it:</b>"),
B("IOL design (single-piece vs 3-piece)"),
B("IOL material (PMMA / acrylic / silicone)"),
B("IOL position: sulcus → reduce ACD by <b>0.25 mm</b>; posterior iris fixation → further 0.25 mm"),
B("Surgeon's own technique — should personalise using ≥ 20–50 own cases"),
SP(3),
]))
story.append(KeepTogether([
Q("How does a keratometry error compare to an axial length error in terms of IOL impact?"),
SP(2),
make_table(
["Error Source", "Magnitude", "IOL Power Impact"],
[
["Axial Length error", "1 mm", "2.5–3 D"],
["Keratometry error", "1 D", "~1 D"],
],
col_widths=[5*cm, 4*cm, 6.5*cm]
),
SP(2),
HL("Axial length error has 2.5–3× greater impact than keratometry error — most consequential mistake."),
SP(3),
]))
story.append(PageBreak())
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 5: SPECIAL SITUATIONS
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_banner("SECTION 5 — Special Situations", NAVY))
story.append(SP(4))
story.append(KeepTogether([
Q("How do you perform biometry in silicone oil-filled eyes?"),
A("Silicone oil velocity (~980–1040 m/s) is far lower than normal vitreous (1532 m/s). "
"A-scan significantly <b>overestimates</b> axial length (falsely long)."),
A("<b>Solutions:</b>"),
B("Use optical biometry (IOL Master) — unaffected by silicone oil"),
B("A-scan: use silicone oil-specific velocity setting"),
B("Apply Okulix calculation or correction: <b>CF = CT × (1 − 1532/vel)</b>"),
HL("Silicone oil = use optical biometry as first choice."),
SP(3),
]))
story.append(KeepTogether([
Q("What are the pseudophakic A-scan correction factors for different IOL materials?"),
A("Use aphakic mode (1532 m/s), then <b>add correction</b>:"),
SP(2),
make_table(
["IOL Material", "Correction to Add"],
[
["PMMA", "+0.4 mm"],
["Acrylic", "+0.2 mm"],
["Silicone (high velocity)", "−0.4 to −0.8 mm"],
],
col_widths=[8*cm, 7.5*cm]
),
SP(2),
A("Formula: <b>CF = CT × (1 − 1532 / velocity of material)</b>"),
SP(3),
]))
story.append(KeepTogether([
Q("How does aphakia affect A-scan biometry?"),
B("Sound velocity = <b>1532 m/s</b> (no lens, all fluid)"),
B("Two lens spikes are <b>absent</b>; single spike from anterior vitreous face / posterior capsule"),
B("Biometer must be set to <b>aphakic mode</b>"),
B("Immersion technique strongly preferred"),
SP(3),
]))
story.append(KeepTogether([
Q("How do you manage biometry after previous LASIK/PRK?"),
A("Standard IOL formulas FAIL because:"),
B("Keratometry underestimates corneal power (altered index of refraction assumptions)"),
B("ELP prediction errors (formulae assume normal corneal shape)"),
A("<b>Approaches:</b>"),
B("Clinical history method: pre-LASIK refraction + K values"),
B("Contact lens method: plano lens to derive true corneal power"),
B("Haigis-L formula: statistical regression, no historical data needed"),
B("Barrett True K / Masket formula"),
HL("Always target mild myopia (−0.5 to −1.0 D) as safety buffer. Warn patient of refractive surprise."),
SP(3),
]))
story.append(KeepTogether([
