Complete explanation of mechanical ventilation
Reading File
Finding Sources
Searching PubMed
"mechanical ventilation" AND "lung protective"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative sources. Let me compile the complete explanation.
Mechanical Ventilation: Complete Explanation
1. Definition and Goals
Mechanical ventilation is a life-sustaining therapy in which a mechanical device (the ventilator) provides partial or full support for patients with respiratory failure. The main goals are to:
- Maintain adequate gas exchange (oxygenation and CO2 elimination)
- Rest the respiratory muscles and decrease the oxygen cost of breathing
- Minimize iatrogenic consequences - including hyperinflation, infection, oxygen toxicity, respiratory muscle injury, and ventilator-induced lung injury (VILI)
Modern strategies accept that targeting perfectly normal blood gases is not always preferred. A conservative oxygen target (PaO2 70-100 mmHg or SpO2 94-98%) is at least as good as aggressive therapy (PaO2 up to 150 mmHg). Further reducing PaO2 to 55-75 mmHg or SpO2 goal of 90% is not beneficial.
- Goldman-Cecil Medicine, p. 1061
2. Physiological Basis: How Ventilation Works
Oxygenation
Three main strategies improve oxygenation:
- Increasing FiO2 - raises the partial pressure of oxygen available for hemoglobin transport. FiO2 >50% is generally tolerated but risks oxygen toxicity and absorptive atelectasis.
- Increasing mean airway pressure - via increasing PEEP, driving pressure, or adjusting the I:E ratio to raise inspiratory time. Plateau pressure must be limited to minimize barotrauma and VILI.
- Recruitment maneuvers (RM) - transient increases in airway pressure to re-open collapsed alveoli, followed by increased PEEP to prevent recollapse. Risk: barotrauma and transient decreased cardiac output.
Ventilation (CO2 Elimination)
Alveolar ventilation = minute ventilation (RR × tidal volume) - dead space. To increase ventilation: increase tidal volume or respiratory rate.
- Current Surgical Therapy 14e, p. 1575
3. Types of Mechanical Ventilation
3a. Invasive vs. Noninvasive
| Feature | Invasive | Noninvasive (NIV) |
|---|---|---|
| Interface | Endotracheal tube or tracheostomy | Tight-fitting face/nasal mask |
| Full support | Yes | Partial |
| Airway protection | Yes | No |
| Risk | VAP, sedation-related | Skin breakdown, less aspiration protection |
Positive-pressure ventilation is the basis of both types. Gas is delivered to the lung under positive pressure, in contrast to the negative pressure used in "iron lungs."
4. Modes of Mechanical Ventilation
4a. Controlled Ventilation (CMV)
- A preset tidal volume (volume-controlled) or preset inspiratory pressure (pressure-controlled) is delivered at a predetermined rate and insufflation time, regardless of patient effort.
- Used in heavily sedated or paralyzed patients and in severe ARDS or shock requiring full support.
- Disadvantage: Rapid respiratory muscle atrophy from disuse; altered gas distribution from supine position and lack of diaphragm activity.
4b. Assist-Control Ventilation (AC)
- Most commonly used mode in ICUs.
- The ventilator delivers full preset breaths whenever triggered - either by the patient's inspiratory effort or by the ventilator timer if no patient effort occurs in the set interval.
- Every breath (patient-triggered or machine-triggered) receives the full preset support.
- Advantage: Low work of breathing; tidal volume is guaranteed.
- Disadvantage: Risk of breath stacking and respiratory alkalosis if patient over-breathes.
4c. Synchronized Intermittent Mandatory Ventilation (SIMV)
- The ventilator delivers a mandatory breath rate and also permits the patient to take additional spontaneous variable breaths above the set rate.
- Mandatory breaths are synchronized with the patient's inspiratory effort to minimize breath stacking.
- If the patient does not trigger, the ventilator delivers mandatory breaths at the set rate.
- Spontaneous breaths between mandatory breaths are unsupported (or can be supported with pressure support).
