Rectal prolapse
Reading File
search_medical_text
rectal prolapse classification etiology diagnosis management surgery
search_medical_image
rectal prolapse clinical image anatomy
GradeResponse
GradeResponse
Rectal Prolapse
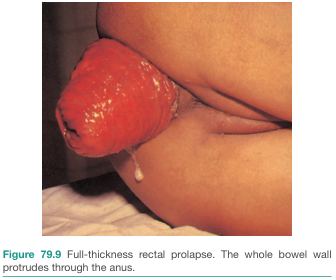
Rectal prolapse is the protrusion of the rectal wall through the anal orifice. It ranges from partial mucosal descent to complete full-thickness extrusion of the rectal wall.
Classification
| Type | Description |
|---|---|
| Mucosal prolapse | Only the mucosa protrudes; muscularis propria remains in place |
| Full-thickness (complete) prolapse | All layers of the rectal wall protrude through the anus |
| Internal rectal prolapse (intussusception) | Rectum telescopes internally without external protrusion; a precursor to full-thickness prolapse |
Etiology & Predisposing Factors
- Children: Typically mucosal, associated with malnutrition, cystic fibrosis, chronic diarrhea, or straining
- Adults: More common in older women (though men are also affected); associated with:
- Chronic straining / constipation
- Multiparity and pelvic floor laxity
- Neurological conditions (e.g., cauda equina lesions, multiple sclerosis)
- Redundant sigmoid colon / deep pouch of Douglas
- Pudendal neuropathy
- Prior pelvic surgery
Clinical Features
- Visible red mass protruding from the anus, especially on straining or defecation
- Mucus or blood-stained discharge
- Fecal incontinence (common, due to sphincter stretch and pudendal nerve injury)
- Constipation or obstructed defecation
- Perineal heaviness or discomfort
- In advanced cases: ulceration, edema, or incarceration of prolapsed tissue
Diagnosis
Clinical examination is usually sufficient:
- Inspect at rest and during straining (squatting position or sitting on a commode is ideal)
- Digital rectal exam: assess sphincter tone (often reduced)
- Differentiate from prolapsing hemorrhoids (see below)
Differentiating full-thickness prolapse from prolapsing hemorrhoids:
| Feature | Full-thickness Prolapse | Prolapsing Hemorrhoids |
|---|---|---|
| Mucosal folds | Concentric (circular) | Radial |
| Sulcus between mass and anal skin | Absent | Present |
| Consistency | Cylinder of bowel wall | Discrete cushions |
| Incontinence | Common | Less common |
Further investigations (selected cases):
- Defecating proctogram / MRI defecography: identifies internal prolapse, enterocele, associated pelvic floor disorders
- Colonoscopy: if concern for coincident colorectal pathology
- Anorectal manometry: pre-operative baseline for sphincter function
- EMG / pudendal nerve terminal motor latency: assess degree of neuropathy
Management
Children
Conservative management is preferred (Bailey & Love's, p. 1418):
- Treat underlying cause (nutritional supplementation, treat diarrhea, cystic fibrosis management)
- Manual reduction after each episode
- Strapping the buttocks between episodes
- Most resolve spontaneously with growth
Adults — Full-Thickness Prolapse
Surgery is almost always necessary for full-thickness rectal prolapse (Bailey & Love's, p. 1418).
Surgical approaches fall into two categories:
1. Perineal Approaches
Preferred for elderly/high-risk patients with significant comorbidities:
| Procedure | Description |
|---|---|
| Delorme's procedure | Mucosal sleeve resection + plication of muscularis propria; lower morbidity |
| Altemeier's procedure (perineal rectosigmoidectomy) | Full-thickness resection of prolapsed bowel via perineum; useful for large/incarcerated prolapse |
| Thiersch wire / Encirclement | Subcutaneous suture/wire around anus to reduce outlet; largely historical |
2. Abdominal Approaches
Generally preferred in fit patients — lower recurrence rates:
| Procedure | Description |
|---|---|
| Resection rectopexy | Rectum mobilized, sigmoid resected, rectum fixed to sacrum; addresses constipation |
| Suture rectopexy (Wells / posterior mesh rectopexy) | Rectum fixed to sacrum without resection; lower risk but may worsen constipation |
| Ventral mesh rectopexy (D'Hoore) | Laparoscopic; mesh fixed anteriorly; gaining popularity, especially for associated pelvic organ prolapse |
| Laparoscopic approaches | Now preferred over open; equivalent recurrence rates with faster recovery |
Complications
- Incarceration / strangulation: surgical emergency requiring urgent reduction or operative intervention
- Ulceration and bleeding: from repeated trauma to exposed mucosa
- Fecal incontinence: may persist even after successful repair (due to irreversible sphincter/nerve damage)
- Recurrence: higher after perineal procedures (~20–30%) vs. abdominal procedures (~5–10%)
- Constipation: may worsen after rectopexy without sigmoid resection
Prognosis
- In children, the prognosis is excellent with conservative management
- In adults, surgical repair reliably prevents recurrence; however, continence may not fully recover post-operatively, especially when pudendal neuropathy is established
- Pelvic floor physiotherapy is an important adjunct pre- and post-operatively
Primary reference: Bailey and Love's Short Practice of Surgery, 28th Edition, pp. 1418–1419
This is a shared conversation. Sign in to Orris to start your own chat.