Q("A contact lens wearer needs biometry. What precaution is required?"),
B("Soft contact lenses: withhold for <b>≥ 1 week</b> before biometry"),
B("Rigid gas permeable (RGP) lenses: longer period needed — corneal re-stabilisation"),
B("Purpose: allow corneal curvature to return to natural state to avoid false K readings"),
SP(3),
]))
story.append(PageBreak())
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 6: ERRORS & QUALITY CONTROL
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_banner("SECTION 6 — Errors & Quality Control", TEAL))
story.append(SP(4))
story.append(KeepTogether([
Q("List the sources of error in A-scan biometry."),
A("<b>Technical errors:</b>"),
B("Corneal compression (contact) → underestimates AL → hyperopic surprise"),
B("Misalignment (off visual axis) → underestimates AL"),
B("Sloped retinal spike (beam not perpendicular to macula)"),
B("Beam directed at optic nerve instead of macula → absent scleral spike"),
A("<b>Patient factors:</b>"),
B("Poor fixation — dense cataract, nystagmus, macular disease"),
B("Posterior staphyloma — variable readings from same eye"),
B("Silicone oil in vitreous"),
B("Previous corneal refractive surgery"),
A("<b>Formula selection errors:</b>"),
B("Wrong formula for extreme AL"),
B("Unoptimised A-constants"),
SP(3),
]))
story.append(KeepTogether([
Q("What does the ideal retinal spike look like and why does it matter?"),
A("The ideal retinal spike must:"),
B("Rise <b>steeply at 90°</b> to the baseline"),
B("Be at <b>maximum height</b>"),
B("Be <b>clearly separated</b> from the scleral spike"),
HL("A sloped retinal spike = off-axis measurement. That reading MUST be rejected — "
"it represents a longer-than-true path through the vitreous."),
SP(3),
]))
story.append(KeepTogether([
Q("What is posterior staphyloma and why is it problematic for biometry?"),
A("Posterior staphyloma is an outpouching of the posterior sclera seen in high myopia. "
"The macula may be at the bottom of the staphyloma, resulting in:"),
B("Multiple different axial length readings from the same eye"),
B("Difficulty identifying the true macular point"),
B("Optical biometry (IOL Master) is preferred as it targets the RPE directly"),
B("A-scan: use the reading corresponding to the longest reproducible measurement"),
SP(3),
]))
story.append(PageBreak())
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 7: CLINICAL VIVA SCENARIOS
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_banner("SECTION 7 — Clinical Viva Scenarios", NAVY))
story.append(SP(4))
story.append(KeepTogether([
Q("A dense white cataract — contact A-scan gives AL = 21.8 mm. What do you do?"),
HL("Red flags: dense cataract (poor fixation), very short AL, contact method used."),
A("<b>Steps:</b>"),
B("1. Repeat with <b>immersion technique</b> (Prager shell + saline bath)"),
B("2. Measure fellow eye — bilateral AL should be within 0.3 mm"),
B("3. Select formula for short eye: <b>Hoffer Q or Haigis</b>"),
B("4. Target slight myopia (−0.5 D) to avoid aphakia from underpowered IOL"),
