Act as a professional dental histology professor and give me a detailed answer for cementogenesis for a bds 1 year atudent
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have excellent content from multiple textbook sources. Let me compile the comprehensive, professor-level answer on cementogenesis for a BDS 1st year student.
Cementogenesis - Formation of Cementum
Dental Histology | BDS 1st Year
1. Definition
Cementogenesis is the process of formation and deposition of cementum on the root surface of a developing tooth. It begins after root dentin has been laid down and continues throughout the life of the tooth.
2. What is Cementum? (Quick Review)
Cementum is a specialized, mineralized connective tissue that covers the entire root surface of the tooth - from the cementoenamel junction (CEJ) at the cervical region down to the root apex. It is:
- 65% inorganic (hydroxyapatite) - similar to bone
- Contains the highest concentration of fluoride of any mineralized tissue in the body
- Avascular (unlike bone)
- Produced by cementoblasts
3. Pre-requisite: Role of Hertwig's Epithelial Root Sheath (HERS)
Before cementogenesis can begin, the root must be initiated. This is done by HERS:
- At the completion of crown formation, the inner and outer enamel epithelium at the cervical loop proliferate apically
- They fuse together to form a two-layered collar of cells - this is Hertwig's Epithelial Root Sheath (HERS)
- HERS grows apically, molding and determining the shape, number, and length of the roots
- HERS induces the adjacent ectomesenchymal cells (dental papilla) to differentiate into odontoblasts, which then lay down root dentin
- Once root dentin is deposited, HERS breaks up and disintegrates (due to penetration by blood vessels from the dental follicle)
- The fragmented epithelial remnants of HERS persist in the periodontal ligament as the Rests of Malassez (clinically important - can give rise to radicular cysts and certain odontogenic tumors)
- The disintegration of HERS exposes the newly formed root dentin surface to the dental follicle cells - this is the trigger for cementogenesis
4. Source of Cementoblasts
After HERS disintegrates, the ectomesenchymal cells of the dental follicle (dental sac) that are now in direct contact with the root dentin differentiate into cementoblasts. This is a critical point:
Cementoblasts are derived from the ectomesenchyme of the dental follicle (dental sac), NOT from epithelium.
5. Steps of Cementogenesis (Mechanism)
Step 1 - Cementoblast Differentiation
- Dental follicle cells adjacent to the exposed root dentin surface differentiate into large, cuboidal cementoblasts
- These cells resemble osteoblasts in morphology and function
Step 2 - Secretion of Cementoid (Precementum)
- Cementoblasts secrete an unmineralized organic matrix called cementoid (also called precementum)
- This matrix consists of:
- Type I collagen (intrinsic fibers)
