Antibiotic stewardship
Reading File
Finding Sources
Searching PubMed
"antibiotic stewardship" AND outcomes
Searching the Web
antibiotic stewardship programs principles 2024 2025 guidelines
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from Harrison's 22E, Red Book 2021, Harriet Lane, Tietz, Sherris, and Fischer's Surgery. Let me compose the full answer.
Antibiotic Stewardship
Definition
Antibiotic (antimicrobial) stewardship is a coordinated set of actions that promote responsible use of antimicrobials to ensure sustainable access for those who need them. In practice it means "coordinated interventions designed to improve and measure the appropriate use of antimicrobial agents by promoting the selection of the optimal antimicrobial drug regimen including dose, duration of therapy, and route of administration."
- Tietz Textbook of Laboratory Medicine, 7th Ed.
It is far more than just picking the "right" antibiotic - it also covers empiric therapy concordance with guidelines, dose optimization, shortest effective duration, preferential use of agents with lower C. difficile risk, proper surgical prophylaxis, and explicitly avoiding antibiotics where they are not indicated (viral URIs, asymptomatic bacteriuria).
Why Stewardship Matters
- Antimicrobial resistance (AMR): The CDC has identified AMR as one of the most serious health threats globally. More than 2 million people are infected with antibiotic-resistant organisms annually in the US, causing >20,000 deaths.
- Collateral damage: Antibiotic use selects for resistant organisms (MRSA, ESBL-producers, CRE, VRE) and drives Clostridioides difficile colitis - consequences that extend beyond the treated patient into the community. - Fischer's Mastery of Surgery, 8th Ed.
- Inappropriate prescribing scale: Ambulatory antibiotic use accounts for ~85% of total antibiotic use in most developed countries, making outpatient settings a critical stewardship target. - Harrison's Principles of Internal Medicine, 22E (2025)
Goals of Antimicrobial Stewardship Programs (ASPs)
- Improve patient care through appropriate antimicrobial use
- Preserve antimicrobials as a health resource by curbing resistance
- Reduce incidence of adverse drug effects (including C. diff, nephrotoxicity)
- Control healthcare costs
- Harrison's 22E
The 7 CDC Core Elements of Hospital ASPs
These apply to inpatient facilities and are the recognized framework in the US:
| # | Core Element | What It Means |
|---|---|---|
| 1 | Leadership Commitment | Hospital administration dedicates human, financial, and IT resources; provides dedicated time to program leaders |
| 2 | Accountability | A physician leader + pharmacist co-leader with clear responsibility for program management |
| 3 | Pharmacy Expertise | Pharmacist with infectious disease training co-leads implementation |
| 4 | Action | Concrete interventions - prospective audit + feedback, preauthorization, guideline implementation, IV-to-oral conversion, dose optimization |
| 5 | Tracking | Monitor antibiotic use (days of therapy/1,000 patient-days), C. diff rates, resistance patterns using tools like CDC's NHSN AUR module (SAAR metric) |
| 6 | Reporting | Regular feedback to prescribers, pharmacists, nurses, and leadership |
| 7 | Education | Annual training for all healthcare workers; patient/family education |
- Red Book 2021 (AAP), Tietz Laboratory Medicine 7th Ed.
Key ASP Interventions
Prospective Audit and Feedback
Orders for broad-spectrum agents (carbapenems, daptomycin, ceftazidime-avibactam) are reviewed regularly by an ID physician or pharmacist. When use can be optimized, the ASP team intervenes and recommends alternatives. This "handshake stewardship" model has demonstrated declines in broad-spectrum drug use and reductions in adverse events including C. difficile infection.
Formulary Restriction
A limited set of antimicrobials is included in the hospital formulary to limit indiscriminate use and avoid unnecessary drug expenditure.
Preauthorization
Clinicians must obtain approval before prescribing certain antimicrobials, functioning as a gatekeeper for high-value or high-risk agents.
De-escalation
Once culture and sensitivity data return, broad empiric regimens should be narrowed to targeted therapy. Narrower-spectrum agents are often more bactericidal and cause less damage to commensal microbiota than broad-spectrum drugs.
- Sherris & Ryan's Medical Microbiology, 8th Ed.
IV-to-Oral (IV-to-PO) Conversion
Switching from intravenous to oral antibiotics when clinically appropriate reduces costs, line-associated complications, and hospital length of stay.
Duration Optimization
"Shorter may be better." Treating for the briefest effective duration reduces selective pressure on bystander flora. For example, 4 days of antimicrobial therapy has been shown as effective as longer regimens for complicated intra-abdominal infections following adequate source control.