B("5. If optical biometry was tried but failed: A-scan immersion is the gold standard backup"),
SP(3),
]))
story.append(KeepTogether([
Q("IOL Master K readings post-LASIK show 36.5 D. What is the concern?"),
HL("Post-myopic LASIK: central ablation makes cornea flatter → IOL Master "
"underestimates true corneal power using standard index (1.3375)."),
A("<b>Approach:</b>"),
B("Use Haigis-L or Barrett True K (no pre-LASIK data needed)"),
B("If historical data available: clinical history method"),
B("Target −0.5 to −1.0 D as safety buffer"),
B("Counsel patient: higher risk of refractive surprise, possible piggyback IOL later"),
SP(3),
]))
story.append(KeepTogether([
Q("Why does optical biometry (IOL Master) fail in some cases and what is the backup?"),
A("Optical biometry (partial coherence interferometry) uses laser — blocked by:"),
B("Very dense posterior subcapsular cataracts"),
B("Dense nuclear or cortical opacities where the signal cannot penetrate"),
B("Corneal scarring / opacification"),
A("<b>Backup:</b> Immersion A-scan ultrasonography — sound penetrates opaque media."),
SP(3),
]))
story.append(KeepTogether([
Q("A patient reports −6.0 D residual hyperopia after cataract surgery. "
"What went wrong and how?"),
A("Most likely cause: <b>corneal compression during contact A-scan biometry</b>. "
"Compressed cornea → falsely short AL → IOL power calculated too low → "
"insufficient refractive power implanted → hyperopic outcome."),
A("Other possibilities: formula error for short eye, wrong A-constant, wrong IOL implanted."),
B("Prevention: immersion A-scan or optical biometry; check fellow eye symmetry"),
B("Management: spectacles, contact lens, IOL exchange, piggyback IOL, or LASIK correction"),
SP(3),
]))
# ═══════════════════════════════════════════════════════════════════════════════
# QUICK REFERENCE FLASHCARD TABLE
# ═══════════════════════════════════════════════════════════════════════════════
story.append(PageBreak())
story.append(section_banner("QUICK REFERENCE — High-Yield Numbers & Facts", GOLD))
story.append(SP(4))
qr_data = [
[Paragraph("<b>Parameter</b>", table_hdr), Paragraph("<b>Value / Fact</b>", table_hdr)],
[P("Normal adult axial length", table_cell), P("<b>24 mm</b>", table_cell)],
[P("AL impact on IOL power", table_cell), P("<b>2.5–3 D per mm</b>", table_cell)],
[P("K impact on IOL power", table_cell), P("<b>~1 D per 1 D</b>", table_cell)],
[P("Sound velocity — phakic eye", table_cell), P("<b>1555 m/s</b>", table_cell)],
[P("Sound velocity — aphakic eye", table_cell), P("<b>1532 m/s</b>", table_cell)],
[P("Sound velocity — cornea + lens", table_cell), P("<b>1641 m/s</b>", table_cell)],
[P("Contact A-scan spikes", table_cell), P("<b>5 spikes</b>", table_cell)],
[P("Immersion A-scan spikes", table_cell), P("<b>6 spikes</b> (cornea + probe separate)", table_cell)],
[P("Immersion vs contact AL difference", table_cell), P("<b>0.1–0.3 mm longer</b> on immersion (no compression)", table_cell)],