4d. Spontaneous Modes (Pressure Support Ventilation - PSV)
- No mandatory breaths - respiratory rate is entirely patient-determined.
- The ventilator provides a set pressure boost to augment each patient-initiated breath.
- Requires intact respiratory drive; apnea alarms and back-up rates are mandatory.
- Used for patient comfort and to assist with ventilator liberation (weaning).
4e. Bilevel Ventilation (APRV / BiLevel)
Uses two pressure levels (PEEP-high and PEEP-low) over two time periods (T-high and T-low), with spontaneous breathing allowed at both pressure levels. This is illustrated below:
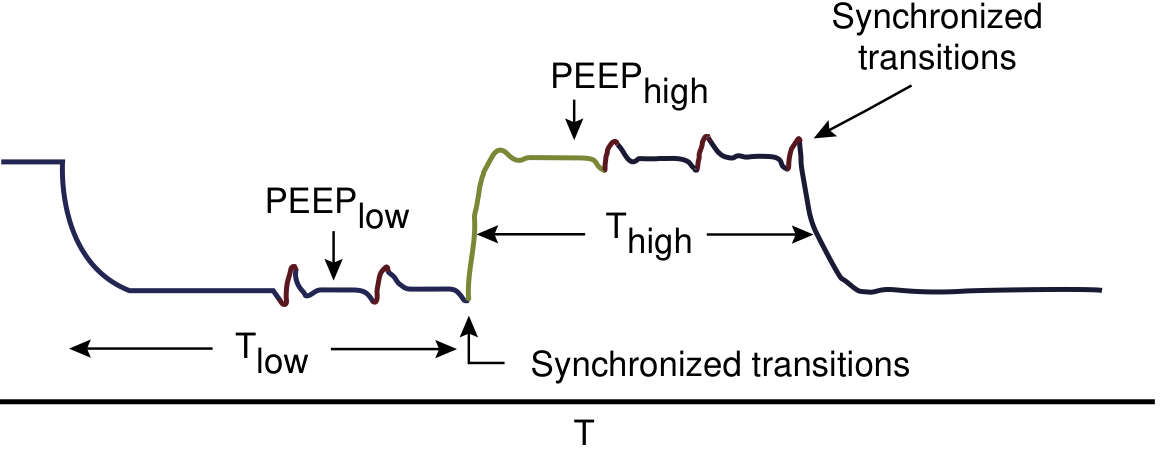
Current Surgical Therapy 14e, p. 1576
5. Volume vs. Pressure Breaths
| Feature | Volume-Controlled | Pressure-Controlled |
|---|---|---|
| Primary target | Tidal volume guaranteed | Inspiratory pressure set |
| Variable | Pressure (can rise unpredictably) | Tidal volume (varies with compliance) |
| VILI risk | Higher if compliance drops | Lower (pressure limited) |
| Clinical use | Most common initially | Preferred in ARDS, children |
Neither is definitively superior to the other. In both types, plateau pressure (measured during an inspiratory hold) should be monitored - values >30 cmH2O are associated with VILI.