- Fischer's Mastery of Surgery 8th Ed., Tietz 7th Ed.
Outpatient / Ambulatory Stewardship
The CDC's 2016 Core Elements of Outpatient Antibiotic Stewardship define four components:
- Commit to improving antibiotic prescribing
- Implement at least one policy/practice to improve prescribing and assess effectiveness
- Monitor prescribing and provide feedback
- Provide educational resources to clinicians and patients
Effective ambulatory interventions include peer comparison, accountable justification (requiring written reasoning), precommitment, clinical decision support tools, patient education, and multifaceted combined interventions. Communication training - making a clear diagnosis, setting expectations for illness course, identifying red flags - is particularly effective.
What does NOT work well: Procalcitonin testing has been unproven for reducing ambulatory antibiotic prescribing. CRP testing effects are not durable. Delayed antibiotic prescriptions are explicitly discouraged - they are conceptually flawed, burden the patient with clinical decisions, and send a mixed message about appropriateness of antibiotics for respiratory infections.
- Harrison's 22E (2025)
Stewardship in Surgery
Surgeons play a unique and important role. Key surgical stewardship principles:
-
Limit prophylactic antibiotics to procedures with meaningful SSI risk
-
Use narrow-spectrum agents for prophylaxis (e.g., cefazolin)
-
Ensure adequate tissue levels at incision; re-dose for prolonged procedures
-
Discontinue prophylaxis once the procedure is complete - do not continue postoperatively for uncomplicated cases
-
Obtain cultures before starting empiric therapy; then de-escalate when culture data return
-
Source control (surgical or interventional) is indispensable - it reduces microbial burden and enables shorter antibiotic courses
-
ASP team membership is now required by Joint Commission (JCAHO), CMS, and many state bodies
-
Fischer's Mastery of Surgery 8th Ed.
Stewardship in Pediatrics (AAP / Choosing Wisely)
The AAP and PIDS "Five Things to Question" include:
-
Don't start empiric antibiotics without first obtaining appropriate cultures (blood, urine, etc.)
-
Don't use broad-spectrum agents for perioperative prophylaxis or continue prophylaxis after wound closure in clean/clean-contaminated procedures
-
Don't treat uncomplicated CAP in otherwise healthy hospitalized children with anything broader than ampicillin
-
Consult local antibiograms and ID specialists for resistant organism questions (MRSA, ESBL, CRE, VRE)
-
Red Book 2021, Harriet Lane Handbook 23rd Ed.
Stewardship and Diagnostics
The lab is a critical partner. The role of diagnostics in stewardship:
- Cultures should ideally be obtained before starting antibiotics in non-emergency situations
- Newer molecular methods (rapid PCR panels, whole-genome sequencing) can dramatically shorten time-to-targeted-therapy and create de-escalation opportunities
- Procalcitonin is used in some settings (e.g., CAP, ICU sepsis) to guide duration - but its ambulatory value remains unproven
- Antibiogram data (local resistance patterns) guides empiric therapy selection at the institutional level
What Not to Do (Common Stewardship Pitfalls)
| Bad Practice | Reason |
|---|---|
| Antibiotics for viral URIs/rhinosinusitis | No benefit; promotes resistance |
| Treating asymptomatic bacteriuria | Unnecessary; increases resistance risk |
| Prolonged surgical prophylaxis | No evidence of benefit after closure; increases C. diff and resistance risk |
| Delayed antibiotic prescriptions | Conceptually flawed; burdens patient |
| Failing to de-escalate after cultures return | Maintains unnecessary broad-spectrum pressure |
| Subtherapeutic dosing/intermittent administration | Promotes resistance without curing infection |
Recent Evidence (PubMed, 2024-2026)
- AI in ASPs (PMID 39955846): A 2025 systematic review shows AI-driven tools are increasingly being applied to optimize antibiotic prescribing within stewardship programs.
- Procalcitonin for pneumonia stewardship (PMID 41412284): A 2026 systematic review examines whether procalcitonin-guided management produces different stewardship outcomes in European vs. US settings - outcomes differ by context.
- Dental ASPs (PMID 39400429): A 2025 systematic review of dental antibiotic stewardship interventions shows growing evidence that dentistry is a major contributor to outpatient antibiotic overuse and a target for stewardship.
Summary
Antibiotic stewardship is not a single act but a structured, multidisciplinary program. The core message across all settings is: right drug, right dose, right route, right duration - and critically, no antibiotic when one is not needed. Successful stewardship reduces resistance, C. difficile infection, adverse effects, and costs while improving patient outcomes. It is now a regulatory requirement in hospital settings (JCAHO, CMS) and a public health imperative globally.