[P("Sulcus ACD reduction", table_cell), P("<b>−0.25 mm</b> from in-bag value", table_cell)],
[P("PMMA pseudophakic correction", table_cell), P("<b>+0.4 mm</b> from aphakic mode", table_cell)],
[P("Acrylic IOL correction", table_cell), P("<b>+0.2 mm</b> from aphakic mode", table_cell)],
[P("Silicone IOL correction", table_cell), P("<b>−0.4 to −0.8 mm</b> from aphakic mode", table_cell)],
[P("Short eye formula choice (AL < 22 mm)", table_cell), P("<b>Hoffer Q, Haigis, Hill-RBF, Kane</b>", table_cell)],
[P("Long eye formula choice (AL > 26 mm)", table_cell), P("<b>Barrett Universal II, Holladay, Haigis, Kane</b>", table_cell)],
[P("Nanophthalmos", table_cell), P("<b>AL < 20 mm</b>", table_cell)],
[P("A-constant unique to", table_cell), P("IOL design, material, position, surgeon technique", table_cell)],
[P("Haigis formula constants", table_cell), P("<b>3 constants: a0, a1, a2</b>", table_cell)],
[P("Soft CL: withhold before biometry", table_cell), P("<b>≥ 1 week</b>", table_cell)],
]
qr_tbl = Table(qr_data, colWidths=[8*cm, 7.5*cm])
qr_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("ROWBACKGROUNDS", (0,1), (-1,-1), [WHITE, LIGHT_GOLD]),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#CCCCCC")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 7),
("RIGHTPADDING", (0,0), (-1,-1), 7),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
]))
story.append(qr_tbl)
story.append(SP(5))
story.append(P("Good luck in your viva! Review the high-yield numbers daily in the week before your exam.", note_style))
# ── Build ─────────────────────────────────────────────────────────────────────
doc.build(story)
print("PDF built successfully:", OUTPUT)
cd /home/daytona/workspace/ascan-viva && python3 build_pdf.py 2>&1
ls -lh /home/daytona/workspace/ascan-viva/AScan_Viva_StudyGuide.pdf
AScan Viva StudyGuide
PDF Document · PDF
| Section | Content |
|---|---|
| Cover page | Key numbers at a glance (navy/gold design) |
| Section 1 | Physics & Principles — 5 Q&As with velocity table |
| Section 2 | Contact vs Immersion — comparison table, Prager shell, 5 vs 6 spikes |
| Section 3 | Axial Length & Normal Values — AL ranges table |
| Section 4 | IOL Power Formulae — SRK, ELP, Haigis, formula selection by AL |
| Section 5 | Special Situations — silicone oil, pseudophakic corrections, post-LASIK, aphakia |
| Section 6 | Errors & Quality Control — retinal spike criteria, staphyloma |
| Section 7 | Clinical Viva Scenarios — 4 case-based questions |
| Quick Ref | Full high-yield numbers table (gold header) |
Panopthalmitis case presentation for ophthalmology residency
panophthalmitis case presentation clinical features management ophthalmology residency
https://eyewiki.org/Panophthalmitis
PANOPHTHALMITIS — Complete Case Presentation
Ophthalmology Residency Grand Rounds
DEFINITION & ANATOMICAL EXTENT
| Term | Extent of Inflammation |
|---|---|
| Endophthalmitis | Vitreous cavity ± anterior segment |
| Panophthalmitis | All above + uvea + sclera + Tenon's capsule + orbit |
CASE PRESENTATION