6. Key Ventilator Settings
| Parameter | Target / Notes |
|---|---|
| Tidal volume (VT) | 6-8 mL/kg ideal body weight (IBW) |
| Respiratory rate (RR) | 12-20/min; adjusted to target PaCO2 |
| FiO2 | Start at 1.0, wean to lowest tolerated (target SpO2 94-98%) |
| PEEP | 5-10 cmH2O standard; higher in ARDS |
| Plateau pressure | <30 cmH2O; <16 cmH2O associated with lowest PPC risk |
| Driving pressure | Plateau - PEEP; target <15 cmH2O |
| I:E ratio | Usually 1:2; may be reversed in ARDS |
| Flow rate | Adjusted to allow full exhalation and prevent auto-PEEP |
- Murray & Nadel's Textbook of Respiratory Medicine; Current Surgical Therapy 14e
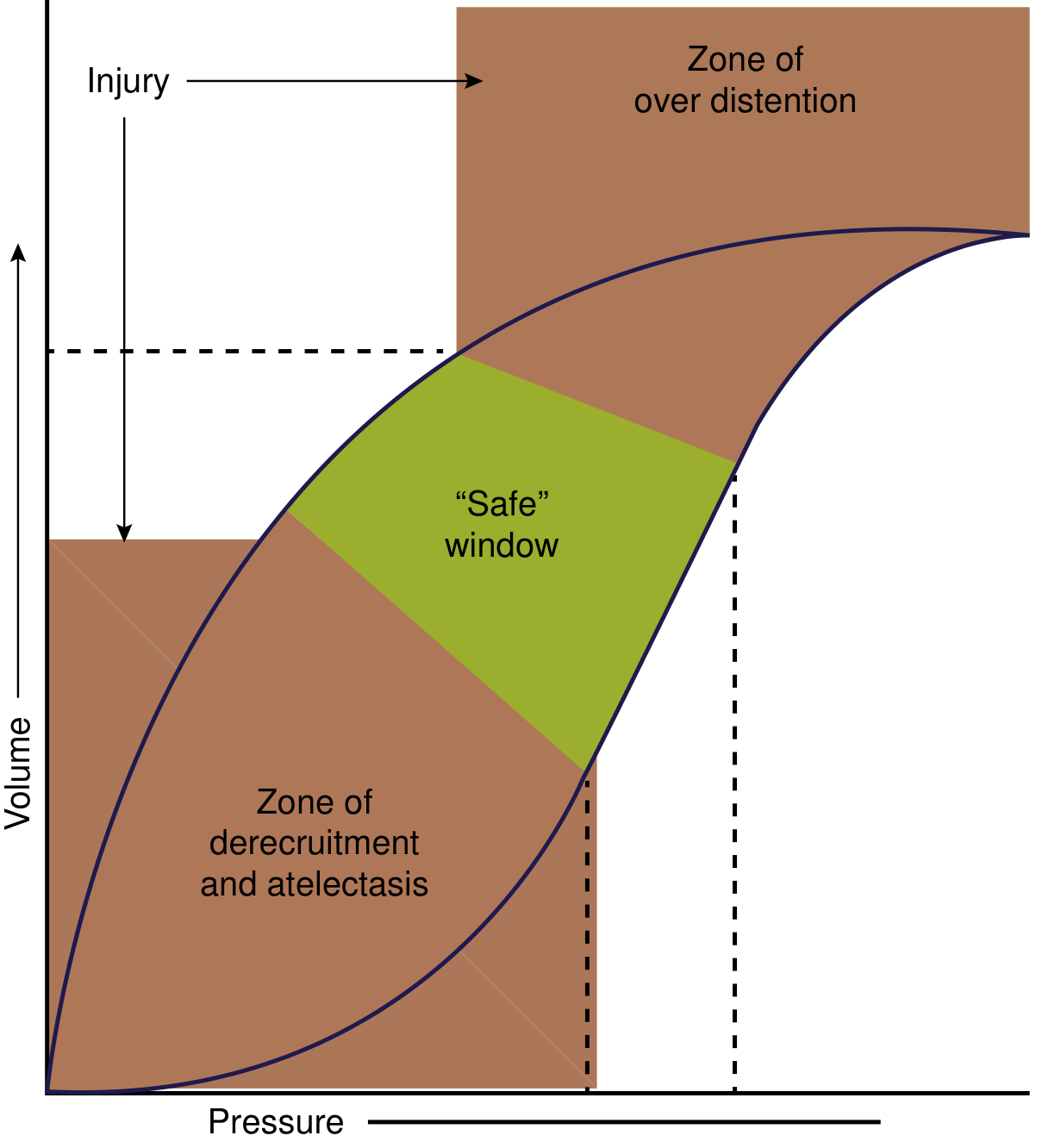
7. Pressure-Volume Curve and the "Safe Window"
The pressure-volume (P-V) curve shows two hazard zones:
-
Zone of overdistension (barotrauma/volutrauma): Too high a pressure or volume stretches and ruptures alveoli.
