Explain the counter current mechanism of urine formation of RENAL PHYSIOLOGY in detailed explanation with flowcharts
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content and images. Let me compile the full detailed explanation.
Countercurrent Mechanism of Urine Formation - Renal Physiology
Overview
The kidneys can produce urine ranging from 50 mOsm/L (very dilute) to 1200-1400 mOsm/L (maximally concentrated). This extraordinary ability depends on two related but distinct mechanisms:
- Countercurrent Multiplication - actively builds a hyperosmotic medullary gradient
- Countercurrent Exchange - passively preserves that gradient
Both depend on the hairpin (U-shaped) anatomy of the loop of Henle and the vasa recta.
PART 1: Anatomical Basis
CORTEX
|
|── Proximal Tubule (isotonic, ~300 mOsm)
|
↓ Descending Limb (thin) ──────────────┐
↓ │ LOOP OF HENLE
↓ [TIP OF LOOP] ~1200 mOsm │ (U-shape)
↓ │
↑ Thin Ascending Limb │
↑ Thick Ascending Limb ────────────────┘
|
|── Distal Tubule → Collecting Duct
| ↓ (passes back through medulla)
| Papillary tip → Renal Pelvis → Ureter
Key anatomical facts:
- ~25% of nephrons are juxtamedullary nephrons with long loops reaching the papillary tip
- The vasa recta (peritubular capillaries) run parallel to these long loops in the same U-shape
- This parallel arrangement is the physical basis for both countercurrent processes
- Guyton and Hall Textbook of Medical Physiology
PART 2: Permeability Properties of Each Segment
This table is the foundation of understanding how concentration gradients are built:
| Segment | Active NaCl Transport | Water Permeability | NaCl Permeability | Urea Permeability |
|---|---|---|---|---|
| Proximal tubule | ++ | ++ | + | + |
| Thin descending limb | 0 | ++ | + | + |
| Thin ascending limb | 0 | 0 | + | + |
| Thick ascending limb | ++ | 0 | 0 | 0 |
| Distal tubule | + | +ADH | 0 | 0 |
| Cortical collecting duct | + | +ADH | 0 | 0 |
| Inner medullary collecting duct | + | +ADH | 0 | +ADH |
The "magic" key: The thick ascending limb actively pumps NaCl out but is impermeable to water - this is the "single effect" that drives everything. (Guyton and Hall, Table 29.1)
PART 3: Countercurrent Multiplier - Step by Step
The "Single Effect"
The thick ascending limb uses the Na-K-2Cl cotransporter (NKCC2) to actively pump Na+, K+, and Cl- into the interstitium. Because this segment is water-impermeable, water cannot follow. This creates a ~200 mOsm/L gradient between the tubule lumen and the surrounding interstitium at any given level.
How a 200 mOsm Single Effect Becomes a 900 mOsm Gradient
The countercurrent flow multiplies this single effect progressively:
STEP 0 - Starting Condition (all segments at 300 mOsm)
─────────────────────────────────────────────────────
Descending │ Interstitium │ Ascending
300 │ 300 │ 300
300 │ 300 │ 300
300 │ 300 │ 300
300 │ 300 │ 300 ← tip
STEP 1 - Single Effect (pump in ascending limb creates 200 mOsm gradient)
─────────────────────────────────────────────────────
Descending │ Interstitium │ Ascending
350 │ 350 │ 150 ← 200 mOsm difference maintained
350 │ 350 │ 150
350 │ 350 │ 150
350 │ 350 │ 150 ← tip
STEP 2 - Axial Shift (fluid flows down descending, up ascending)
─────────────────────────────────────────────────────
Descending │ Interstitium │ Ascending
300 │ 325 │ 325
350 │ 350 │ 150
350 │ 350 │ 150
400 │ 400 │ 200 ← more concentrated at tip
STEP 3 - Single Effect Again
─────────────────────────────────────────────────────
Descending │ Interstitium │ Ascending
325 │ 325 │ 125
350 │ 375 │ 175
400 │ 400 │ 200
500 │ 500 │ 300 ← tip builds up further
... repeat many cycles ...