HISTORY OF PRESENT ILLNESS
- Onset: Sudden onset of severe, throbbing right eye pain 5 days ago
- Preceding event: Sustaining a penetrating injury to the right eye with a wooden twig 6 days prior while working in a field; patient initially ignored the injury
- Progression: Progressive redness, profuse mucopurulent discharge, swelling of eyelids, and complete loss of vision over 72 hours
- Systemic symptoms: Fever (38.9°C), malaise, severe headache
- Marked lid swelling and inability to open the eye
- Purulent yellow-green discharge
- Photophobia (prior to complete loss of light perception)
- Nausea and vomiting (from severe pain)
- Proptosis noted by family members
PAST HISTORY
- No prior ocular surgery or trauma
- No systemic illness (diabetes, hypertension, immunosuppression)
- No intravenous drug use
- Tetanus vaccination status: unknown
EXAMINATION
External Examination - Right Eye:
| Finding | Description |
|---|---|
| Eyelids | Marked oedema, hyperaemia, warm to touch |
| Conjunctiva | Intense chemosis, 360° ciliary + conjunctival congestion |
| Discharge | Profuse mucopurulent/purulent |
| Proptosis | ~4 mm by Hertel exophthalmometry |
| Ocular motility | Severely restricted in all directions; painful on attempted movement |
| Cornea | Oedematous, cloudy, yellowish infiltration; impending perforation centrally |
Slit-Lamp Examination - Right Eye:
| Structure | Finding |
|---|---|
| Cornea | Dense oedema, stromal infiltration, Descemet's folds |
| Anterior chamber | Hypopyon (2 mm level), intense flare |
| Iris | Congested, muddy, posterior synechiae |
| Pupil | Mid-dilated, sluggish, irregular |
| Lens | Hazy view |
| Fundus | No red reflex; no fundal view |
Left Eye: Completely normal
- Right eye: No light perception (NLP)
- Left eye: 6/6
INVESTIGATIONS
Ocular Investigations:
- Dense vitreous echoes (vitritis)
- Choroidal thickening
- Scleral thickening with subtenon fluid (T-sign / thickened posterior coats)
- No retinal detachment identified
- Vitreous aspiration performed
- Gram stain: Gram-positive bacilli (preliminary)
- Culture sent (blood agar, chocolate agar, Sabouraud's)
Systemic Investigations:
| Investigation | Result |
|---|---|
| CBC | WBC 18,400/μL (neutrophilia) |
| CRP | 86 mg/L (elevated) |
| ESR | 68 mm/hr |
| Blood cultures (×2 sets) | Pending |
| Blood glucose (random) | 89 mg/dL |
| Chest X-ray | No focal consolidation |
| ECG | Normal sinus rhythm |
| CT orbit (axial + coronal, with contrast) | Right globe: diffuse scleral thickening, subtenon enhancement, periorbital fat stranding; no subperiosteal abscess; no intracranial extension |
PATHOLOGICAL IMAGE
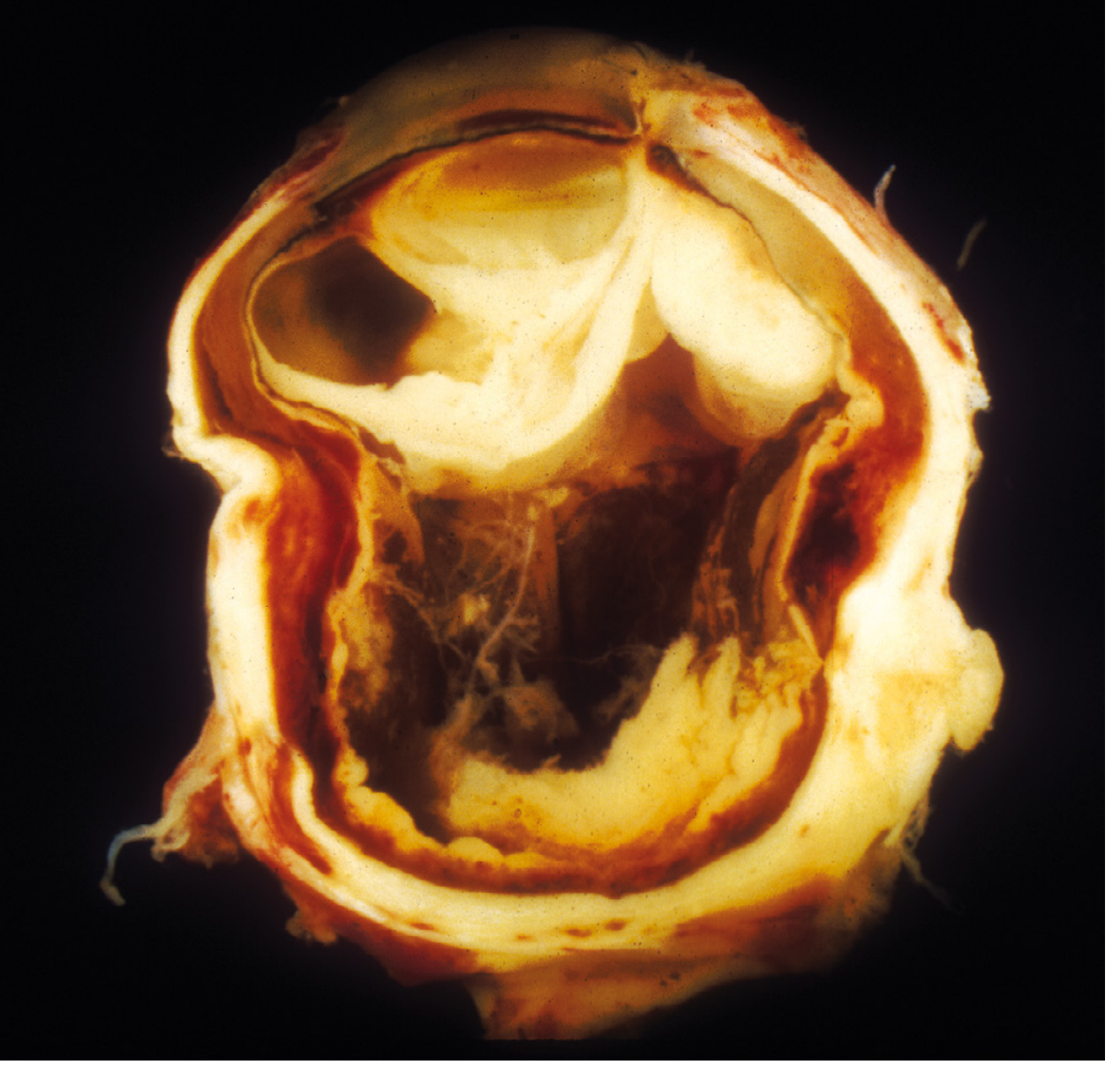
DIAGNOSIS
AETIOLOGY & CLASSIFICATION
Classification by Route of Infection:
1. Exogenous (most common)
- Penetrating ocular injuries (especially organic matter: wood, vegetable matter, soil)
- Perforating corneal ulcer
- Post-operative infection following intraocular surgery
- Infected corneal ulcer with scleral spread
