Loss of lordotic curve
Reading File
search_medical_text
loss of lordotic curve cervical lumbar spine causes clinical significance
search_medical_image
loss of lordotic curve cervical lumbar spine X-ray
GradeResponse
GradeResponse
Loss of Lordotic Curve (Cervical / Lumbar)
Normal Spinal Curvature
The spine has four natural curves:
- Cervical lordosis (concave posteriorly, ~40–60°)
- Thoracic kyphosis
- Lumbar lordosis (concave posteriorly, ~30–50°)
- Sacral kyphosis
Lordosis in the cervical and lumbar regions is essential for load distribution, shock absorption, and upright posture.
Loss of Lordosis: Definition
Also called hypolordosis or straight spine, this refers to the flattening or reversal of the normal anterior concavity. In extreme cases, the curve reverses into kyphosis (posterior convexity).
Causes
Cervical Spine
| Category | Examples |
|---|---|
| Muscle spasm | Most common acute cause (trauma, cervical strain, torticollis) |
| Degenerative disc disease | Disc height loss leads to progressive straightening |
| Cervical spondylosis | Osteophyte formation with segmental rigidity |
| Trauma | Whiplash injury, fractures |
| Ankylosing spondylitis | Progressive fusion with global flattening |
| Postural/occupational | Prolonged forward head posture (e.g., screen use) |
| Inflammatory arthritis | Rheumatoid arthritis affecting C1–C2 and lower segments |
Lumbar Spine
| Category | Examples |
|---|---|
| Muscle spasm | Protective flattening in acute disc prolapse or herniation |
| Lumbar disc herniation | Paraspinal spasm straightens the curve |
| Degenerative disc disease | Loss of disc height reduces lumbar lordosis |
| Ankylosing spondylitis | Classic "bamboo spine" with complete lordosis loss |
| Postural | Prolonged sitting, hip flexor tightness |
| Pregnancy / obesity | Can paradoxically increase OR decrease lordosis |
| Spondylolisthesis | Vertebral slippage alters sagittal balance |
Clinical Presentation
- Pain: Neck or low back pain, often worsened with extension
- Stiffness: Reduced range of motion (normal cervical flexion ~45°, extension ~55°; normal lumbar flexion 40–60°, extension 20–35°) (Bailey and Love's, p. 530)
- Neurological symptoms: Radiculopathy or myelopathy if neural foramina or spinal canal are compromised
- Postural changes: Forward head posture (cervical), flat back appearance (lumbar)
Radiological Findings
On lateral X-ray, loss of lordosis appears as straightening or reversal of the expected curve. Below is a series demonstrating cervical lordosis loss and its correction:
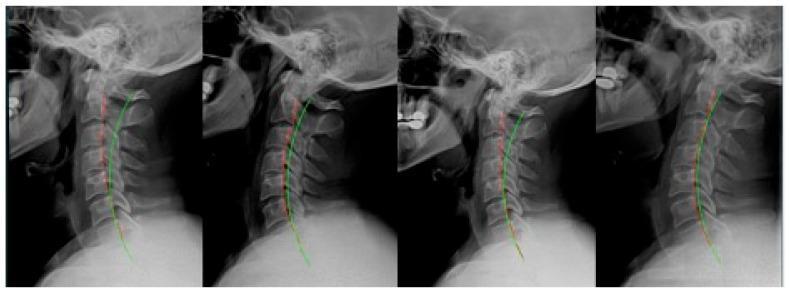
Lateral cervical spine series: (1) pre-treatment showing loss of lordosis, (2) post-initial correction with improved curve, (3) regression after MVC trauma, (4) restoration after rehabilitative intervention. Green arc = ideal lordosis; red dashed line = actual posterior vertebral alignment.
Diagnostic Approach
- Plain X-ray (lateral view) — first-line; measures Cobb angle or C2–C7 angle
- MRI — evaluates disc pathology, neural compression, spinal cord signal change
- CT scan — bony detail in trauma or advanced spondylosis
- Electromyography (EMG/NCS) — if radiculopathy suspected
Management
Conservative
- Physical therapy: Core strengthening, cervical retraction exercises, postural correction
- NSAIDs / muscle relaxants: Acute spasm and pain relief
- Heat/cold therapy, TENS, traction
- Chiropractic / manual therapy: Evidence supports short-term pain relief
Interventional
- Epidural steroid injections: For radicular pain secondary to disc pathology
- Facet joint injections / medial branch blocks
Surgical
- Reserved for refractory cases with progressive neurological deficit, instability, or failed conservative management
- Options: anterior cervical discectomy and fusion (ACDF), lumbar fusion, osteotomy (for rigid deformities, e.g., ankylosing spondylitis)
Clinical Significance
Loss of lordosis is often a radiological finding rather than a diagnosis — its significance depends on the underlying etiology. Acute loss due to muscle spasm is typically reversible. Chronic loss secondary to degenerative disc disease or inflammatory arthropathy carries a higher risk of progressive disability, adjacent segment disease, and sagittal imbalance.
How much time it takes for recovery
search_medical_text
loss of lordosis recovery time prognosis treatment duration
GradeResponse
Recovery time depends heavily on the underlying cause. There is no single timeline — here is a breakdown:
Recovery Timelines by Cause
| Cause | Expected Recovery |
|---|---|
| Acute muscle spasm (most common) | Days to 2–4 weeks with rest, NSAIDs, and heat |
| Whiplash / cervical strain | 6–12 weeks with physiotherapy; some cases persist 3–6 months |
| Lumbar disc herniation | 4–6 weeks (most improve conservatively); up to 3 months for full recovery |
| Cervical/lumbar spondylosis | Months to years; management is ongoing — structural loss may be permanent |
| Postural loss of lordosis | 8–12 weeks of targeted physiotherapy; highly reversible if caught early |
| Ankylosing spondylitis | Chronic, progressive — lordosis loss is largely irreversible without early intervention |
| Post-surgical | 3–6 months depending on procedure |
Factors That Predict Faster Recovery
According to Diagnosis and Treatment of Low Back Pain (p. 47), patients recover more quickly when they have:
- Lower initial pain intensity (≤7/10)
- Shorter symptom duration (less than 5 days before starting treatment)
- No prior episodes of the same condition
Conversely, pain >7/10, symptoms lasting more than 5 days, and recurrent episodes are associated with slower recovery.
General Principles
- Acute / postural cases: Most reversible. Consistent physiotherapy (core strengthening, posture correction, stretching) over 6–12 weeks produces significant improvement.
- Degenerative cases: The pain and spasm component improves (weeks to months), but the structural loss of lordosis from disc height reduction or facet changes may be permanent or only partially correctable.
- Consistency matters: Irregular physiotherapy dramatically extends recovery time.
- Red flags (progressive neurological deficit, bowel/bladder involvement) require urgent evaluation and do not follow standard recovery timelines.
Bottom line: For most acute and postural causes, expect 4–12 weeks of active treatment for meaningful recovery. Degenerative and inflammatory causes require long-term management rather than a defined "recovery" endpoint.
This is a shared conversation. Sign in to Orris to start your own chat.