Give me details preferred antibiotics according to each site
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I have all the content I need. Let me compile the comprehensive site-by-site antibiotic reference.
Preferred Antibiotics by Site of Infection
Based on Katzung's Basic & Clinical Pharmacology 16th Ed., Lippincott Illustrated Reviews Pharmacology, and Harrison's Principles of Internal Medicine 22E (2025)
1. Central Nervous System - Meningitis
| Patient Group | Common Pathogens | Drug of First Choice | Alternatives |
|---|---|---|---|
| Neonate | Group B Streptococcus, E. coli, Listeria monocytogenes | Ampicillin + 3rd-gen cephalosporin | Ampicillin + aminoglycoside; chloramphenicol; meropenem |
| Child | H. influenzae, S. pneumoniae, N. meningitidis | Ceftriaxone + vancomycin | Chloramphenicol, meropenem |
| Adult 18-50 yrs | S. pneumoniae, N. meningitidis | Ceftriaxone | Vancomycin + ceftriaxone |
| Adult >50 yrs / immunocompromised | S. pneumoniae, N. meningitidis, Listeria | Ceftriaxone + ampicillin | Vancomycin + ceftriaxone + ampicillin |
Key principle: Add vancomycin whenever S. pneumoniae is suspected and local resistance to penicillin/cephalosporins is a concern. Add ampicillin to cover Listeria in neonates, elderly, and immunocompromised patients.
2. Respiratory Tract
Upper Respiratory - Acute Otitis Media & Sinusitis
| Pathogens | First Choice | Alternatives |
|---|---|---|
| H. influenzae, S. pneumoniae, M. catarrhalis | Amoxicillin | Amoxicillin-clavulanate; cefuroxime axetil; cefpodoxime |
Lower Respiratory - Pneumonia
| Patient Group | Common Pathogens | First Choice | Notes |
|---|---|---|---|
| Neonate | Same as neonatal meningitis | Ampicillin + 3rd-gen cephalosporin | - |
| Child | S. pneumoniae, S. aureus, H. influenzae | Ceftriaxone, cefuroxime, or cefotaxime | Ampicillin-sulbactam as alternative |
