In which condition or which pattern of ecg required to give aspirin 300, clopidogrel 300, atorvastatin 80
Reading File
Finding Sources
Finding Sources
Searching the Web
aspirin 300 clopidogrel 300 atorvastatin 80 loading dose ECG indication STEMI NSTEMI
Finding Sources
Finding Sources
Searching Images
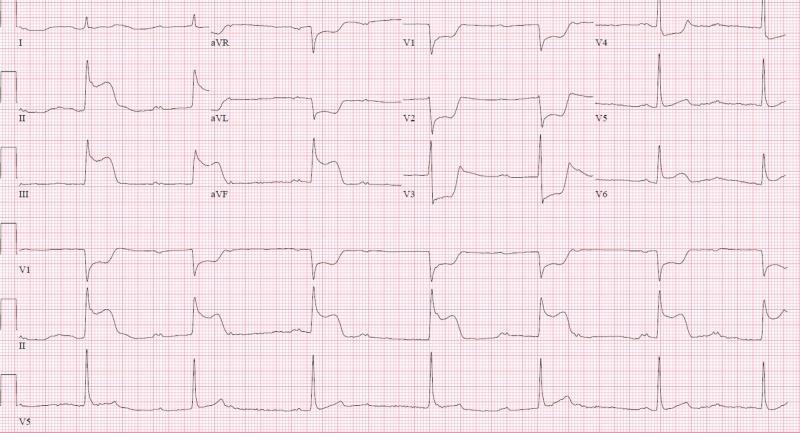
STEMI ECG ST elevation myocardial infarction pattern
Here is a comprehensive answer:
When to Give Aspirin 300 mg + Clopidogrel 300 mg + Atorvastatin 80 mg
This triple combination is the standard loading regimen for Acute Coronary Syndrome (ACS) — given as soon as the diagnosis is made, based on clinical presentation plus ECG findings.
ECG Patterns That Trigger This Regimen
1. STEMI — ST-Elevation Myocardial Infarction
The primary indication. Key ECG criteria:
- ST elevation ≥ 1 mm in ≥ 2 contiguous limb leads (II, III, aVF / I, aVL)
- ST elevation ≥ 2 mm in ≥ 2 contiguous precordial leads (V1–V6)
- New Left Bundle Branch Block (LBBB) — treated as STEMI equivalent
- Tombstone pattern — massive convex ST elevation merging with T-wave (LAD occlusion)
- Shark-fin pattern — monophasic QRS-ST-T complex, indicates extensive ischemia
- Reciprocal ST depression in opposite leads confirms the diagnosis

2. NSTEMI — Non-ST-Elevation MI
- ST depression ≥ 0.5–1 mm (horizontal or downsloping) in ≥ 2 contiguous leads
- T-wave inversion (deep, symmetrical) — especially in V1–V4 (Wellens pattern = critical LAD stenosis)
- Dynamic ECG changes — ST/T changes that evolve with symptoms
- Troponin is elevated (differentiates from unstable angina)
3. Unstable Angina (UA)
- ECG may show transient ST depression or T-wave changes during pain
- Troponin is negative, but the same antiplatelet loading applies
The Rationale for Each Drug
| Drug | Loading Dose | Mechanism | Why Given |
|---|---|---|---|
| Aspirin | 300 mg (chewed/crushed) | Irreversibly inhibits COX-1 → blocks TXA₂ → reduces platelet aggregation | Immediate antiplatelet effect; reduces mortality in ACS |
| Clopidogrel | 300 mg (or 600 mg pre-PCI) | P2Y12 ADP receptor antagonist → blocks ADP-mediated platelet activation | Dual antiplatelet therapy (DAPT) with aspirin; CURE trial showed 18–20% reduction in CV events |
| Atorvastatin | 80 mg | HMG-CoA reductase inhibitor → pleiotropic effects: plaque stabilization, anti-inflammatory, endothelial protection | High-intensity statin reduces recurrent events; given regardless of baseline LDL |
Key Points on Dosing
- Aspirin 300 mg: Given STAT to all ACS patients; chewed for faster absorption. Maintenance = 75–100 mg/day indefinitely.
- Clopidogrel 300 mg: Used when going for fibrinolysis (thrombolytics) or medical management. If going for primary PCI, prefer 600 mg loading dose for faster platelet inhibition.
- In patients ≥75 years receiving fibrinolysis → use 75 mg (not 300 mg) to reduce bleeding risk.
- Atorvastatin 80 mg: Started as early as possible regardless of cholesterol levels; the default statin for all ACS cases per NICE and most guidelines.
Summary: The "Triple Therapy" ECG Trigger
Give Aspirin 300 + Clopidogrel 300 + Atorvastatin 80 whenever the ECG shows:
- ST elevation in ≥ 2 contiguous leads (STEMI), OR
- New LBBB (STEMI equivalent), OR
- ST depression / T-wave inversion with symptoms (NSTEMI/UA)
This is standard ACS management per NICE guideline NG185, ACC/AHA, and ESC guidelines. The regimen is initiated in the ED/ambulance as soon as ACS is confirmed or highly suspected — you do not wait for troponin results to start antiplatelet therapy.
Create a quick reference ECG guide for STEMI vs. NSTEMI patterns
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.