- Non-collagenous proteins: osteopontin, bone sialoprotein, osteocalcin
- Proteoglycans
Step 3 - Mineralization
- The cementoid matrix undergoes mineralization by deposition of hydroxyapatite crystals
- Mineralization front advances away from the dentin surface
- A thin layer of unmineralized cementoid is always maintained at the outer surface (between the mineralizing front and the cementoblasts) - this is the precementum zone
Step 4 - Formation of Two Types of Cementum (see below)
Step 5 - Cementoblast Fate
- Some cementoblasts get entrapped within the mineralizing matrix and become cementocytes (cellular cementum)
- Others remain on the surface and continue secretion
- Cementocytes reside in spaces called lacunae and extend processes through canaliculi - analogous to osteocytes in bone, but the canaliculi do NOT form an interconnecting network (unlike bone)
6. Types of Cementum Formed
Five distinct types are recognized, but for BDS 1st year, focus on the two primary forms:
A. Acellular (Primary) Cementum
| Feature | Detail |
|---|---|
| Also called | Afibrillar cementum / Primary cementum |
| Location | Cervical 1/3 to 1/2 of root |
| Cementocytes | ABSENT (no entrapped cementoblasts) |
| Formation | Slow deposition; cementoblasts move away before being trapped |
| Sharpey's fibers | Predominantly present (extrinsic fibers from PDL) |
| Thickness | Thin (~20-50 μm) |
| Function | Main fiber attachment zone for periodontal ligament |
B. Cellular (Secondary) Cementum
| Feature | Detail |
|---|---|
| Also called | Secondary cementum |
| Location | Apical 1/2 to 2/3 of root (also in furcation areas) |
| Cementocytes | PRESENT in lacunae with canaliculi |
| Formation | Rapid deposition; cementoblasts get trapped |
| Sharpey's fibers | Mixed intrinsic + extrinsic fibers |
| Thickness | Thicker (~150-200 μm at apex) |
| Function | Adaptive and reparative role; compensation for tooth eruption |
Memory tip: "ACellular = Absent cells; Cellular = Contains cells"
Additional types (advanced knowledge):
- Acellular afibrillar cementum - no cells, no collagen fibers (found at CEJ, over enamel)
- Acellular extrinsic fiber cementum (AEFC) - only Sharpey's fibers, most important for attachment
- Cellular mixed fiber cementum (CMFC) - cementocytes + both fiber types (apical region)
- Cellular intrinsic fiber cementum (CIFC) - only cementocytes + intrinsic collagen
- Intermediate cementum - thin, acellular sheath around entire root
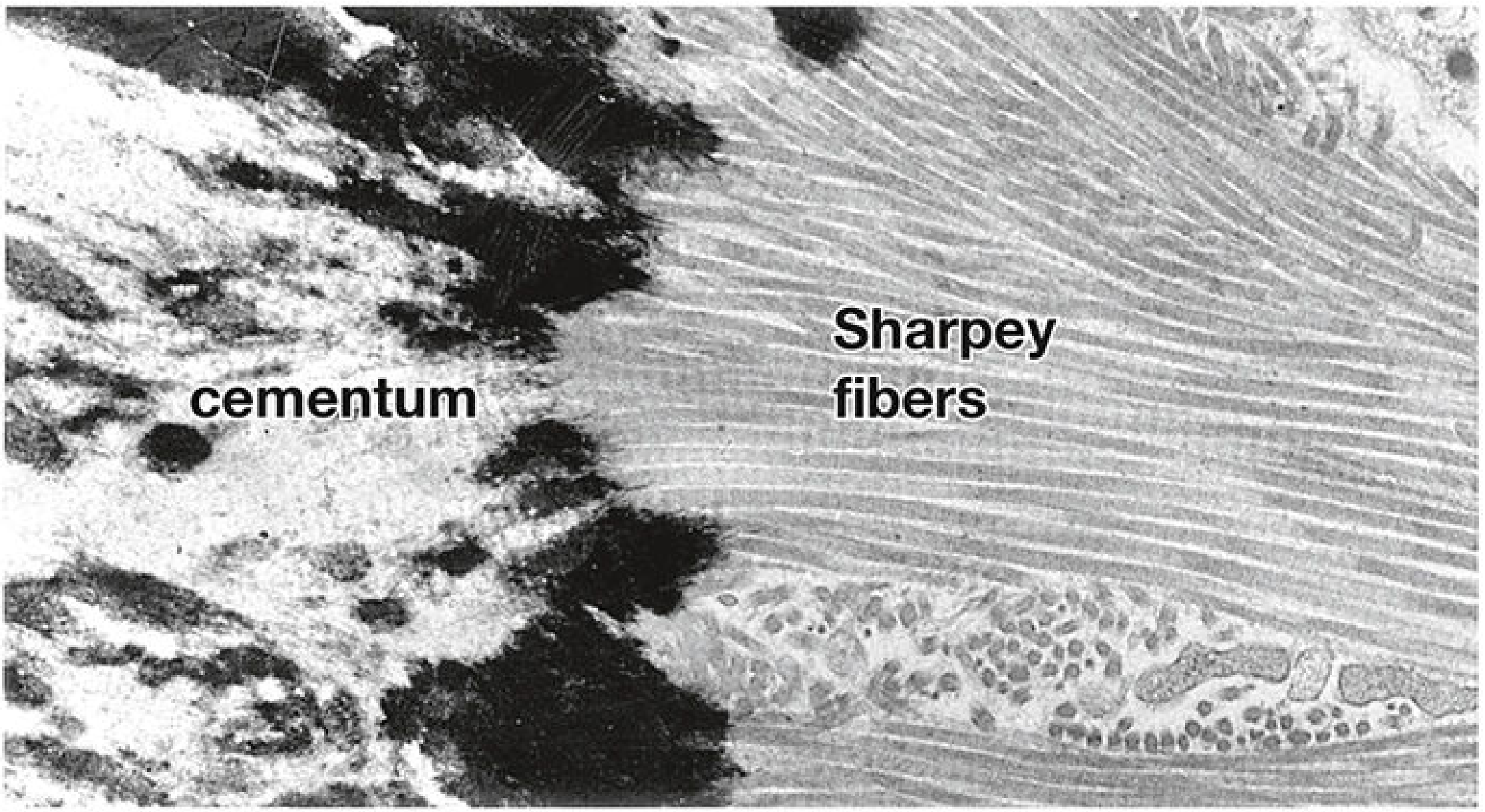
7. Sharpey's Fibers - The Attachment Mechanism
A defining feature of cementogenesis is how Sharpey's fibers are incorporated:
- The principal fibers of the periodontal ligament (PDL) are type I collagen bundles secreted by PDL fibroblasts
- One end embeds into the alveolar bone, the other end embeds into cementum - these embedded portions are Sharpey's fibers
- During cementogenesis, the mineralizing cementum engulfs these fiber bundles, anchoring the tooth to the bone