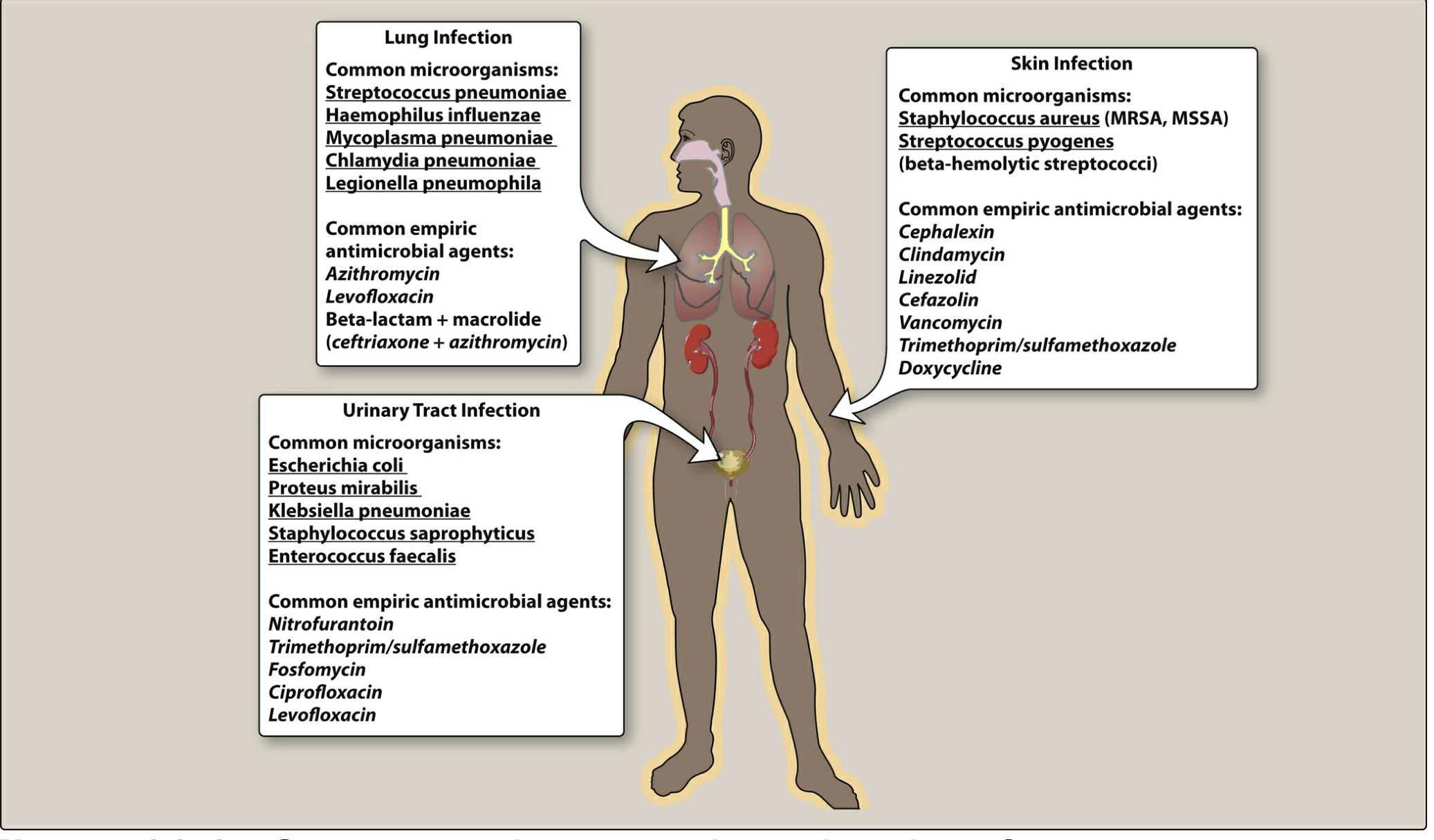
| CAP - Outpatient, healthy | S. pneumoniae, Mycoplasma, Legionella, H. influenzae, Chlamydia | Macrolide (azithromycin/clarithromycin), amoxicillin, or doxycycline | No comorbidities, no recent antibiotics |
| CAP - Outpatient, comorbidities | Same + drug-resistant S. pneumoniae risk | Respiratory fluoroquinolone (levofloxacin/moxifloxacin) OR amoxicillin-clavulanate/cefuroxime/cefpodoxime + macrolide or doxycycline | Diabetes, heart/lung/liver/renal disease, asplenia, immunosuppression, recent antibiotics |
| CAP - Inpatient | Same | Macrolide or doxycycline + cefotaxime/ceftriaxone/ertapenem; OR respiratory fluoroquinolone alone | |
| HAP / VAP (Hospital-acquired) | S. aureus (MRSA), Pseudomonas aeruginosa, Enterobacterales | Vancomycin or linezolid (MRSA coverage) + piperacillin-tazobactam or cefepime or antipseudomonal carbapenem ± aminoglycoside or respiratory fluoroquinolone | Tailor to local antibiogram |
3. Cardiovascular - Bacterial Endocarditis
| Type | Common Pathogens | First Choice | Alternatives |
|---|---|---|---|
| Acute (rapid onset, virulent) | S. aureus | Vancomycin + ceftriaxone | Penicillinase-resistant penicillin (nafcillin/oxacillin) + gentamicin |
| Subacute (indolent) | Viridans streptococci, enterococci | Penicillin + gentamicin | Vancomycin + gentamicin |
4. Gastrointestinal / Intra-abdominal
| Condition | Common Pathogens | First Choice | Alternatives |
|---|---|---|---|
| Peritonitis / Ruptured viscus / IAI | Coliforms, B. fragilis, Enterococci, viridans streptococci | Metronidazole + 3rd-gen cephalosporin OR piperacillin-tazobactam | Carbapenem (meropenem/imipenem); tigecycline; metronidazole + fluoroquinolone |
Source control (surgical/interventional) is mandatory - it permits shorter antibiotic courses (as few as 4 days post-source control for complicated IAI).