- Secondary from orbital cellulitis
2. Endogenous (haematogenous spread)
- Septicaemia (any source)
- Infective endocarditis
- IV drug abuse (Bacillus cereus is classic)
- Klebsiella liver abscess (especially East/Southeast Asia - Klebsiella pneumoniae endogenous endophthalmitis-panophthalmitis)
- Dental abscess / puerperal sepsis (less common)
- Meningococcaemia
Causative Organisms:
Bacterial (most common overall):
| Category | Organisms |
|---|---|
| Gram-positive cocci (most common post-surgical) | S. epidermidis, S. aureus, Streptococcus spp. |
| Post-traumatic (especially organic FB) | Bacillus cereus, Bacillus anthracis |
| Endogenous sepsis | S. aureus, Streptococci, Klebsiella, Neisseria meningitidis, H. influenzae |
| IV drug users | Bacillus cereus (classic association) |
| Post-cataract surgery | S. epidermidis, S. aureus, Pseudomonas |
| Anaerobes | Propionibacterium acnes (delayed post-op), Clostridium |
Fungal:
- Aspergillus (post-traumatic, especially agricultural soil)
- Rhizopus / Mucor (immunocompromised, diabetics)
- Candida (endogenous, IV drug users, immunosuppressed)
- Fusarium
Viral (rare panophthalmitis):
- Herpes simplex virus (HSV)
- Varicella-zoster virus (VZV)
- Dengue virus
DIFFERENTIAL DIAGNOSIS
| Condition | Key Differentiating Features |
|---|---|
| Endophthalmitis (without orbital extension) | No proptosis, no restricted EOM, no Tenon's involvement on imaging |
| Orbital cellulitis | No hypopyon, anterior segment usually normal, no fundal involvement |
| Acute angle-closure glaucoma | Corneal haze but no discharge, no hypopyon, IOP very elevated |
| Perforated corneal ulcer with iris prolapse | Flat AC, prolapsed iris plug, no orbital signs |
| Acute dacryocystitis with orbital spread | Medial canthal swelling, nasolacrimal system origin |
| Retinoblastoma with secondary inflammation | Child, leukocoria history, imaging shows mass |
| Sympathetic ophthalmia | History of trauma to fellow eye, bilateral granulomatous uveitis |
MANAGEMENT
Principles:
- Multidisciplinary approach - Ophthalmology + Infectious Disease + Internal Medicine
- Immediate hospitalisation
- Maximise globe salvage attempts before proceeding to destructive surgery
- Systemic cultures before initiating antibiotics
Step-by-Step Management:
STEP 1 — Cultures First (Before Any Antibiotic)
- Vitreous tap ± anterior chamber tap
- Blood cultures (×2 sets, different sites)
- Culture of any discharge (Gram stain, KOH, culture)
- Urine culture if endogenous source suspected
- Consider transesophageal echocardiogram (rule out endocarditis)
STEP 2 — Empiric Intravitreal Antibiotics (Tap & Inject)
| Drug | Dose (intravitreal) |
|---|---|
| Vancomycin (Gram-positive cover) | 1 mg in 0.1 mL |
| Ceftazidime (Gram-negative cover) | 2.25 mg in 0.1 mL |
| Clindamycin (anaerobe / Bacillus cover) | 1 mg in 0.1 mL |
| Amikacin (if Bacillus / penicillin allergy) | 0.4 mg in 0.1 mL |
Caution: Intravitreal aminoglycosides (amikacin, gentamicin) risk macular infarction - use selectively.