FINAL STATE (antidiuresis):
─────────────────────────────────────────────────────
Descending │ Interstitium │ Ascending ← Level
300 │ 300 │ 100 ← cortex
600 │ 600 │ 400 │
900 │ 900 │ 700 │ deeper medulla
1200 │ 1200 │ 1000 ← papillary tip
The countercurrent flow in adjacent limbs is what "multiplies" each small (200 mOsm) single effect into a large (900+ mOsm) corticomedullary gradient. - Medical Physiology (Boron & Boulpaep)
PART 4: Role of Each Tubular Segment
1. Proximal Tubule
- Reabsorbs ~65% of filtered Na+, water, and solutes
- Highly permeable to water → fluid remains isotonic at ~300 mOsm
- Volume delivered to loop: 44 mL/min (from 125 mL/min GFR)
2. Thin Descending Limb
- Highly permeable to water, poorly permeable to solutes
- As fluid descends through the increasingly hyperosmotic medulla, water is drawn OUT by osmosis
- Tubular fluid becomes progressively concentrated
- By the hairpin tip: ~1200 mOsm/L (in antidiuresis)
- Also contains AQP-1 channels for facilitated water movement
- Passive urea secretion (via UT-A2) can occur into the descending limb
3. Thin Ascending Limb
- Impermeable to water (critical!)
- NaCl passively diffuses OUT into the interstitium (because it became so concentrated during descending)
- This is the passive component of the single effect
- Fluid starts to dilute as NaCl leaves but water cannot follow
4. Thick Ascending Limb (TAL) - THE WORKHORSE
- Impermeable to water (critical!)
- Actively pumps Na+, K+, Cl- via NKCC2 cotransporter (apical) and Na-K-ATPase (basolateral)
- Also paracellular Na+ driven by lumen-positive voltage
- Can generate up to 200 mOsm gradient between lumen and interstitium (the "single effect")
- Fluid leaving the TAL is very dilute: ~100-150 mOsm (the "diluting segment")
- This is why the TAL is also called the "diluting segment"
TAL Mechanism:
──────────────────────────────────────────────────
Lumen Interstitium
Apical
Na+ ─────────────NKCC2──────────────→ Na+ added
K+ ─────────────NKCC2──────────────→ to interstitium
2Cl-─────────────NKCC2──────────────→ (solutes without water)
Na+ ──paracellular (lumen +ve)──────→
Basolateral
Na-K-ATPase maintains gradient
──────────────────────────────────────────────────
Net: Luminal fluid DILUTES; Interstitium CONCENTRATES
5. Distal Tubule
- Continues to reabsorb NaCl (though less actively)
- Water permeability is ADH-dependent
- With ADH: some water reabsorption, fluid remains ~isosmotic to cortex (~300 mOsm)
- Without ADH: remains dilute (~100 mOsm)
6. Collecting Duct (Cortical then Medullary)
- Cortical: ADH increases water permeability via AQP-2 insertion into apical membrane
- Medullary: passes through increasingly hyperosmotic interstitium
- With high ADH → water osmoses out into interstitium → urine concentrates up to 1200 mOsm
- Without ADH → remains dilute → large volume of hypotonic urine excreted
PART 5: Role of Urea in the Medullary Gradient
Urea contributes approximately 40-50% of the inner medullary osmolality. The recycling mechanism is important:
UREA RECYCLING PATHWAY
────────────────────────────────────────────────────────────
Cortical collecting duct:
- ADH ↑ water permeability → water reabsorbed
- ADH does NOT increase urea permeability here
- → Urea CONCENTRATES in tubular fluid
↓
Outer medullary collecting duct:
- Same: water out, urea stays
- Urea [concentration] continues to rise
↓
Inner medullary collecting duct (IMCD):
- ADH activates UT-A1 and UT-A3 urea transporters
- Concentrated urea diffuses DOWN its gradient into interstitium
- Adds to medullary hyperosmolarity
↓
Interstitium (inner medulla):
- Urea diffuses into thin ascending limb (UT-A2)
- → Recycles back through the loop system
- Prevents urea washout from the medulla
────────────────────────────────────────────────────────────
Result: Inner medullary osmolality = NaCl (~600) + Urea (~600) = ~1200 mOsm
- Costanzo Physiology, 7th Edition
PART 6: ADH (Vasopressin/AVP) - The Master Switch
ADH is secreted by the posterior pituitary in response to:
- Increased plasma osmolality (detected by hypothalamic osmoreceptors)
- Decreased blood volume/pressure (via baroreceptors)
Mechanism of action:
ADH released from posterior pituitary
↓
Binds V2 receptors on collecting duct principal cells
↓
↑ cAMP → PKA activation
↓
AQP-2 vesicles inserted into APICAL membrane
↓
Water permeability of collecting duct ↑↑
↓
Water flows by osmosis from lumen → interstitium → vasa recta → blood
↓
Urine concentrates (up to 1200 mOsm)
ADH also:
- Stimulates NKCC2 in the TAL → augments the single effect
- Activates UT-A1/UT-A3 in IMCD → augments urea recycling
- Both effects increase the corticopapillary gradient
PART 7: Countercurrent Exchange in the Vasa Recta
This is a passive process that preserves (not creates) the medullary gradient.