- Sharpey's fibers within cementum are mineralized; those within the PDL are not mineralized
- This arrangement forms the gomphosis joint - a fibrous joint unique to teeth
(See electron micrograph below showing Sharpey's fibers penetrating into cementum)
8. Sequence Summary: CEJ to Apex
Crown complete → HERS forms → Root dentin deposited → HERS breaks up
→ Rests of Malassez left behind → Dental follicle cells exposed to dentin
→ Differentiate into cementoblasts → Secrete cementoid → Mineralization
→ Acellular cementum (cervical) + Cellular cementum (apical) formed
→ Sharpey's fibers embedded → PDL anchors tooth to bone
9. Comparison: Cementum vs Bone vs Dentin
| Property | Cementum | Bone | Dentin |
|---|---|---|---|
| Cell | Cementoblast/cementocyte | Osteoblast/osteocyte | Odontoblast |
| % Mineral | ~65% | ~65% | ~70% |
| Vascularity | Avascular | Vascular | Avascular |
| Resorption | Resistant | Occurs normally | Resistant |
| Lacunae/canaliculi network | Irregular, no network | Regular, interconnected | Dentinal tubules |
| Regeneration | Possible (by dental follicle cells) | Readily regenerates | Limited |
10. Clinical Relevance (Know for Exams)
- Orthodontic movement: Alveolar bone is resorbed and redeposited during tooth movement, but cementum is NOT resorbed - this is why teeth can be moved orthodontically without damaging root attachment
- Rests of Malassez: HERS remnants in the PDL - can give rise to periapical (radicular) cysts due to inflammatory stimulation
- Hypercementosis: Excessive cementum deposition around the root (associated with Paget's disease, periapical inflammation)
- Ankylosis: Fusion of cementum directly to alveolar bone (no PDL space) - complicates tooth extraction
- Root sensitivity: Exposure of cementum at the cervical region (due to gingival recession) - cementum is thin here and dentinal tubules may be exposed
- Cementoma/Cemento-ossifying fibroma: Benign lesions involving cementum-like deposits
11. Key Terms Summary
| Term | Meaning |
|---|---|
| Cementogenesis | Process of cementum formation |
| Cementoblast | Cementum-forming cell (from dental follicle ectomesenchyme) |
| Cementocyte | Entrapped cementoblast within cellular cementum |
| Cementoid | Unmineralized precementum matrix |
| HERS | Hertwig's Epithelial Root Sheath - triggers root formation |
| Rests of Malassez | HERS epithelial remnants in PDL |
| Sharpey's fibers | PDL collagen fibers embedded in cementum |
| Acellular cementum | No cementocytes; cervical location; slow deposition |
| Cellular cementum | Has cementocytes; apical location; fast deposition |
| Gomphosis | Fibrous joint attaching tooth to alveolar bone via PDL |
Sources: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina & Ross) | Cummings Otolaryngology Head and Neck Surgery | Forensic Anthropology: A Comprehensive Introduction (Christensen et al.)