-
Zone of derecruitment and atelectasis: Too little pressure allows alveoli to collapse.
-
Safe window (green): The clinical goal - use sufficient PEEP to keep alveoli open while using small tidal volumes to stay below the overdistension threshold.
-
Current Surgical Therapy 14e, Fig. 1
8. Ventilator-Induced Lung Injury (VILI)
VILI has four main mechanisms:
| Mechanism | Definition |
|---|---|
| Barotrauma | Injury from excess airway/alveolar pressure |
| Volutrauma | Diffuse alveolar injury from alveolar overdistension |
| Atelectrauma | Injury from repeated cycles of alveolar collapse and recruitment |
| Biotrauma | Release of local inflammatory mediators, causing systemic injury |
Prevention: Lung-protective ventilation with VT 6 mL/kg IBW, plateau pressure <30 cmH2O, appropriate PEEP to prevent derecruitment.
9. Auto-PEEP and Dynamic Hyperinflation
Auto-PEEP is the difference between alveolar pressure and airway opening pressure at end-expiration. It develops when there is insufficient time for complete exhalation, leading to air trapping (dynamic hyperinflation).
Major determinants:
- High minute ventilation
- Increased expiratory airway resistance (e.g., COPD, asthma)
- Increased respiratory system compliance
- Short expiratory time
Consequences: Reduced venous return, hemodynamic compromise, false-low compliance readings, and increased work of breathing to trigger the ventilator.
Detection: Expiratory hold maneuver - pressure at airway opening during prolonged expiration reveals true alveolar pressure.
Management: Reduce respiratory rate, increase expiratory time (lower I:E), reduce tidal volume, treat bronchospasm.
- Goldman-Cecil Medicine, p. 1063
10. Hemodynamic Effects of Positive-Pressure Ventilation
Positive pressure has complex cardiovascular effects:
-
Increases intrathoracic pressure → decreases venous return → reduced preload → may drop cardiac output
-
At high lung volumes: Compresses alveolar vessels → increased pulmonary vascular resistance → right ventricular strain → acute cor pulmonale
-
ARDS patients tolerate relatively higher PEEP because low lung compliance limits the transmission of airway pressure to pleural pressure
-
COPD patients tolerate lower PEEP because high compliance transmits more pressure to pleura
-
Obese patients tolerate PEEP ~8 cmH2O higher than non-obese patients due to higher baseline intrathoracic pressures from abdominal/chest wall load
-
Goldman-Cecil Medicine, p. 1063
11. Disease-Specific Ventilation Strategies
11a. ARDS (Acute Respiratory Distress Syndrome)
- Lung-protective ventilation: VT 6 mL/kg IBW, plateau pressure <30 cmH2O
- Higher PEEP to prevent derecruitment; titrate using PEEP-FiO2 tables
- Prone positioning for moderate-severe ARDS (PaO2/FiO2 <150): improves dorsal recruitment
- Permissive hypercapnia acceptable to avoid volutrauma
- Neuromuscular blockade in severe early ARDS to reduce patient-ventilator dyssynchrony and VILI
11b. COPD / Status Asthmaticus
- Avoid dynamic hyperinflation - use low respiratory rates (10-12/min), smaller tidal volumes, long expiratory times
- Accept permissive hypercapnia (controlled hypoventilation)
- PEEP should be set at 80-85% of auto-PEEP to reduce inspiratory trigger work without worsening hyperinflation
- NIV preferred initially to avoid intubation
11c. Neuromuscular Disease
- VT 6-8 mL/kg, rates slightly below spontaneous, 5-10 cmH2O PEEP
- Pressure-limited ventilation acceptable if pressure difference (Pi - Pe) is at least 8-10 cmH2O
- NIV preferred when possible; failed NIV (especially with bulbar involvement) requires intubation
12. Noninvasive Ventilation (NIV)
NIV delivers positive pressure through a mask (face, nasal, or helmet). Two main modes:
| Mode | Description | Indication |
|---|---|---|
| CPAP (Continuous Positive Airway Pressure) | Single fixed pressure throughout breathing cycle | OSA, cardiogenic pulmonary edema, post-extubation |
| BiPAP (Bilevel Positive Airway Pressure) | Higher IPAP on inspiration, lower EPAP on expiration | COPD exacerbation, hypercapnic respiratory failure, NMD |
Advantages over invasive MV: No ETT-associated complications, no need for sedation, patient can eat/speak, shorter ICU stay.