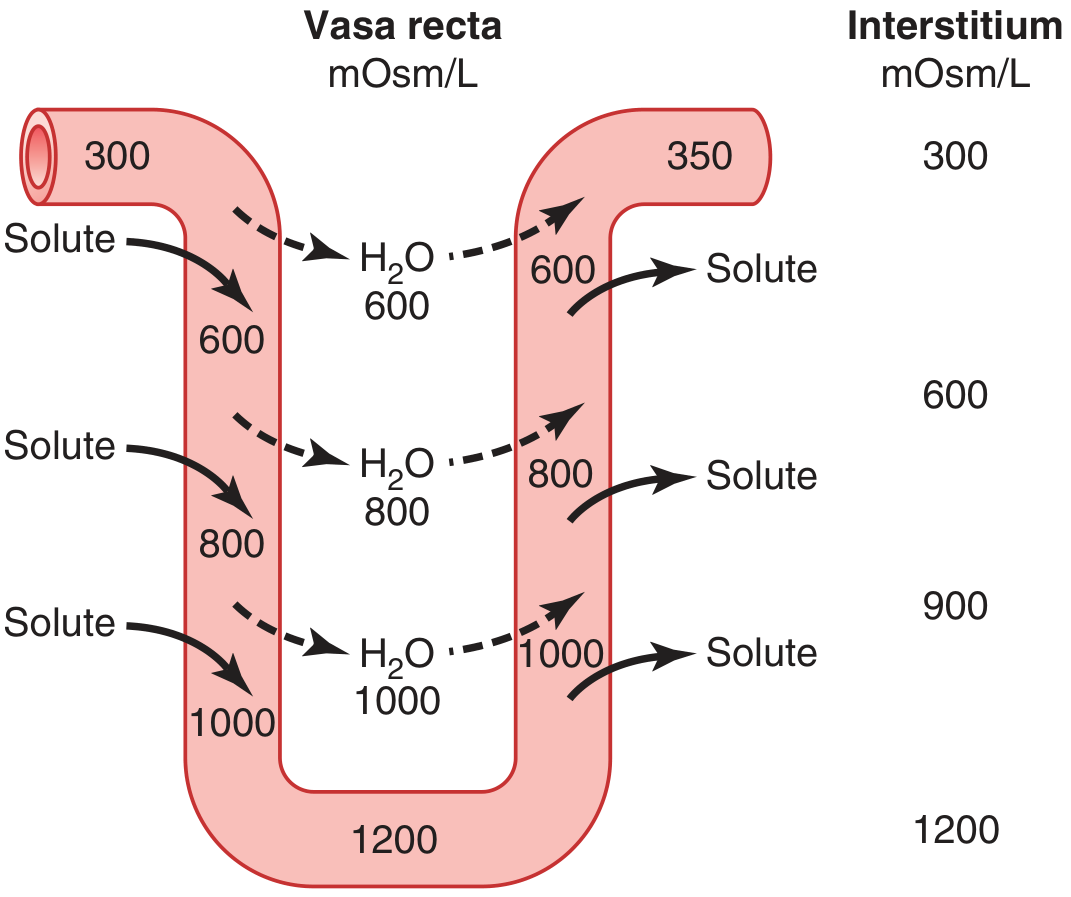
How it works:
DESCENDING VASA RECTA (blood flows toward medulla):
- Enters cortex at 300 mOsm
- As it descends into hyperosmotic medulla:
→ Solutes (NaCl, urea) diffuse IN from interstitium
→ Water diffuses OUT into interstitium
- By the tip: blood reaches ~1200 mOsm (equilibrates with interstitium)
ASCENDING VASA RECTA (blood flows back toward cortex):
- As it ascends into less osmotic regions:
→ Solutes diffuse BACK OUT into interstitium
→ Water diffuses BACK IN
- By the time it exits: ~350 mOsm (nearly back to normal)
KEY INSIGHT: Solutes "short-circuit" from descending to ascending limb.
They never actually leave the medulla - they just cycle between the two limbs.
This is why the gradient is PRESERVED, not washed out.