Deglutation
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Guyton & Hall and Scott-Brown's. Here is the full, professor-level answer on deglutition for a BDS 1st year student.
Deglutition (Swallowing)
Physiology | BDS 1st Year
1. Definition
Deglutition is the complex, coordinated neuromuscular act by which a bolus of food or liquid is transported from the oral cavity → pharynx → esophagus → stomach. It involves both voluntary and involuntary (reflex) components and requires precise coordination with respiration.
"Swallowing is a complicated mechanism, principally because the pharynx subserves both respiration and swallowing." - Guyton & Hall Textbook of Medical Physiology
2. Stages of Deglutition
Deglutition is classically divided into three stages:
| Stage | Control | Location | Duration |
|---|---|---|---|
| 1. Oral (Voluntary) | Voluntary | Oral cavity | Variable |
| 2. Pharyngeal | Involuntary (Reflex) | Pharynx | < 2 seconds |
| 3. Esophageal | Involuntary | Esophagus | 8-10 seconds |
Stage 1: Oral (Voluntary) Stage
This stage has two sub-phases:
A. Oral Preparatory Phase
- Food is received in the mouth and mixed with saliva
- Mastication (chewing) reduces food to a manageable size
- The tongue, buccal musculature, and teeth work together to form a cohesive bolus
- The soft palate is lowered to seal off the nasopharynx initially, directing the bolus toward the oropharynx
B. Oral Transport Phase
- The tongue voluntarily squeezes and rolls the bolus posteriorly
- The tongue tip elevates against the hard palate and presses backward in a wave-like motion
- The bolus is pushed through the oropharyngeal isthmus into the pharynx
- Once the bolus reaches the tonsillar pillars and posterior pharyngeal wall, swallowing becomes automatic and cannot be stopped
Key point for dentistry: This stage is why tongue posture, palatal vault shape, and missing teeth directly affect swallowing efficiency.
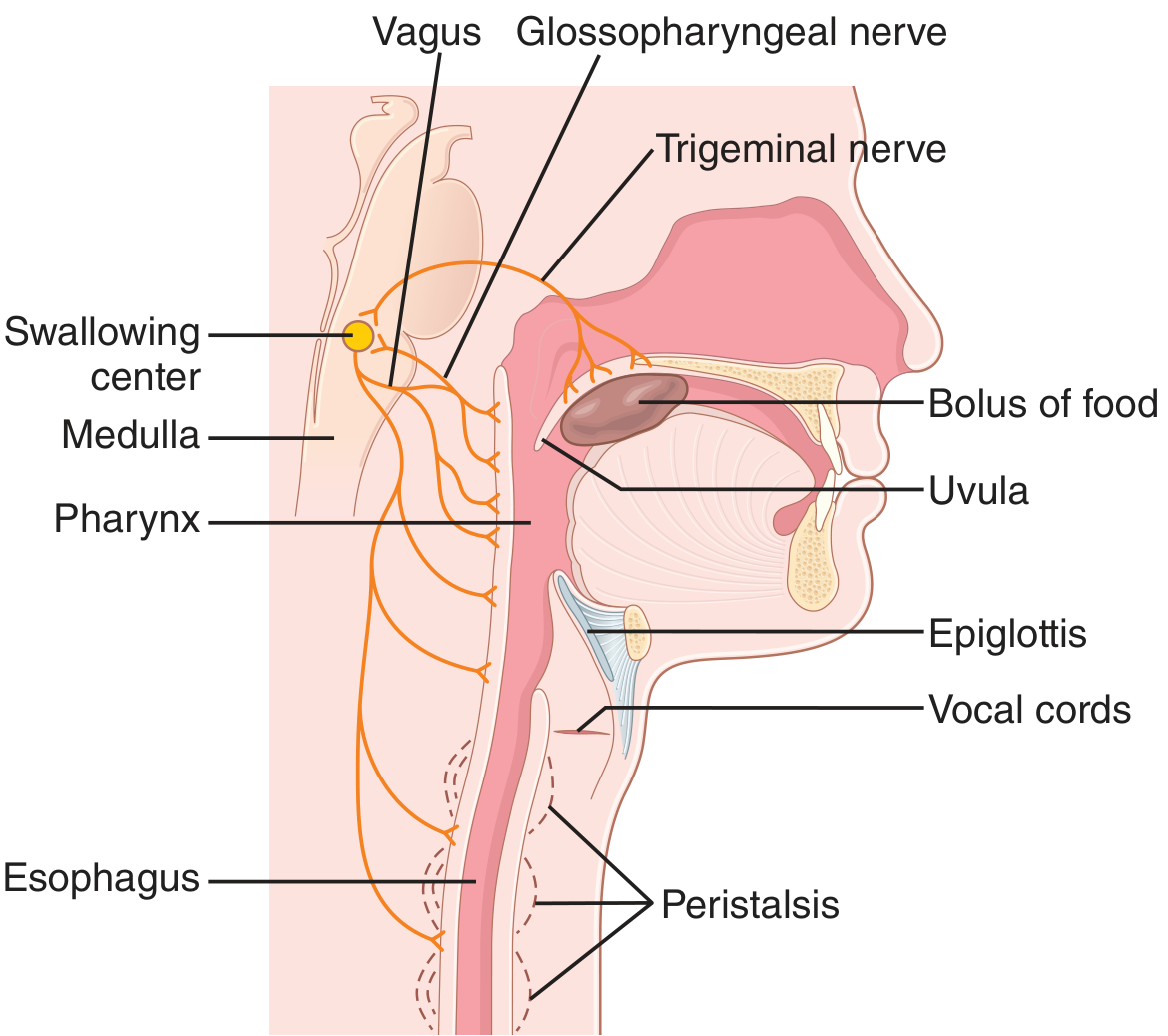
Stage 2: Pharyngeal Stage (Involuntary Reflex)
This is the most complex and most clinically important stage. It is a reflex triggered by stimulation of the posterior pharyngeal receptors.
Trigger
- The bolus stimulates epithelial swallowing receptor areas around the pharyngeal opening, especially on the tonsillar pillars
- Afferent impulses travel via CN V (trigeminal) and CN IX (glossopharyngeal) to the medulla oblongata (tractus solitarius)
- The swallowing/deglutition center in the reticular formation of the medulla and lower pons coordinates the reflex
Five Sequential Protective Events (must happen in order):
1. Nasopharyngeal Closure
- Soft palate is pulled upward by the levator and tensor veli palatini muscles