Contraindications/failure predictors: Hemodynamic instability, inability to protect airway, severe bulbar dysfunction, high secretion burden, uncooperative patient, facial trauma.
13. Monitoring During Mechanical Ventilation
Key monitored parameters:
- Continuous: ECG, pulse oximetry, capnometry (EtCO2)
- Airway pressures: Peak, plateau, mean, and PEEP - measured continuously
- Tidal volumes: Inhaled and exhaled (mechanical + spontaneous)
- FiO2: Should match set values
- Chest radiograph: To confirm ETT position, detect pneumothorax, pulmonary edema
- Arterial blood gas (ABG): Via arterial line for accurate pH, PaO2, PaCO2
- Fluid balance: Urine output monitoring
Interpreting pressure changes:
-
Rising plateau pressure = worsening compliance
-
Rising peak + hypotension = suspect pneumothorax
-
Rising peak only (plateau stable) = increased airway resistance (secretions, bronchospasm, ETT obstruction)
-
Dynamic hyperinflation = drop in BP + rising plateau → disconnect from ventilator to release trapped gas
-
Morgan & Mikhail's Clinical Anesthesiology, p. 2538
14. Complications of Mechanical Ventilation
Pulmonary
| Complication | Notes |
|---|---|
| VILI (Barotrauma/Volutrauma/Atelectrauma) | See Section 8 |
| Pneumothorax | Can rapidly become tension; monitor airway pressure trends |
| Oxygen toxicity | FiO2 >0.6 for prolonged periods → alveolar injury |
| Auto-PEEP / Dynamic hyperinflation | See Section 9 |
Infectious
Ventilator-Associated Pneumonia (VAP):
- Defined as pneumonia ≥48 hours after initiating mechanical ventilation
- Occurs in up to 15% of ventilated patients; ~50% mortality when it occurs
- Pathogens: S. aureus, Pseudomonas aeruginosa, gram-negative enteric rods (MRSA in select patients)
- Empiric treatment: IV beta-lactam (piperacillin-tazobactam, cefepime) ± MRSA coverage (vancomycin or linezolid)
- Treatment duration: 7 days when possible
VAP Prevention Bundle:
- Head-of-bed elevation 30-45° (70% VAP reduction vs. supine)
- Specialized ETT with suction port above cuff (50% VAP reduction)
- Minimize ventilator circuit tubing changes
- Hand hygiene before handling circuits
- Daily sedation interruption and readiness-for-extubation assessment
- Oral/dental care
Cardiovascular
- Hemodynamic compromise in up to 40% of emergency intubations
- Decreased venous return, cardiac output, and BP from high intrathoracic pressures
Extrathoracic
-
GI stress ulcers and bleeding (requires prophylaxis with H2 blockers or PPIs)
-
Deep venous thrombosis / pulmonary embolism (requires pharmacologic or mechanical DVT prophylaxis)
-
Delirium and sleep disruption
-
ICU-acquired weakness (ICUAW) from prolonged sedation, paralysis, disuse atrophy
-
Harrison's Principles of Internal Medicine, 22e, p. 2351
15. Liberation (Weaning) from Mechanical Ventilation
The term "weaning" implies gradual withdrawal, which can unnecessarily extend ventilation by up to 40%. The preferred framework is active daily assessment for liberation readiness.