Comparison:
| Feature | Countercurrent Multiplication | Countercurrent Exchange |
|---|---|---|
| Location | Loop of Henle | Vasa recta |
| Process | Active | Passive |
| Function | CREATES medullary gradient | PRESERVES medullary gradient |
| Energy needed | Yes (NKCC2, Na-K-ATPase) | No |
| Blood flow | N/A | Low (5% of RBF) - important! |
Only 5% of renal blood flow goes to the medulla. High medullary blood flow would "wash out" the gradient - this is why medullary blood flow is deliberately kept low. - Costanzo Physiology, 7th Edition
PART 8: Osmolarity Changes Along the Nephron
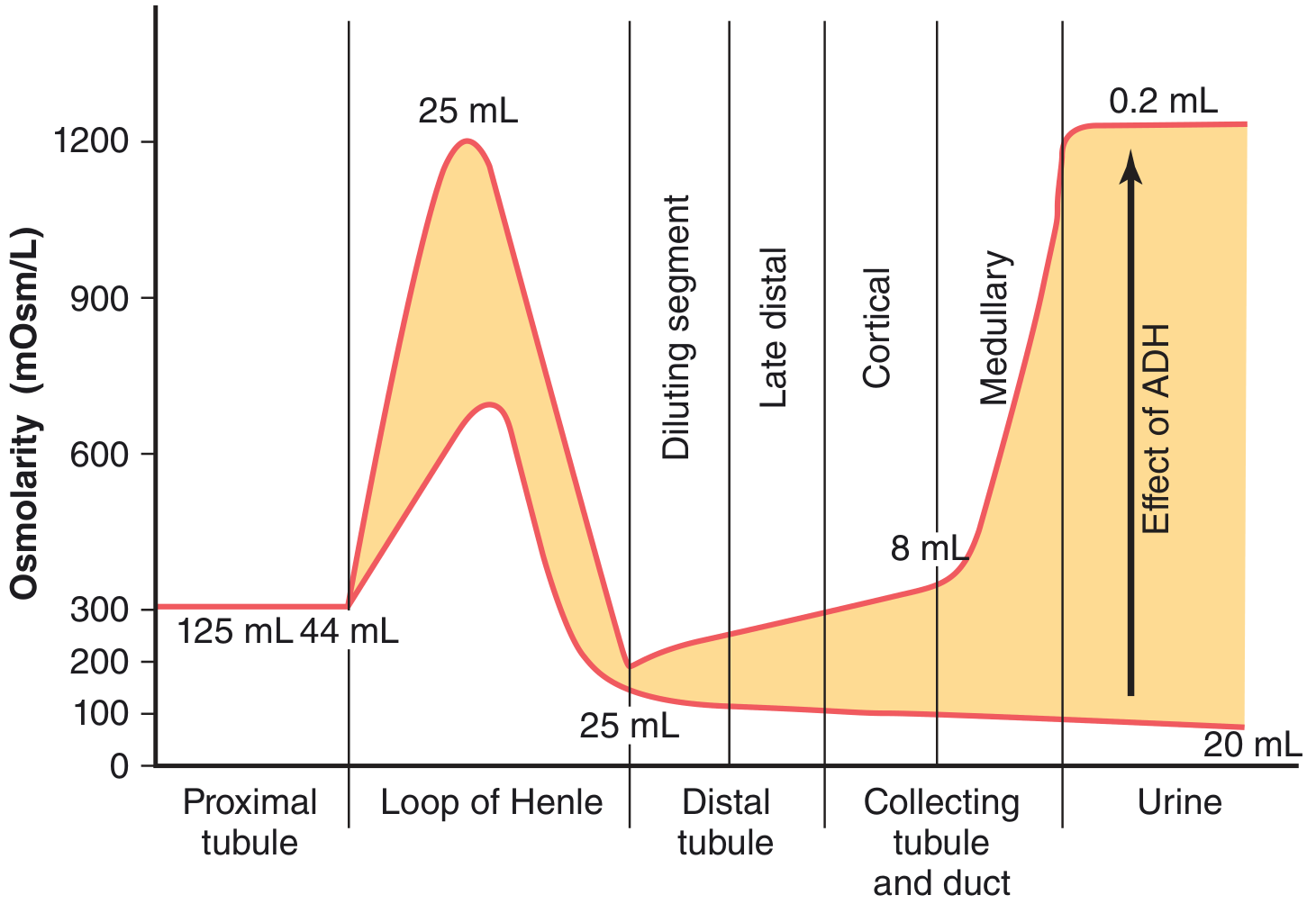
| Segment | Osmolarity (High ADH) | Volume |
|---|---|---|
| Glomerular filtrate | 300 mOsm | 125 mL/min |
| End of proximal tubule | 300 mOsm | 44 mL/min |
| Tip of loop (descending) | ~1200 mOsm | 25 mL/min |
| End of TAL (ascending) | ~100-150 mOsm | 25 mL/min |
| End of distal tubule | ~100 mOsm | ~8 mL/min |
| Final urine (high ADH) | ~1200 mOsm | 0.2 mL/min |
| Final urine (no ADH) | ~50-100 mOsm | 20 mL/min |
PART 9: Master Flowchart - Concentrated Urine Formation
┌─────────────────────────────────────────────────────────┐
│ STIMULUS: Water deprivation / ↑ plasma osmolality │
└────────────────────────┬────────────────────────────────┘
↓
┌─────────────────────────────────────────────────────────┐
│ Hypothalamic osmoreceptors activated │
│ → Posterior pituitary releases ADH (vasopressin) │
└────────────────────────┬────────────────────────────────┘
↓
┌───────────────┴─────────────────┐
↓ ↓
┌────────────────────┐ ┌──────────────────────────┐
│ ADH binds V2R on │ │ ADH stimulates NKCC2 │
│ collecting duct │ │ in thick ascending limb │
│ → AQP-2 insertion │ │ → More NaCl pumped out │
└────────┬───────────┘ └──────────┬───────────────┘
↓ ↓
┌────────────────────┐ ┌──────────────────────────┐
│ Collecting duct │ │ Medullary gradient ↑ │
│ water-permeable │ │ (up to 1200 mOsm) │
└────────┬───────────┘ └──────────┬───────────────┘
└──────────────┬─────────────────┘
↓
┌─────────────────────────────────────────────────────────┐
│ Water osmoses from collecting duct lumen │
│ INTO hyperosmotic medullary interstitium │
│ → Carried away by ascending vasa recta to cortex │
└────────────────────────┬────────────────────────────────┘
↓
┌─────────────────────────────────────────────────────────┐
│ ADH also activates UT-A1/A3 in IMCD │
│ → Urea recycled from collecting duct → medulla │