- Closes off the posterior nares → prevents food reflux into the nasal cavity
2. Palatopharyngeal Fold Adduction
- Palatopharyngeal folds are pulled medially toward each other
- Forms a narrow sagittal slit through which the bolus must pass
- Acts as a selective filter - adequately chewed food passes; large objects are impeded
- This entire process takes < 1 second
3. Laryngeal Protection (Airway Closure) - The most critical event
- Vocal cords strongly approximate (adduct) - this is the PRIMARY airway protector
- The larynx is pulled upward and anteriorly by the suprahyoid and thyrohyoid muscles
- The hyoid bone moves anteriorly
- This upward movement causes the epiglottis to swing backward (tilt) over the laryngeal inlet
- The result: three-tiered airway closure - aryepiglottic folds, ventricular folds, and true vocal folds all close
- Vocal fold adduction during swallowing averages ~2.3 seconds
4. Upper Esophageal Sphincter (UES) Opening
- The upward-forward movement of the larynx pulls open the UES (pharyngoesophageal sphincter)
- The UES = upper 3-4 cm of esophageal muscular wall, normally tonically contracted
- It relaxes to allow the bolus to enter the esophagus
- There is a transient negative pressure in the cricopharyngeal sphincter as the bolus passes
5. Pharyngeal Peristalsis
- A peristaltic wave sweeps from the superior pharynx downward through the middle and inferior pharynx
- This propels the bolus into the upper esophagus
- Entire pharyngeal stage: less than 2 seconds
Respiration is Temporarily Halted
- The swallowing center inhibits the respiratory center of the medulla
- Breathing is interrupted at any point in the respiratory cycle for < 6 seconds
- This prevents aspiration
Stage 3: Esophageal Stage (Involuntary)
The esophagus conducts food from the pharynx to the stomach. It uses two types of peristalsis:
A. Primary Peristalsis
- A continuation of the pharyngeal peristaltic wave into the esophagus
- Travels the entire length of the esophagus in 8-10 seconds
- In an upright person, gravity assists - bolus may reach the stomach in 5-8 seconds even before the wave arrives
B. Secondary Peristalsis
- Occurs if primary peristalsis fails to clear all food from the esophagus
- Initiated by distension of the esophagus by retained food
- Continues until the esophagus is completely emptied
- Involves the intrinsic myenteric plexus of the esophagus
Muscular Composition of the Esophagus
| Region | Muscle Type | Neural Control |
|---|---|---|
| Upper 1/3 (pharynx + upper esophagus) | Striated (skeletal) | CN IX, X (vagus + glossopharyngeal) |
| Lower 2/3 | Smooth muscle | Vagus + myenteric (Auerbach's) plexus |
Even if vagal input is cut, the myenteric plexus alone can sustain secondary peristalsis after a few days.