5. Urinary Tract
| Type | Common Pathogens | First Choice | Notes |
|---|---|---|---|
| Uncomplicated UTI (cystitis) | E. coli, K. pneumoniae, P. mirabilis, S. saprophyticus, Enterococci | TMP-SMX, fosfomycin, nitrofurantoin | Nitrofurantoin avoids systemic exposure; fosfomycin is single-dose; avoid TMP-SMX if local resistance >20% |
| Complicated UTI / Pyelonephritis | Same + broader gram-negatives | Fluoroquinolone (ciprofloxacin/levofloxacin) OR ceftriaxone (IV, hospitalized) | Step-down to oral once improving; adjust per culture |
6. Skin & Soft Tissue
| Condition | Common Pathogens | First Choice | Notes |
|---|---|---|---|
| Non-purulent (cellulitis, erysipelas) - no MRSA concern | S. pyogenes (Group A Strep), MSSA | 1st-gen cephalosporin (cephalexin PO / cefazolin IV) or penicillinase-resistant penicillin (dicloxacillin/nafcillin) | Beta-hemolytic strep is the primary target |
| Purulent (abscess, furuncle) - MRSA suspected | S. aureus (MRSA) | TMP-SMX, doxycycline (outpatient) OR linezolid, vancomycin, daptomycin (inpatient/severe) | Always drain abscesses - antibiotics are adjunctive |
| Diabetic foot infection | Above + Enterobacterales, B. fragilis, Enterococci (polymicrobial) | Ceftriaxone/cefepime/levofloxacin/ciprofloxacin + metronidazole; OR ampicillin-sulbactam; OR piperacillin-tazobactam; OR carbapenem ± vancomycin/linezolid (if MRSA risk) | Assess vascularity; surgical debridement often needed |
| Necrotizing fasciitis (Group A Strep) | S. pyogenes ± polymicrobial | Penicillin + clindamycin (clindamycin suppresses toxin production) | Surgical emergency - immediate debridement |
7. Bone & Joint
| Type | Common Pathogens | First Choice | Alternatives |
|---|---|---|---|
| Septic arthritis - Child | H. influenzae, S. aureus, beta-hemolytic streptococci | Vancomycin + ceftriaxone | Vancomycin + ampicillin-sulbactam or ertapenem |
| Septic arthritis - Adult | S. aureus, Enterobacterales, N. gonorrhoeae | Vancomycin + ceftriaxone | Vancomycin + ertapenem; or fluoroquinolone (if gonococcal) |
| Osteomyelitis (hematogenous) | S. aureus (most common) | Anti-staphylococcal penicillin (MSSA) or vancomycin (MRSA) | TMP-SMX or doxycycline (MRSA, outpatient) |
8. Septicemia / Bloodstream Infection
| Context | First Choice | Notes |
|---|---|---|
| Sepsis (unknown source) | Vancomycin + 3rd-gen cephalosporin OR piperacillin-tazobactam OR imipenem/meropenem | Start within 1 hour of diagnosis; de-escalate once cultures return |
| Febrile neutropenia / Granulocytopenia | Antipseudomonal penicillin + aminoglycoside; OR ceftazidime; OR cefepime; OR imipenem/meropenem; add vancomycin if catheter infection or severe mucositis suspected; consider antifungal if fever persists >5-7 days on empiric antibiotics | Broad coverage mandatory; Pseudomonas must be covered |
9. Sexually Transmitted Infections (STIs)
| Infection | First Choice | Alternatives / Notes |
|---|---|---|
| Gonorrhea (uncomplicated) | Ceftriaxone IM (single dose) | Fluoroquinolone resistance is widespread - avoid empirically |
| Chlamydia | Doxycycline x 7 days OR azithromycin 1g single dose | Always treat both gonorrhea AND chlamydia empirically in urethritis/cervicitis |
| Syphilis (primary/secondary) | Benzathine penicillin G IM (single dose) | Doxycycline if penicillin-allergic |
| Pelvic inflammatory disease | Ceftriaxone + doxycycline ± metronidazole | Cover gonorrhea, chlamydia, and anaerobes |
Key Stewardship Reminders by Site
| Site | Do This | Avoid |
|---|---|---|
| Respiratory | Use narrowest spectrum for CAP outpatient (amoxicillin/macrolide) | Broad-spectrum for mild uncomplicated CAP |
| UTI | Nitrofurantoin or fosfomycin for simple cystitis | Fluoroquinolones as first-line for uncomplicated cystitis (reserve for complicated UTI) |
| Skin | Drain abscesses; antibiotics are adjunctive | Treating asymptomatic colonization |
| IAI | Source control first; limit to 4 days post-control | Prolonged antibiotics without source control |
| Meningitis/Endocarditis | Bactericidal therapy is mandatory | Bacteriostatic agents (e.g., clindamycin) as sole therapy |
| All sites | De-escalate once culture data return | Continuing broad empiric therapy after organism identified |
- Katzung's Basic & Clinical Pharmacology 16th Ed., Table on Empiric Antimicrobial Therapy by Site
- Lippincott Illustrated Reviews: Pharmacology (Figure 28.2)
- Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.