- Intravitreal Voriconazole 100 μg/0.1 mL, OR
- Intravitreal Amphotericin B 5 μg/0.1 mL
STEP 3 — Systemic (IV) Antibiotics
- Broad-spectrum IV antibiotics at doses used for meningitis/severe infections
- IV Vancomycin + IV Ceftriaxone/Piperacillin-tazobactam (empiric)
- Modify based on culture sensitivity
- IV drug users: IV aminoglycoside + clindamycin (Bacillus cereus cover)
- Good vitreous penetration is essential - fluoroquinolones achieve best penetration
STEP 4 — Adjunctive Topical Therapy
- Cycloplegic: Atropine 1% TID (prevents posterior synechiae, reduces ciliary spasm)
- Topical steroids: once fungal aetiology ruled out (prednisolone acetate 1% q1-4h)
- Topical antibiotics (fortified): Vancomycin 5% + Tobramycin/Cefazolin drops
STEP 5 — Pars Plana Vitrectomy (PPV)
- No response to intravitreal + IV antibiotics within 24-48 hours
- Fungal aetiology (requires vitrectomy for adequate antifungal delivery)
- Dense vitreous opacification
- Early stages with potential for vision salvage
- Reduces infective and inflammatory load
- Provides adequate material for culture + histopathology
- Permits intravitreal antibiotics at higher concentrations
- Clears vitreous media
STEP 6 — Evisceration (if Globe Salvage Fails)
- No light perception (NLP) + failure of all medical/surgical treatment
- Threat to life (spreading orbital/intracranial infection)
- Blind, painful, cosmetically unacceptable eye
- Impending corneal perforation with uncontrolled infection
| Procedure | Description | Preferred when |
|---|---|---|
| Evisceration | Removal of ocular contents, scleral shell preserved | Panophthalmitis (scleral shell limits orbital spread debate; better cosmesis with implant) |
| Enucleation | Removal of entire globe | Suspected intraocular tumour; sympathetic ophthalmia risk; orbital invasion |
Sympathetic ophthalmia caveat: Evisceration in panophthalmitis is generally safe but classical teaching recommends enucleation within 14 days of penetrating injury if there is risk of sympathetic ophthalmia. In practice, evisceration is widely performed.
PROGNOSIS
- Visual prognosis is very poor once NLP is established
- Retina is extremely intolerant of suppurative inflammation - irreversible injury can occur within hours
- Even with aggressive treatment, most eyes with true panophthalmitis retain little or no useful vision
- Life-threatening complications must be actively excluded
COMPLICATIONS
Ocular:
- Corneal perforation
- Phthisis bulbi (end-stage shrunken eye)
- Hypotony or secondary glaucoma
- Retinal detachment
- Subretinal/choroidal abscess
Orbital & Systemic:
- Orbital abscess
- Orbital cellulitis
- Cavernous sinus thrombosis (life-threatening)
- Meningitis / intracranial extension
- Septicaemia / multi-organ failure
- Sympathetic ophthalmia (fellow eye)
KEY TEACHING POINTS FOR VIVA
- Panophthalmitis = endophthalmitis + scleral/orbital extension (Tenon's involvement distinguishes it)
- Most common cause exogenous: penetrating trauma, especially organic material (agricultural injuries - Bacillus, Aspergillus)
- IV drug users: think Bacillus cereus → treat with aminoglycoside + clindamycin
- Klebsiella pneumoniae endogenous panophthalmitis is classic in East Asian patients with liver abscess or DM
- B-scan findings: T-sign (scleral thickening + subtenon fluid), dense vitreous echoes
- Intravitreal vancomycin + ceftazidime = empirical first-line intravitreal therapy
- Retina tolerates suppuration for only a few hours - time is vision
- NLP + failed treatment = evisceration (don't delay surgical intervention when eye is unsalvageable)
- Multi-disciplinary: Ophthalmology + ID + Medicine - always do systemic workup
- Steroids only after fungal aetiology excluded
SUMMARY TABLE
| Domain | Key Point |
|---|---|
| Definition | Inflammation of entire globe extending to Tenon's/orbit |
| Aetiology (most common) | Penetrating trauma (exogenous); sepsis (endogenous) |
| Organisms | Bacteria (Staph, Bacillus, Streptococcus, Pseudomonas) |
| Symptoms | Severe pain, NLP/severe VL, swelling, discharge, fever |
| Signs | Hypopyon, NLP, proptosis, restricted EOM, chemosis, absent red reflex |
| Key investigation | B-scan US, vitreous tap for C&S, blood cultures, CT orbit |
| Intravitreal Rx | Vancomycin 1mg + Ceftazidime 2.25 mg |
| Systemic Rx | IV broad-spectrum antibiotics (meningitis-dose) |
| Surgical escalation | PPV → Evisceration (if NLP + failed Rx) |
| Prognosis | Very poor for vision; systemic complications can be fatal |