Receptive Relaxation of the Stomach
- As the peristaltic wave approaches the stomach, a wave of relaxation precedes it
- The stomach and proximal duodenum relax ahead of the bolus - this is "receptive relaxation"
- Mediated by myenteric inhibitory neurons
Lower Esophageal Sphincter (LES / Gastroesophageal Sphincter)
- Located 3 cm above the esophagogastric junction
- Normally tonically contracted at ~30 mmHg intraluminal pressure
- As the peristaltic wave arrives, receptive relaxation of the LES occurs → bolus enters the stomach
- Between swallows, the LES prevents gastroesophageal reflux (GERD)
- Failure to relax = Achalasia
3. Neural Control Summary
| Component | Details |
|---|---|
| Afferent (sensory) pathway | CN V (trigeminal), CN IX (glossopharyngeal) |
| Swallowing center | Reticular formation of medulla oblongata + lower pons |
| Efferent (motor) pathway | CN V, VII, IX, X (vagus), XII (hypoglossal) + upper cervical nerves |
| Muscles of pharynx + upper esophagus | Controlled by CN IX, X |
| Lower esophagus | Vagus + myenteric plexus |
4. Dental Relevance of Deglutition
As a BDS student, you must know how oral conditions affect swallowing:
- Tongue thrust swallowing (infantile swallowing pattern): The tongue pushes forward against the teeth during swallowing instead of pressing the palate. If this persists beyond age 4, it causes open bite and proclination of anterior teeth - a major concern in orthodontics
- Edentulous patients: Loss of teeth impairs the oral preparatory phase; inadequate bolus formation increases choking risk
- Xerostomia (dry mouth): Reduced saliva makes bolus formation difficult - impairs oral stage of swallowing
- Palatal defects (cleft palate): Incompetent soft palate closure → nasal regurgitation during swallowing
- Dysphagia: Difficulty swallowing; can result from oral cancer, post-radiation changes, neurological lesions
- TMJ disorders: Can impair mastication and thus the oral preparatory phase
5. Quick Comparison: Oral vs Pharyngeal vs Esophageal Stage
| Feature | Oral | Pharyngeal | Esophageal |
|---|---|---|---|
| Control | Voluntary | Involuntary reflex | Involuntary |
| Duration | Variable | < 2 seconds | 8-10 seconds |
| Key structure | Tongue | Larynx/epiglottis | UES + LES |
| Main function | Bolus formation + propulsion | Airway protection | Transport to stomach |
| Initiating stimulus | Conscious decision | Bolus at tonsillar pillars | Bolus entering esophagus |
6. Key Terms
| Term | Meaning |
|---|---|
| Bolus | Chewed food mass moistened by saliva |
| UES | Upper esophageal sphincter (pharyngoesophageal sphincter) |
| LES | Lower esophageal sphincter (gastroesophageal sphincter) |
| Deglutition center | In medulla oblongata - coordinates the swallowing reflex |
| Primary peristalsis | Continuation of pharyngeal wave into esophagus |
| Secondary peristalsis | Triggered by esophageal distension when primary fails |
| Achalasia | Failure of LES to relax - causes dysphagia |
| Receptive relaxation | Stomach relaxes ahead of incoming bolus |
| Rests of Malassez | (from previous lecture) - not relevant here |
| Dysphagia | Difficulty in swallowing |
Sources: Guyton & Hall Textbook of Medical Physiology (14th ed.) | Scott-Brown's Otorhinolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.