│ → Adds ~600 mOsm to inner medullary interstitium │
└────────────────────────┬────────────────────────────────┘
↓
┌─────────────────────────────────────────────────────────┐
│ RESULT: Concentrated urine ~1200 mOsm │
│ Small volume: 0.2–0.5 mL/min │
└─────────────────────────────────────────────────────────┘
PART 10: Dilute Urine Formation (No ADH)
STIMULUS: High water intake → ↓ plasma osmolality
↓
ADH secretion SUPPRESSED
↓
AQP-2 channels remain in cytoplasm (not inserted into membrane)
↓
Collecting duct IMPERMEABLE to water
↓
TAL continues to pump NaCl OUT → tubular fluid dilutes to ~100 mOsm
↓
Dilute fluid passes through distal tubule and collecting duct
WITHOUT water being reabsorbed (membrane impermeable)
↓
Large volume of hypotonic urine excreted (~50–100 mOsm, up to 20 mL/min)
Note: Even during water diuresis, the medullary gradient still exists (~500 mOsm), but it is less steep because urea recycling and NKCC2 stimulation are both reduced. - Medical Physiology (Boron & Boulpaep)
PART 11: Clinical Correlations
| Condition | Mechanism Disrupted | Effect on Urine |
|---|---|---|
| Central Diabetes Insipidus | No ADH secreted | Dilute polyuria (50-200 mOsm) |
| Nephrogenic Diabetes Insipidus | V2 receptor or AQP-2 defect | Dilute polyuria despite high ADH |
| Loop diuretics (Furosemide) | Block NKCC2 in TAL → no single effect | Reduces medullary gradient; dilute urine |
| SIADH | Excess ADH → too much water retention | Hyponatremia; concentrated urine |
| Renal medullary disease | Destroys medullary architecture | Impaired concentrating ability |
| High medullary blood flow | Washes out medullary gradient | Reduced concentrating ability |
| Low protein diet | Less urea available for recycling | Reduced inner medullary osmolality |
Summary in One Sentence
The kidney concentrates urine by using the countercurrent multiplier (active NaCl pumping from the water-impermeable thick ascending limb) to build a corticomedullary osmotic gradient of up to 1200 mOsm/L, which is preserved by countercurrent exchange in the vasa recta, and then exploited by ADH-driven water reabsorption in the collecting duct, with urea recycling amplifying the inner medullary component of that gradient.
Sources: Guyton and Hall Textbook of Medical Physiology, 14th ed. | Medical Physiology (Boron & Boulpaep) | Costanzo Physiology, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.