15a. Readiness Criteria (Daily Screening)
- Underlying cause of respiratory failure is improving or resolved
- Patient is awake, alert, off or on minimal sedation
- FiO2 ≤ 0.5, PEEP < 8 cmH2O, SpO2 > 88%
- Hemodynamically stable (no vasopressors or minimal doses)
- Manageable secretions with adequate cough
- pH > 7.25
15b. Spontaneous Breathing Trial (SBT)
If readiness criteria are met, perform an SBT:
- Set pressure support to 5-7 cmH2O (to compensate for ETT resistance)
- Patient breathes spontaneously for 30-120 minutes
- Passes SBT if: Comfortable, SpO2 stable, RR <35/min, HR and BP stable, no distress or diaphoresis
15c. Rapid Shallow Breathing Index (RSBI)
RSBI = Respiratory Rate (f) / Tidal Volume (VT in liters), measured during T-piece breathing
- RSBI < 105: Predicts successful extubation (sensitivity ~97%)
- RSBI > 105: Predicts weaning failure
15d. Additional Weaning Parameters
| Parameter | Favorable Value |
|---|---|
| SpO2 on FiO2 40-50% with PEEP <5 | ≥90% |
| Negative inspiratory force (NIF) | < -20 to -25 cmH2O |
| Vital capacity | >10 mL/kg |
| Minute ventilation | <10 L/min |
| RSBI | <105 |
15e. Methods of Weaning (when gradual withdrawal needed)
- Daily SBT (T-piece or low PSV): Most evidence-based. Pass → extubate.
- Gradual PSV reduction: Decrease pressure support by 2-4 cmH2O increments until 5-7 cmH2O tolerated.
- SIMV rate reduction: Progressively lower mandatory rate. Now considered least preferred (slower weaning).
15f. Tracheostomy
-
Consider when a patient has required intubation for ≥ 2 weeks or is predicted to require prolonged ventilation.
-
Early tracheostomy (<1 week) is generally no better than waiting 10-15 days.
-
Allows weaning while maintaining airway access, reducing sedation requirements, and enabling communication.
-
Harrison's Principles of Internal Medicine, 22e; Morgan & Mikhail's Clinical Anesthesiology, p. 2539
16. Recent Evidence (2024-2026)
Two recent systematic reviews update established understanding:
-
Intraoperative ventilation (PMID: 40133080, Anaesthesia, 2025): Network meta-analysis of RCTs found that lung-protective intraoperative ventilation strategies remain superior, though optimal combinations of VT, PEEP, and recruitment maneuvers are still debated.
-
Mechanical power and VILI (PMID: 41270941, Respir Med, 2025): Mechanical power (MP) - the total energy delivered to the lung per minute (encompassing pressure, tidal volume, flow, and rate) - is emerging as a more unified index of VILI risk than individual parameters. Limiting MP may reduce VILI beyond traditional lung-protective settings alone.
Summary Table: Quick Reference
| Topic | Key Points |
|---|---|
| Goals | Gas exchange, rest muscles, minimize VILI |
| Primary mode | Assist-control (volume or pressure) |
| Lung-protective VT | 6 mL/kg IBW |
| Plateau pressure | <30 cmH2O |
| PEEP | 5-10 cmH2O standard; titrate in ARDS |
| ARDS strategy | Low VT, high PEEP, prone, permissive hypercapnia |
| COPD strategy | Low RR, long expiratory time, prevent auto-PEEP |
| VAP prevention | HOB ≥30°, daily SBT, suction port ETT |
| Liberation | Daily screening + SBT; RSBI <105 predicts success |
| Tracheostomy | Consider after ≥2 weeks of intubation |
Sources: Goldman-Cecil Medicine 26e | Murray & Nadel's Textbook of Respiratory Medicine | Harrison's Principles of Internal Medicine 22e | Current Surgical Therapy 14e | Morgan & Mikhail's Clinical Anesthesiology 7e | Barash Clinical Anesthesia 9e | PMID 40133080 (Anaesthesia, 2025) | PMID 41270941 (Respir Med, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.